UNIT 12 HUMAN REPRODUCTION
UNIT 12: HUMAN REPRODUCTION
Key Unit Competence
Explain the role of hormones in human reproduction, stages of pregnancy and foetal
development.
Learning objectives
By the end of the lesson, I should be able to:
– Define menstrual cycle
– Describe main events of menstrual cycle
– Describe the hormonal changes involved in menstrual cycle.
– Distinguish oestrous and menstrual cycle
– Describe how mammals mate
– Explain how a sperm enters and fertilizes an ovum and how only one sperm
fertilizes an ovum.
– Outline the technique of in vitro fertilization (IVF).
– Explain the physiological changes in females during pregnancy.
– Explain how placenta forms and discuss its functions.
– Explain the gestation period birth.
– Describe the main stages of birth.
– Discuss the significance of parental care in mammals
– Explain how twins and multiple birth arise.
– Describe the main types of birth control techniques.
– Discuss advantages and disadvantages of different birth control methods.– State the causes and the ways of prevention of STIS and HIV.
Introductory activity
Human beings grow and develop from childhood to adulthood, during such
period of growth and development, there are changes in some parts of body
which may occur physiologically, physically and even psychologically. These
changes prepare individual adulthood to reproduce. Different researches
indicated these changes to be coordinated by different types of hormones.
1. Describe the hormones involved during such period of changes in
body parts?
2. Discuss the significance of these hormones you have mentioned above
during such period of changes.
3. Describe the role of hormones involved during menstrual cycle andbirth.
12.1 Menstrual cycle
Activity 12.1
Using flow-charts, diagrams and information collected in advance from the
library or internet, illustrate the action of hormones in the maintenance of themenstrual cycle.
This refers to the periodical changes in the reproductive behaviour of a female which
tend to occur in a sequence of events one after the other in the periodical circle. At
the onset of puberty, the cycle begins and repeats after 28 days unless interrupted
by pregnancy. The changes are stimulated by the gonadotrophic hormone such as;
follicle stimulating hormone (FSH) and luteinizing hormone (LH). These hormones
stimulate ovaries to secrete; oestrogen (steroid) and progesterone hormones.
These four hormones are involved in menstrual cycle. Two of them including; FSH
and LH are produced by pituitary gland and the other two are released by ovaries
respectively. The most obvious sign of the cycle is the monthly discharge of blood
a process called menstruation. The first day of menstruation is regarded as the first
day of the cycle. Figure 12.2 and 12.3 show the stages of menstrual cycle. Menstrualcycle is divided into three phases or events:
a. Follicular phase
Menstrual cycle usually begins when blood is first discharged from the uterus
during the first to fifth day (1-5 days). Following the reduction of progesterone, the
hypothalamus releases gonadotropin releasing hormone (GnRH) which stimulates
anterior pituitary gland to secrete follicle stimulating hormone (FSH). FSH bringsabout the following effects;
– Stimulates the development of a primary follicle
– Contributes to the shedding of uterine wall
– Causes production of oestrogen by uterine cells. The oestrogen produced
promotes healing, repair and growth of uterine lining, inhibits further secretion
of FSH. Oestrogen levels keep on raising until day 13 where they stimulate
secretion of luteinizing hormone (LH) by anterior pituitary gland.
b. Ovulatory phase
Around the 14th day, the high levels of oestrogen cause release of luteinizing hormone
(LH) the release of LH brings about ovulation (release of mature egg from the ovary).
Immediately after and slightly before ovulation, a woman is fertile and can conceivea baby if she has sexual intercourse or if sperm is present in her oviduct.
c. Luteal phase
After ovulation, the remains of ovarian follicle form corpus luteum also known as
Yellow body, which secrete large amounts of progesterone hormone and smaller
oestrogen. These two hormones; stimulate further development of mammary
glands, inhibit release of FSH and thickening wall of uterus in anticipation of
pregnancy. If oocyte (ovum) is not fertilized with in about 36 hours of being shed
into oviduct, it dies and corpus luteum gets smaller. Thus levels of progesterone
and oestrogen keep on reducing until day 28 days i.e. 14 days after ovulation. Low
levels of progesterone remove the inhibitory effect on FSH, causing its release thusmenstruation and the cycle starts again.
– At menopause there are no more fertile follicle so follicular development and
ovulation is ceased.
– The menstrual cycle is controlled by hormones from both brain and the ovary.
– The natural cycle repeats until there is either a pregnancy or the womanreaches menopause, the end of the reproductive phase of a woman’s life.
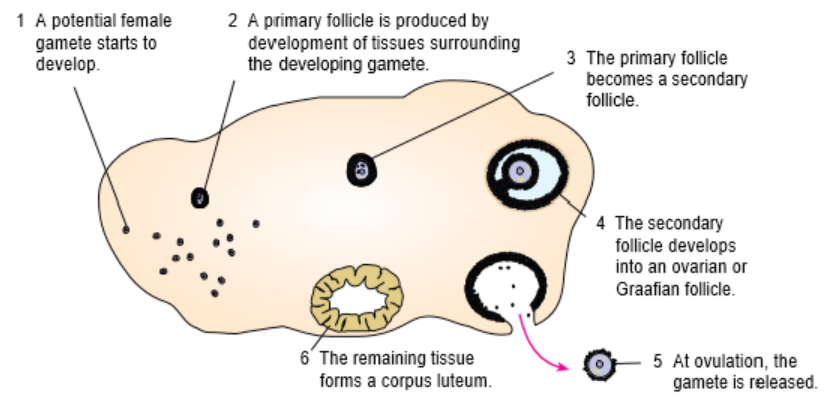
Figure 12.2: The growth of ovarian follicle.
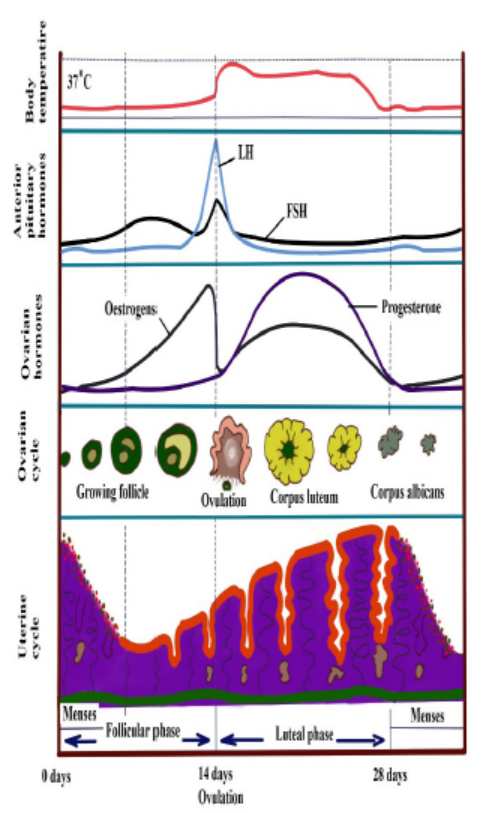
Figure 12.3: Hormonal and Menstrual cycle growth curve.
