UNIT 4 MANAGEMENT OF THE FIRST STAGE OF LABOUR
Key Unit competence: Manage a woman in the first stage of labour
4.1. Stages of labor
Learning Activity 4.1
Madam Kawera came in labour suite, complaining of labour pain that started
2 hours ago. She reports that a nurse earlier told her that she has a cervical
dilatation of 6 cm and the fetal descent was at 0 station, FHR was 140b/minute.
Uterine contractions were 3 in 10 minutes lasting 40 seconds. Her membranes
were intact and no any other complain.
Answer the following questions based on information given to you by madam
Kawera, previous lessons in unit 1,2 and 3 and books:
1. In which phase of labour is Madam Kawera?
2. In which stage of labour is Madam Kawera?
The labor and childbirth processes are natural phenomena during which most
women benefit from a philosophy of minimal intervention.
The first stage of labor starts from the commencement of contractions and lasts
until full dilatation of the cervix. It is a progressive process, and is divided in 3
phases: the latent phase begins with the establishment of regular contractions
(labor pains). Labor pains are often initially felt as sensations similar to painful
menstrual cramping and are usually accompanied by low back pain. Contractions
during this phase are typically about 5 minutes apart, last 30 to 45 seconds, and
are considered to be mild. The latent phase of labor can last as long as 10 to 14
hours as the contractions are mild and cervical changes occur slowly (0 to 3 cm of
dilation).
The active phase of labor is characterized by more contractions, they become
more frequent (every 3 to 5 minutes), last longer, and are of a moderate to strong
intensity. During the active phase, the cervical dilation advances more quickly (4
to 7 cm) as the contractions are often more efficient. While the length of the active
phase is variable, nulliparous women generally progress at an average speed of 1
cm of dilation per hour and multiparas at 1.5 cm of cervical dilation per hour.
The transition phase is the most intense phase of labor (8 to 10 cm of dilation).
Transition phase is characterized by frequent, strong contractions that occur every
2 to 3 minutes. Fortunately, this phase often does not take long because dilation
usually progresses at a pace equal to or faster than active labor (1 cm/hr for a
nullipara and 1.5 cm/hr for a multipara). During the transition phase, the laboring
woman may feel that she can no longer continue; rectal pressure, an increased
urge to bear down, an increase in bloody show, and spontaneous rupture of the
membranes (if they have not already ruptured).
The second stage of labor is traditionally defined as the stage from full cervical
dilation until the baby is born. Usually, the actual time of onset is uncertain because
the complete cervical dilatation does not always go with the descent and station of
the presenting part. The woman may experience vomiting, often with contractions;
show or bright red vaginal loss; spontaneous rupture of the membranes can occur
any time but often at full dilatation; urge to push; powerful, expulsive contractions
every 2–3 minutes, often lasting ≥60 seconds.
The third stage of labor refers to the period following the completed delivery of the
newborn until the completed delivery of the placenta. The length of the third stage
and its complications are affected by the uterine contractility and the duration of
placental separation.
This stage usually lasts 5 to 10 minutes, and may last up to 30 minutes. Once thebaby is born, the uterine cavity immediately becomes smaller.
Table 4.1: Classification of stage and phase oflabour based on cervical dilatation
The appropriate time taken for each stage of labour depends on gravidity. In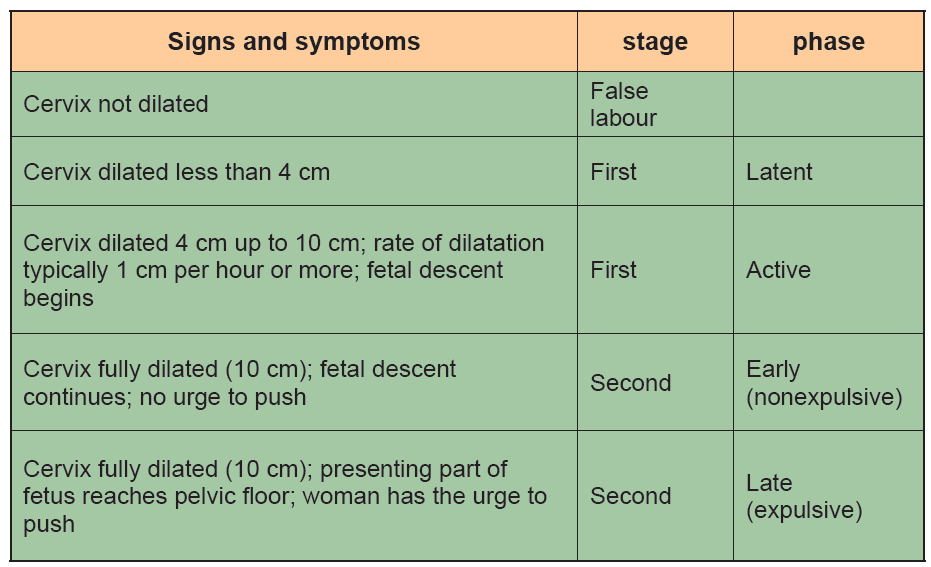
primigravidae the first stage lasts between 12 to 14 hours and 6 to 10 hours in
multigravidae; the second stage lasts 60 minutes for primigravidae and up to 30
minutes for multigravidae; the third stage lasts 20 to 30 minutes or 5 to 15 minutes
for primigraviadae and multigravidae in active management.
Self