The uterine cycle also has three phases (events):
Proliferative phase: It stimulates the thickening of endometrium of the uterus. This
thickness of endometrium is stimulated by oestrogen from follicles before ovulation. This
results the development of ovary. It acts like follicular phase.
Secretory phase: it occurs after ovulation for describes further thickening of endometrium
(endometrium tissue become more complex) in preparation for implantation. This is
stimulated by progesterone which is secreted by corpus luteum and this occurs when
corpus luteum is functioning. It acts like lacteal phase.
Menstrual phase: when endometrium tissue is discharged and vaginal bleeding occurs at
the end of ovulatory cycle if pregnancy has not occurred. It is called menstruation.it describes
the shedding of endometrium when implantation does not occur. When pregnancy does not
occur the level of progesterone falls and this results shedding of endometrium. Menstrual
bleeding lasts between 3 and 5 days. The first day of the period is the first day of the cycle.
Oestrous cycle
The word oestrus is derived from the Latin language oestrus meaning sexual desire. It
describes the phase when the female animal is sexually receptive to a male. Females
of most species of mammals except human come into ‘heat’ known as oestrus in
regular cycles at particular times of year. Oestrus is the time when females are both
fertile and sexually receptive. Oestrus cycle is controlled by the same hormones as
the human menstrual cycle. FSH and oestrogen control the process until ripe ova are
released when LH and progesterone take over.
Application 12.1
1. What is the main difference between menstrual and oestrus cycle?
2. What are significant events which happen between day 13 and day 15
of menstrual cycle?
3. Asses the main events of menstrual cycle.
4. (a) Explain the meaning of oestrus cycle in mammals(b) State the difference between oestrous and menstrual cycle.
12.2 Copulation, fertilization and embryo development.
Activity 12.1
Watch a simulation from internet; illustrate the stages that bring aboutfertilization and development of an embryo.
12.2.1 Copulation
It is act of mating where sperms from male are transferred into the female tract.
Male mammals have an intromittent organ called penis which becomes erect at a
moment of mating for insertion into female’s vagina. The erection of penis is brought
by hydraulic action (penis becomes gorged with blood). This occurs as a result of
sexual arousal which brings about by ejaculation (release of sperm). The semen’s
are secreted from accessory glands into vas deferens and bladder sphincter closes
preventing urine from entering urethra. Sperms are expelled from epididymis into
vas deferens and out of the body by a series of muscle contraction of penis.
In a female, sexual arousal results in the swelling of clitoris and stimulates thesecretion of mucus which lubricates vagina during sexual intercourse.
12.2.2 Fertilisation
Fertilisation is the fusion of male and female nuclei to form zygote. Copulation
results in the ejection of spermatozoa into vagina. The spermatozoa swim in the
watery mucus of vagina and uterus up into the oviduct where the fertilisation takes
place in the upper part of the oviduct. From the vagina or uterus spermatozoa
propel using energy from mitochondria. If ovulation has already taken place, the
egg and sperm meet in the upper part of oviduct and once they come into contact,
acrosome raptures and release lytic enzyme which dissolve corona radiata of the
egg and soften zona pellucida and vetelline membrane. The following processestake place:
a. Capacitation
This is a stage where by sperm undergoes essential changes while passing through
female genital trackand this takes about 7 hours. These changes include the
removal of a layer of glycoprotein from outer surface of sperm, by enzyme in uterus.
Cholesterol also is removed to weaken the membrane.
b. Acrosome reaction
This involves the releasing of enzyme found in acrosome such as hyaluronidases
and protease. These enzymes digest corona radiata (narrow path in the follicle
cells) and the zona pellucida (a protective glycoprotein surrounding the plasma
membrane of the egg).
c. Fusion
In this stage the head of sperm will fuse with the microvilli surrounding the secondary
oocyte and penetrate its cytoplasm.
d. Cortical reaction
This stage involves the releasing of enzymes by lysosomes in cortical granules (outer
region of the secondary oocytes); the enzymes cause the zona pellucida to thicken
and harden forming a fertilization membrane. This cortical reaction prevents the
entry of other sperm inside ovum (polyspermy).
e. Zygote formation
The secondary oocyte is stimulated to complete meiosis II, during this time of
stimulation the nucleus of sperm and secondary oocyte are called pro-nuclei andthen the two nuclei fuse to form the zygote (2n).
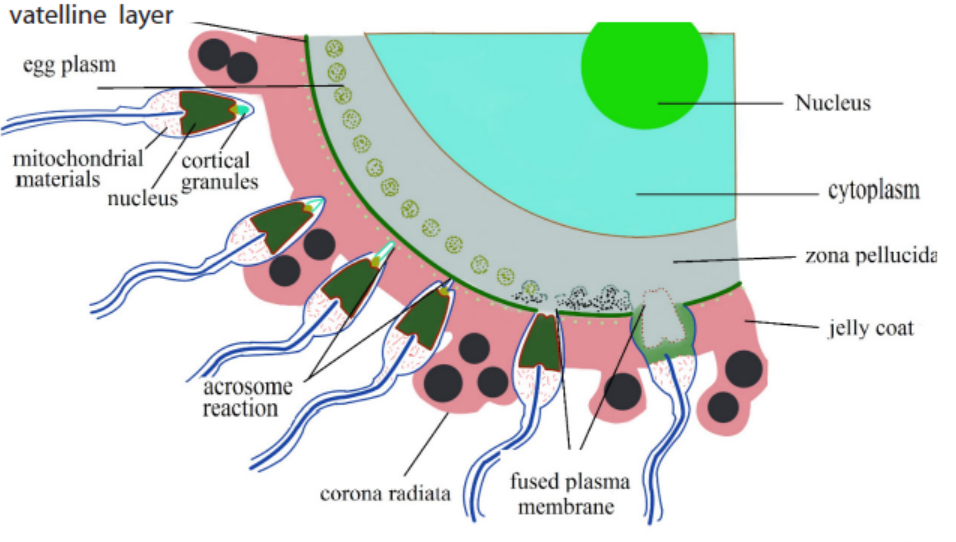
Fig 12.4: Process of fertilization
The movement of sperm in the female reproductive system;
Once sperm arrives the female reproductive tract, they moved largely by female
reproductive system:
– Around the time of ovulation, the vaginal mucus changes in PH in response
to changing levels of sex hormones. It is normally so acidic which can tend to
kill sperm. At the fertile time it becomes more alkaline to prevent sperm from
damage.
– The mucus which blocks the cervix, preventing the entry of pathogens and
become less viscous, allowing sperm to move through it more easily.
– Prostaglandin (local hormone) in semen and oxytocin hormone released by
posterior pituitary gland during sexual intercourse. Initiate the contraction inuterus, helps sperms to move towards fallopian tube.
12.2.3 Embryonic development
The zygote spends the next few days travelling down the oviduct (Fallopian tube) by
peristaltic contraction and by beatings of the cilia in wall of the oviduct toward the
uterus. As it travels, it divides by mitosis several times to form a ball of cells called a
morula. The cell divisions, which are called cleavage, increase the number of cells
but not their overall size. More cell divisions occur, and soon a fluid-filled cavityforms inside the ball of cells. At this stage, the ball of cells is called a blastocyst.
The blastocyst reaches the uterus and becomes embedded in the endometrium at
roughly the 5th – 10th day. Once in the uterus the blastocyst burrows into the uterine
wall a process called implantation. After implantation, the blastocyst becomes
embryo. It grows through multiplication and differentiation of its cells forming
tissues and organs. The heart and blood vessels are the first organs formed andembryo now called foetus.
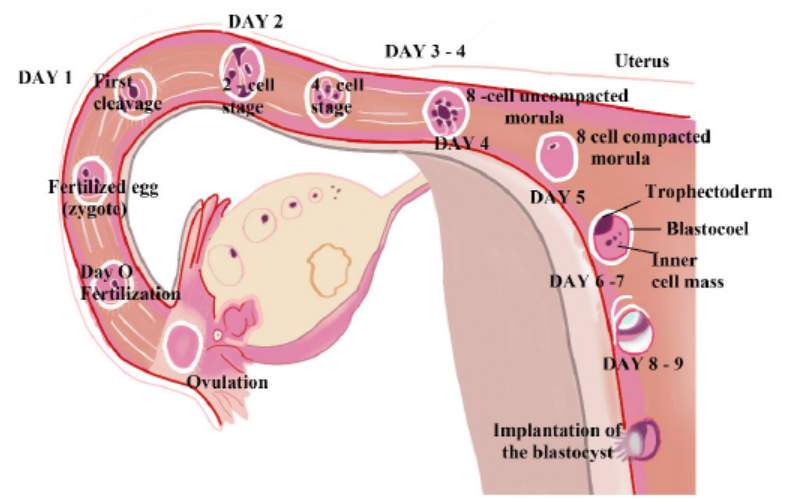
Figure 12.5: Embryo development during the first nine days
a. Stages of embryo development:
There are three major stages of embryo development;
i) Cleavage
The cleavage consists of the division of zygote without increase in mass into a ball of
consisting of many daughter cells.
ii) Gastrulation
It is the development of different layers of cells in the embryo. It generally occurs
during the second week after fertilization. During gastrulation, cells of the embryo
migrate to form three distinct cell layers: the ectoderm, mesoderm, and endoderm.
Each layer will eventually develop into certain types of tissues and cells in the body
of vertebrates.
– Ectoderm—it forms tissues that cover the outer body; develops into cells such
as nerves skin, hair, and nails.
– Mesoderm—it forms tissues that provide movement and support; develops
into cells such as muscles, bones, teeth, and blood.
– Endoderm—it forms tissues involved in digestion and breathing; develop intoorgans such as lungs, liver, pancreas, and gall bladder.
iii) Organogenesis and Differentiation
Differentiation of cells leads to the development of specific organs and tissues within
the three cell layers. This is called organogenesis. All the major organs begin to form
during the remaining weeks of embryonic development.
b. Extra-embryonic membranes
These membranes are part of placenta. The outer cells of the blastocyst, the
trophoblast grow and develop into an outer layer or membrane called the chorion.
This plays a major role in nourishing and removing waste products from the
developing embryo.
The amnion is a thin membrane covering the embryo like an umbrella and has a
protective function. Between the embryo and the amnion is the amniotic fluid. The
amniotic fluid supports the embryo and protects it from mechanical shocks.
The yolk sac has no significant function in humans but is important in reptiles and
birds, where it absorbs food from the separate yolk and transfers food to the gut of
the developing embryo.
Note:
The first trimester of the development or the embryo is critical. There is
high risk of spontaneous abortion or miscarriage due to alcohol, infection,
radiations (X-rays), nutritional deficiencies, genetic mistakes or abnormalities
in the developing embryo. From the 8th week until birth (around 38 weeks), the
developing organism is called a foetus. The foetus is not as sensitive to damage
from environmental exposures as the embryo, and toxic exposures often cause
physiological abnormalities or minor congenital malformation. All major structuresare already formed in the foetus, but they continue to grow and develop.
Application 12:2
1. Explain how sperms enter and later contribute to fertilisation of an
ovum?
2. Explain why only a single spermatozoon fertilises an ovum?3. What is implantation?
12.3 Role of Placenta in the development of embryo
Activity 12.3
Using a diagram of the placenta, discuss how its structure is related to itsfunctions
The placenta is a temporary organ in which nutrients and wastes are exchanged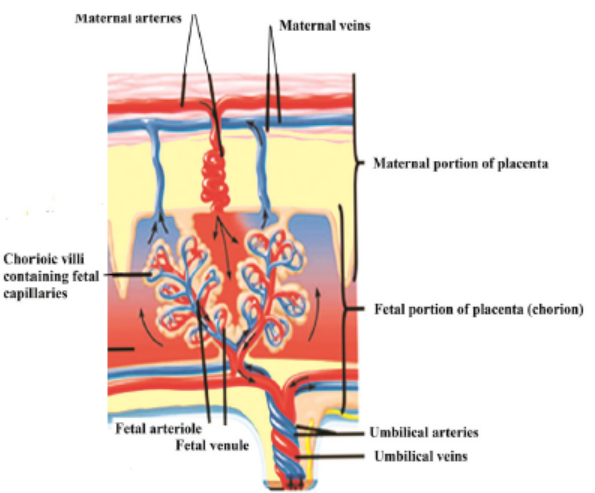
between the mother and the embryo or foetus.
The foetal part of the placenta consists of the allantoides and chorion. The chorion
forms many large projections called chorionic villi which contain a dense network of
foetal capillaries which in turn are connected to two umbilical arteries and umbilical
vein in the umbilical cord. The umbilical arteries carry blood from the foetus to the
placenta, while the umbilical vein carries blood in the opposite direction. Although
maternal blood in the endometrium is in close proximity with the foetal blood in the
umbilical capillaries, they do not mix because they separated by membranes of thevilli and capillary.
12.3.1 Functions of the placenta:
– Allows diffusion of nutrients such as water, glucose, amino acids, simple
proteins and mineral salts from maternal blood.
– It is a site of gaseous exchange: haemoglobin of the foetus has high affinity to
oxygen compared to adult haemoglobin.
– It offers passive natural immunity on the foetus. Certain maternal antibodies
can cross the placental barrier.
– It protects foetal circulation from the high pressure in the maternal circulation
– Prevents mixing of maternal and foetal blood which would cause agglutination
(clotting) if the two blood types are incompatible.
– It produces and secretes hormones such as the HCG (human chorionicgonadotrophin), progesterone, oestrogen, and relaxin.
Note that:
– The action of HCG is similar to that of LH. HCG stimulates the corpus luteum
to secrete progesterone and oestrogen throughout the first trimester. HCG
is produced in such large quantities that some of it is excreted in the urine
of a pregnant woman (positive test of pregnancy). Secretion of HCG declines
around tenth week and the corpus luteum reduces.
– The placenta does not give complete protection to the foetus. Certain
pathogens, toxins, and drugs can enter the foetal circulation and causedamage. Examples are; HIV, rubella toxins, alcohol, nicotine and heroin.
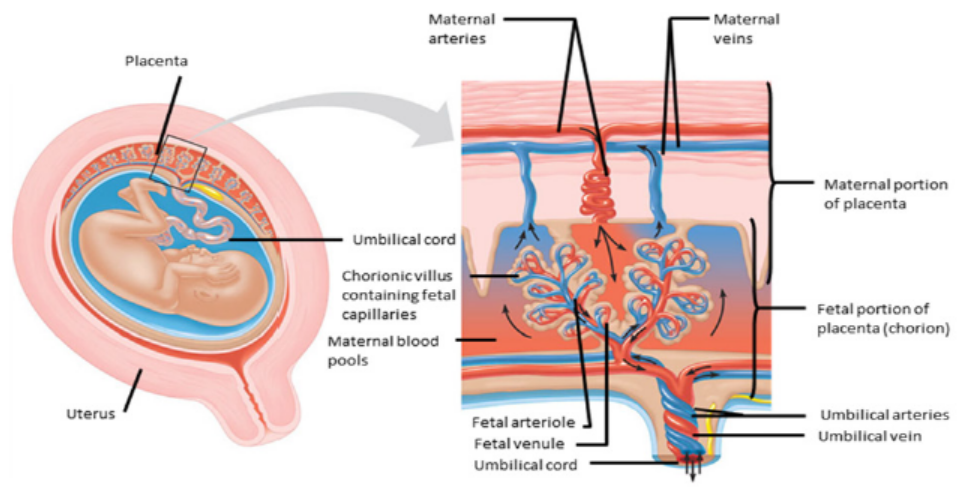
Figure 12.6: The structure of the placenta
12.3.2 How the placenta works?
Blood from the mother enters the maternal blood vessels of the placenta under
pressure, forcing the blood into the empty spaces. When the mother’s blood contacts
the foetal blood vessels, gases are exchanged. Oxygen from the mother’s blood is
exchanged with carbon dioxide from the foetus’s blood. A release of pressure brings
the mother’s blood back from the placenta and into her veins.
– The substances that are moved from the mother to the foetus include:
– Water
– Glucose by passive diffusion
– Hormones
– Amino acids by active transport
– Lipids by membrane lipid diffusion
– Oxygen is released by the maternal haemoglobin. The haemoglobin of the
foetus has a higher affinity for the oxygen.
– Alcohol, many drugs, nicotine (if taken by mother during pregnancy)– Vitamins, minerals.
The substances that are moved from the foetus to the mother include:
Carbon dioxide is taken up by the maternal plasma and transported to the lungs of
the mother for excretion
– Urea passes into the maternal blood and passes to her kidneys for excretion.
The exchange between the mother and the foetus is possible because of specific
structures in the placenta:
– The plasma surface membranes of the cells in the walls of the chorionic villi have
microvilli, which increase their surface area for the exchange of substances by
diffusion, facilitated transport and pinocytosis.
– Numerous mitochondria are found in these cells. They provide the energy for
the active transport and pinocytosis.
– The cell surface membranes contain carrier molecules (protein) used in the
uptake of materials into the villi by active transport.
– Numerous small vesicles are found inside the cells of the villi as a result ofmaterials being taken up from the blood by pinocytosis.
12.3.3 Pregnancy rapid test
Pregnancy tests look for a special hormone – human chorionic gonadotropin (HCG)
– that only develops in a woman’s body during pregnancy.
After the fertilized egg implants, the growing placenta starts releasing HCG into
your blood. Some HCG also gets passed in your urine. HCG can be found in the blood
before the first missed menstrual period. This can be as early as 6 days after the egg
implants.
These tests can use either your urine or blood to look for HCG.
At-home pregnancy tests are inexpensive and commonly used urine tests. There are
a few things to keep in mind when you take a home pregnancy test:
– Use your first morning urine when possible. This is the time of day when your
HCG levels will be the most concentrated and easily detected. If you do it at
another time of day, try and make sure your urine has been in your bladder forat least four hours.
– Don’t drink excessive amounts of fluids before you take a pregnancy test. Many
people think this will increase the volume of urine, but it can also dilute (thin
out) your HCG levels.
– Read the directions that come with the test thoroughly before starting the test
and following every step precisely.
– Collect your urine in a cup and use an eyedropper to move a small amount of
fluid into a special container
– Place the testing stick/strip into the area of your expected urine stream so that
it will catch your urine midstream.
– Wait for the recommended amount of time to view the results which can
include: a change in color – a line – a symbol, such as plus or minus, or – thewords “pregnant” or “not pregnant”

Figure 12.7 Home pregnancy test
Application 12.3
1. What do you understand by the term implantation?
2. Describe the composition of foetal blood entering the placenta and foetal
blood leaving the placenta.
3. Explain the urine of pregnant woman give a positive test while that of non –pregnant one give the negative test.
12.4 Physiological changes during pregnancy and parentalcare
Activity 12.4
Using models that show stages, discuss physiological, physical, and behaviouralchanges that occur during pregnancy.
Pregnancy refers to the development that take place between fertilisation of the
ovum to birth of the foetus. When fertilised egg becomes implanted in uterine wall,
pregnancy results. And a number of important events take place during this period.
The period from fertilisation to birth is called gestation period. In human it is aboutnine months.
12.4.1 Changes during pregnancy
A pregnant woman’s body undergoes various; physiological, physical and behaviouralchanges.
a. Some physiological changes during pregnancy:
– Respiration rate rises for increased maternal oxygen consumption which is
needed for demand of placenta, uterus and foetus.
– More blood vessels grow and pressure of expanding uterus on large veins
causes blood to slow in its return to the heart.
– Rise up and out of pelvic cavity this action displaces the stomach and intestine.
– Blood volume increase greatly.
– Placenta produces large amount of progesterone and oestrogen by 10 to 12
week of pregnancy to control uterine activity.
– Increased requirement of calcium due to increase of parathyroid gland.
– Experiences warm (hot flashes) caused by basal metabolic rate and increased
hormonal level.
– Stretching of abdomen wall and ligaments that support uterus.– Kidney work extra hard to excrete waste products of both mother and foetus.
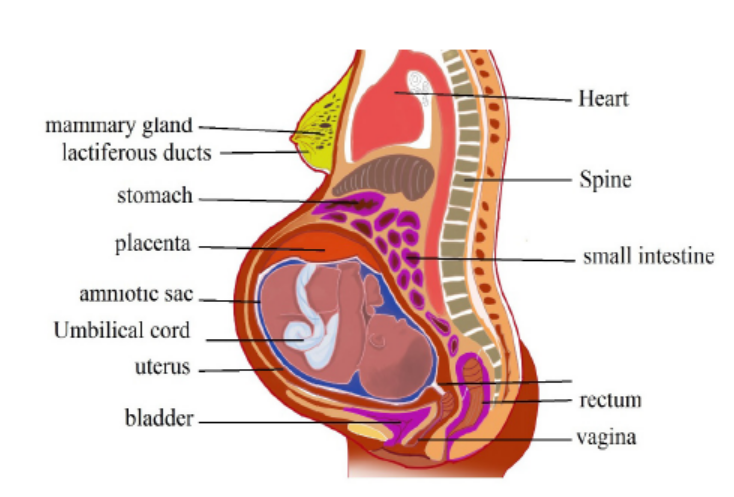
Figure 12.8: Changes during pregnancy.
b. Some physical changes during pregnancy
– Breast may become large and more tender because of increased level of
oestrogen hormone progesterone thus breast gets even bigger to prepare for
breast feeding.
– Nipples may stick out more.
– By the end of third trimester, a yellow, watery, pre-milk may leak from nipples.
– Changes in hair and nail growth and texture due to hormone changes.
– Leg cramp caused by fatigue from carrying pregnant weight.
– Feet and ankles may swell because of extra fluid in the body during pregnancy.
c. Some behavioural changes during pregnancy:
– Physical discomfort such as urinary frequency can be frustrating.
– Fear and anxiety lessen especially foetal movement are felt.
– Self-introspection
– Nesting behaviour begins. Some woman exhibit mood swings and emotional
liability.
12.4.2. Delivery process
By the end of pregnancy, near the time of birth, the amniotic sac raptures (breaks)
and amniotic fluid drains through birth canal and labour usually begins which
involves the contractions of muscular walls of the uterus.
Initiation of birth: Uterine contractions starts when the foetal pituitary gland secretes
adrenocorticotrophic hormone (ACTH) which stimulates foetal adrenal gland to
secrete corticosteroids. These hormones pass into blood sinuses in placenta to cause
maternal cells to secrete prostaglandins (local hormone) and cause uterine wall to
contract. This contraction pushes the foetal head against the cervix to stimulating
stretcher receptor to send information to mother’s brain and causes release of
oxytocin hormone. The prostaglandin and oxytocin hormone together result intense
contraction of uterine walls called labour which stimulates more release of oxytocinhormone and as positive feedback mechanism.
The delivery process can be summarized into three main stages:
– Dilation stage: During this stage, water sac filled with amniotic fluid forms
and precedes the head, widening soft tissue of birth canal, cervix, and vagina
for canal of constant diameter. The amnion raptures and amniotic fluid drains
through vagina.
– The expulsion stage: During this stage, cervix is fully dilated while abdominal
muscle bear down in supporting rhythmic contraction of uterus shorten the
uterine wall and baby is pushed into and through the birth canal. The head
and shoulder align themselves first.
– Placenta stage: This stage begins with complete expulsion of baby and ends
with expulsion of foetal membrane. The cord is clamped and cut when delivery
of baby is complete. This leads carbon dioxide enrichment into baby’s blood
which activates respiratory centre and baby begins to breath with the first cryat the same time foetal circulation changes to baby’s own systemic and
12.4.3 Parental care
The degree of maturity in mammalian new-borns varies from one species to another.
New-born in pigs can move around and eat solid food while new-born in humans,
dogs and rat are quite helpless and require a lot of parental care to survive. All
mammals feed their young ones by milk which contain all the nutrients required
by new born for the first few days. Parents also protect new born from predators
and from unfavourable weather. Some species make nest just before delivering the
new born. Some parents also become aggressive when they have young one. As the
young one grow older the parent start gathering food for them. Once the new born
get old enough to gather food for themselves can leave on their own. In humans’parental care extends for very long time up over 18 years.
In humans breastfeeding is associated with many benefits:
– It makes earlier a closer contact between the mother and her infant
– Breastfed babies do not get too fat
– The infant has a better control over its own milk intake, this prevents over
eating in late life
– Fats and irons from breast milk are better absorbed than those in cow’s milk
and milk is easily digested.
– Breast feeding provides important antibodies that help to prevent respiratory
infections and meningitis,
– Breastfeeding helps the mother’s reproduction organ return to a normal state
more rapidly
– Breast feeding promotes the secretion of LH (and prolactin) and this makes a
delay in follicle development and ovulation,
– The act of sucking on the breasts, promotes the development of the jaw, facial
muscles and teeth (sucking from a bottle requires less effort).
– Pulmonary circulation. After delivery, uterus contract so that placenta separates
from– Uterine wall expelled out as the sign of birth end.
Application 12.4
1. How can you assess physical changes that occur during pregnancy?
2. Discuss the significance of parental care in mammals3. Describe the different stages of birth?
12.5 Twins and multiple births
Activity 12.5
Watch a movie simulation from internets to illustrate the types of twins andexplain how multiple birth arise.
Twins are individuals born to the same mother at the same time. Twins include;
– Fraternal twins or non-identical twins or dizygotic twins: These are twins
which develop from two separate egg cells fertilised by two different sperms.
Fraternal twins are genetically different since they develop from different
gametes.
– Identical twins or monozygotic twins: these are twins which develop from the
same fertilised egg. Identical twins are genetically similar since they develop
from the same sperm and the same egg.
– Siamese twins: are conjoint identical twins i.e. they have not completely
separated during the embryo development. As consequence, they share same
organs. Conjoint identical twins develop without separating completely andare born attached to one another. Such twins may be separated surgically.
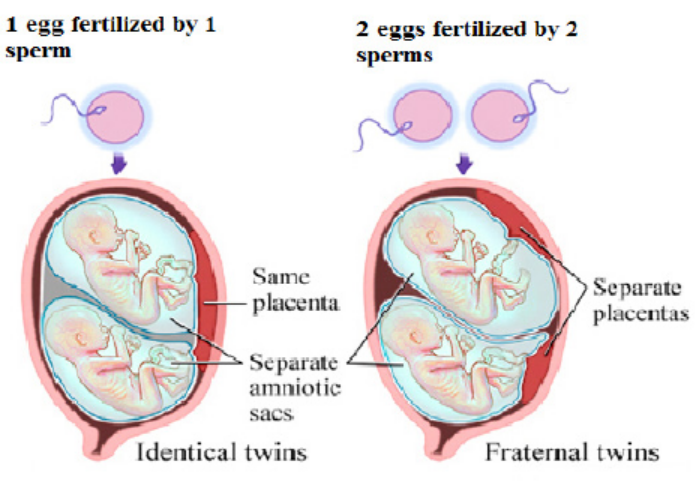
Figure 12.9: Identical and fraternal twins
Multiple births arise when several eggs are released at the ovulation and are
fertilised or when a zygote splits into several zygotes. It is commonly occurring in
mammals such as; pigs, dogs and cats.
Application 12.5
Explain how twins and multiple birth arise?
12.6 Infertility or barrenness
Activity 12.6
1. Discuss the social and economic consequences of barrenness
(infertility), producing many children by a couple and suggest methods
to cope with these issues.
2. Using the internet or library, research about in-vitro fertilization and
discuss the ethical implications.
12.6.1 Infertility
Infertility is the failure to achieve pregnancy when no contraceptive method is used.
In females, infertility may be due to:
– Failure to ovulate due to the lack of some hormones
– Damage of the Fallopian tubes / oviducts, for example the tubes may be
completely blocked by nature or after an infection,
– Damage on the uterus; for example, the endometrium can be destroyed
– Damage on the cervix, for example the cervix may be narrow or too wide or
may stop producing cervical mucus needed for the sperm to reach uterus
– Antibodies against sperms, for example, the cervix, the uterus or the oviduct
of a woman can produce antibodies against her husband’s sperms.
Some causes of infertility/barrenness in males include:
– Absence of sperms in the semen (Azoospermia).
– Low sperm count e.g. when ones ejaculate less than 1cm3 of semen.
– Abnormal sperm e.g. sperms with 2 tails, or without tail, or without acrosomes,
– Auto-immunity e.g. antibodies attack one’s sperms
– Premature ejaculation: the man has orgasm before copulation
– Impotence i.e. inability to achieve or maintain an erection of the penis.
a. Some social consequences include:
– Isolation including exclusion from ceremonies and social gathering.
– Rejection being an outcast and physical abuse perpetrated by community
members.
– Stigmatization or recognizable marginalization.
– Status loss that is no respect and social fail.
– Ridicule including insults and verbal abuse.
Some economic consequences include:
– Cost of infertility by either modern biomedical or traditional treatments.
– A feeling of rejection.
– Having few relations, receiving few gifts and less land.
– Marital instability including fear of husband taking second wife.
– Divorcing childless woman
– Violence perpetrated by partner.
Note:
While infertility may result into conflicts between couples and families, producing
many children also brings about some economic challenges. Many children affect
families’ financial wellbeing and some parents admit that children are expensive.
Consequences of many children per one family include:
– High rate of maternal depression.
– Low rate of immunization and parental care.
– Baby taxing both physical and emotional especially off work after birth.
– I come tend to go up when new members of the family arrive. Men see the
boost in their earnings after birth of child.
– There is economic wellbeing decline in time around birth.
b. Increasing fertility
Increasing fertility can be done in various techniques such as:
– Fertility drugs: a synthetic chemical which stimulates ovulation by either
proving gonadotrophins such as FSH which stimulates growth of follicles. Or
proving chemical which inhibits natural production of oestrogen.
– Artificial insemination: sperm from donor is inserted artificially through cervix
of mother to be.
– Using in-vitro fertilisation
12.6.2 In-vitro-fertilisation
In-vitro fertilisation is the process of fertilisation where an egg is fertilised by sperm
outside the body. It involves the fertilisation of egg cell outside the body which
are then artificially implanted in the uterus to produce test tube baby. The process
involves monitoring and stimulating of woman’s ovulatory process removing ovum
(egg) from woman’s ovaries and letting sperm to fertilise them in liquid laboratory.
The fertilised egg (zygote) undergoes embryo cultured for 2 to 6 days and then
transferred to the same or another uterus for successful pregnancy. The embryo is
implanted in woman’s uterus.
Advantages of in vitro-fertilization techniques include:
– Simplicity: living organisms are extremely complex functional system with
protein molecules, RNA molecules and genes. Therefore, the work of Vitro
simplifies system under study to focus on small number of components.
– Species specificity.in human cells in-vitro method can be studied without
extrapolation from experimental animal’s cellular response.
– Automation and convenience: In-vitro method can be automated, high
yielding throughout screening methods for testing molecule in pharmacology.
– In vitro- fertilisation can be used to achieve successful pregnancy but the
process usually produces more embryos which some scientists wish for
research design to improve our knowledge about disease.
Application 12.6
1. Define in-vitro-fertilisation
2. Outline the techniques of in-vitro-fertilisation.
12.7 Family planning: birth control and contraception
Activity 12.7
Using the internet or library, research about birth control methods and write a
summary of what you have learned.
– Birth control includes contraception, but is broader in meaning because it also
includes any measures taken after fertilization which are designed to prevent
birth. Contraceptionis preventing the fusion of the male gamete and female
gamete. Both natural and artificial methods exist.
Artificial methods:
– Oral Contraceptive pills: a chemical method of contraception. One version
uses a combination of progesterone and oestrogen that inhibits ovulation.
Others are single hormones that require very careful management when taken.
– Intrauterine device (IUD) the coil is placed inside the uterus an exact
understanding how this works is unclear. A possible explanation is that it
‘irritates’ the endometrium such that rejects implantation of embryos. The
device is made from plastic or copper and inserted by a doctor. Nevertheless,
this device is very effective.
– Condom is another mechanical method of contraception that prevents the
sperm from reaching the egg. Composed of a thin barrier of latex this is placed
over the erect penis and captures semen on ejaculation. This is also a good
barrier to prevent the transmission of sexual diseases.
– Cap (diaphragm) is another barrier method again made from latex. The cap is
placed over the cervix to prevent the entry of sperm in semen. This technique
requires that the cap is put in position in advance of sexual intercourse and
that it is used in combination with a spermicidal cream. When used correctly
this is an effective contraceptive however this is not a barrier against the
transmission of sexual diseases.
– Sterilisation is a surgical and near permanent solution for contraception such
as: Vasectomy. In men this involves cutting the vas deferens and prevents
sperm entering the semen. In this state, man still ejaculates normally and
releases semen however this does not contain sperm.
– Tubal ligation. Involves the cutting of fallopian tube so that eggs cannot reach
the uterus. In women the surgery cuts or ties the oviducts thus preventing
sperm from reaching the egg in fertilisation.
– Natural method:
– Natural birth control methods include specific actions that people can donaturally to help prevent an unintended pregnancy.
– Abstinence: the individual makes the choice to delay sexual intercourse until
the decision to conceive a child is made.
– Withdrawal is a behavioural action where a man pulls his penis out of the
vagina before he ejaculates. The withdrawal method also relies on complete
self-control. You must have an exact sense of timing to withdraw your penis in
time.
– Fertility awareness methods: This require a woman to monitor her body to
determine when she is most fertile. You then avoid having unprotected sex
around the time of ovulation.
– This natural birth control method involves paying attention to different body
changes (such as basal body temperature or cervical mucus) and recording
them to predict when you will ovulate. To be successful, you need to be willing
to record and chart your fertility signs.
– Then, you (and your partner) must agree to not have sex (or to use backup
birth control) for 7 days before and 2 days after you ovulate.
– Fertility awareness methods include the Billings Method, the Symptothermal
Method, and the Standard Days method.
– Continuous (Lactational Amenorrhea Method) can postpone ovulation for
up to 6 months after giving birth. This natural birth control method works
because the hormone required to stimulate milk production prevents therelease of the hormone that triggers ovulation.
Advantages and disadvantages of birth control
Some advantages of birth control/contraceptives
– Gives great protection against unplanned pregnancy if one follows instructions.
– Condoms to some extent protect against pregnancy and STDS.
– Combinations of pills reduce/prevent cysts in breasts and ovaries.
– Improved family wellbeing.
– Improved maternal and infant health.
Some disadvantages of birth control/contraceptives
– Necessity of taking medication continually.
– High cost of medication.
– Hormonal contraceptive does not protect against STDS.
– Eggs may fail to mature in the ovary for a woman who uses hormonal
contraceptives.
– Woman must remember to take them regularly.
– Woman must begin using hormonal contraceptive in advance before they
become effective.
– Some women experience several; headaches, breast tenderness, chest pain,discharge from vagina, leg cramps and swelling or pain.
Application 12.7
1. Describe the main types of birth control techniques.2. Discuss the advantages and disadvantages of birth control methods.
12.8 Causes and prevention of STIs and HIV
Activity 12.8
Make research from the internet or library on the causes and prevention ofSTIs and HIV.
Sexual transmitted infections include:
1. Acquired Immune Deficiency Syndrome (AIDS)
It is a serious disease which suppresses body defence. It is characterised by
suppression of immune system leading to development of a number of rare
infectious diseases. It is caused by virus known as Human Immunodeficiency Virus
(HIV). This virus can be transmitted from sick/infected person to healthy one in a
number of ways:
– None protected sexual intercourse either homosexually or heterosexually. It
passes from infected semen or vagina fluid to blood of health person through
damaged tissue in the vagina, penis or rectum.
– From sick mother to her baby during birth or through breast milk during
suckling.
– Through transfusion blood by contaminated needles.
– Through sharing contaminated sharp instruments.
HIV attach white blood cells (helper T cells) which is essential component of the
body’s immune system. HIV is retrovirus invades its genetic materials into the host’s
body and therefore its DNA remains dormant in host cells and being replicated
leading host cells to divide. When HIV uses host cells to manufacture new viruses.
New viruses burst out of host cells and eventually kill it and new host cells to infect
to supress immune system thus HIV develop into AIDS and show number of diseases
such as: tuberculosis, skin cancer, pneumonia and thrush and a person may show
some symptoms such as: swelling of lymph glands, fever, sweating and fatigue,
coughing, diarrhoea and unexplained loss of weight. The death may result as there
is no known cure for AIDS but drugs reduce its progress but cannot stop it. Other
symptoms include:
– Headache
– Vomiting, and upset stomach
– Mouth, genital, or anal sores
– Rash or flaky skin– Short-term memory loss
Treatment:
No specific treatment for AIDS but some drugs may be used to treat various infections
that come about as result of AIDS.
HIV infection is not easy to treat. Some reasons why HIV is difficult to treat are as
follow:
– HIV remains inactive in host cells for years and it cannot be targeted and
destroyed.
– Since its symptoms are not easily evident, the infected person may continue
spreading the virus knowingly or unknowingly.
– HIV is extraordinary variable therefore cells of immune system identify infective
agents by shapes of antigen on their protein coats means that HIV cannot be
detected easily by changing shape of its antigens.
– HIV destroys helper T cells which help in body defence thus difficult to control
it.
2. Syphilis:
– It is serious sexually transmitted disease caused by bacteria Treponema
pallidum. The symptoms of syphilis occurred in three stages if not cured.
– Stage I: it appears between 10 days to 3 months after the time between
contact and appearance of first symptom (incubation period). The disease
begins with painless sore which appear on sex organs and it heals itself.
– Stage II: it appears between 2 to 6 months after contact with disease such as:
headache, fever, pain in bones and joints and sore throat.
– Stage III: it appears about 10 years after contact with disease such as: nervous
system, heart and aorta therefore the result is serious damage to affected
organs.
Ways of transmission: Syphilis can be transmitted through sexual intercourse.Treatment: Syphilis can be cured completely by antibiotics such as penicillin.
3. Gonorrhoea
It is a common sexually transmitted disease caused by bacteria Neisseria
gonorrhoea. It can also have transmitted from mother to baby during birth. The
first symptoms appear from 3 to 5 days after sexual contact with infected individual
and discharges from genital thus burning sensation during urination but in female
there is no symptoms:
– Pain or burning when urinating
– Yellowish and sometimes bloody vaginal discharge
– Bleeding between periods
– Pain during sex
Ways of transmission: Gonorrhoea is transmitted through sexual intercourse. It can
also have transmitted through from mother to baby during birth thus affect newborn’s
eyes.
Ways of treatment: It can be cured by antibiotics but if untreated it may lead sterility,
heart disease and blindness.
4. Genital herpes (simplex).
It is a sexually transmitted disease caused by herpes simplex virus. Symptoms
include: small red bumps, blisters, or open sores where the virus entered the body,
such as on the penis, vagina, or mouth. Its symptoms include:
– Vaginal discharge
– Fever
– Headache
– Muscle aches
– Pain when urinating
– Itching, burning, or swollen glands in genital area
– Pain in legs, buttocks, or genital area
– Symptoms may go away and then come back. Sores heal after 2 to 4 weeks
Ways of treatment: No specific cure for the disease but number of drugs may be
used to reduce pain and even further attach.
5. Trichomoniasis
It is caused by protozoan Trichomonas vaginalis, transmitted through sexual
contact, underwear and toilet seats. Its symptoms are; itching of urethra or vaginal
in females, yellow discharge and smelly.
Ways of Prevention/control include: Avoiding indiscriminate sex, avoiding sharinglinen and personal hygiene.
6. Hepatitis
It is caused by virus hepatitis B through sexual contact, contaminated needles, blood
transfusion and syringes. Its symptoms include; Fever, jaundice, nausea (sickness,
vomiting), loss of appetite and yellow urine.
Ways of prevention include; avoiding indiscriminate sex, use disposable needles and
syringes and strict personal hygiene.
7. Candidiasis
It is caused by fungus Candida albicans through sexual contact, sharing linen and
towels. Its symptoms include; Itching and burning sensation and white discharge
from genitals.
Ways of prevention/ control include; Avoid indiscriminate sex and treat both partners
Ways of controlling STIs / STDs:
– Abstaining from sexual intercourse in order to avoid STDS.
– Using of condoms during sexual intercourse.
– Going for blood check-up before engaging in sexual activities.
– Not engaging in homosexuality/lesbianism reduces the risk of STDS.
– avoiding multiple sexual patners– Getting medical attention as soon as possible in case of getting infections.
Application 12.8
1. What is difference between AIDS and HIV?2. Explain why AIDS is more difficult to eradicate than any other diseases?
End of unit assessment 12
1. What do you understand by the following terms?
a. Zygote
b. Endometrium
c. Implantation2. Study the diagram below and answer the questions that follow:
Choose the number from the above diagram which matches with each of the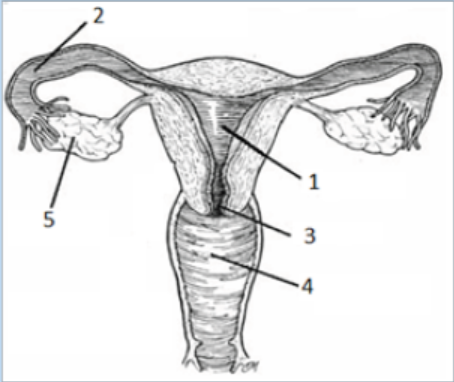
following events:
a. The fertilization takes place.
b. The sex intercourse takes place
c. The zygote develops
d. Follicles develop
e. The opening closes during the pregnancy.
3. What effect do the following hormones have on the size of the follicles?
a. FSHb. LH
4. Answer the following questions:
a. Define the term fertilizationb. The diagram below shows the structure of a human sperm.
i. Explain the part played by the organelle labelled A in the process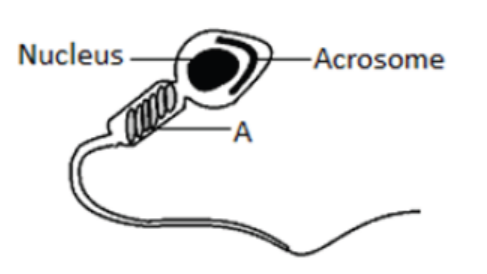
leading to fertilisation.
ii. The acrosome contains an enzyme that breaks down proteins. Describe
the function of this enzyme in the process leading to fertilisation.
5. Study the figure below on menstrual cycle and answer the questions thatfollow:
a. Name the hormones labelled a, b, c and d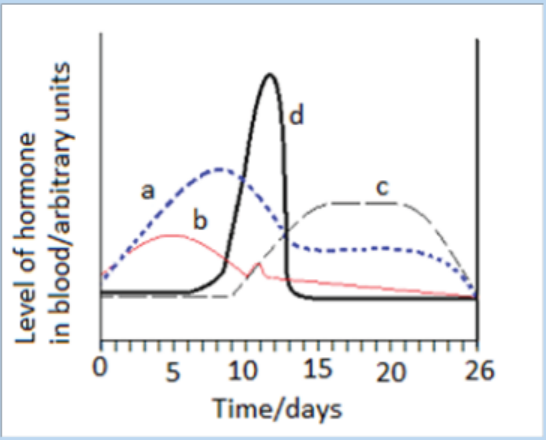
b. Give the likely day of the cycle on which ovulation takes places and give
reason for your answer.
c. What is meant by the term ovulation?d. State any 2 physical features which can prove that a female has ovulated.
6. The chard diagram below shows one way in which twins can be formed:
a. Give the name of the cell X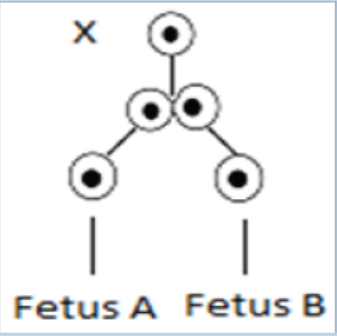
b. Why in this case will the embryo develop into identical twins?
7. Access the events that take place between the following stages in human
female.
a. The time the sperm meet the egg and fertilisation.
b. Fertilisation and implantation.
8. The eggs of birds are relatively much larger than those of mammal. Suggest
reason to account for the difference.
9. Identify the changes (events) occur in the uterus of a woman for menstrual
cycle to take place.10. Discus the main ways by which HIV is transmitted?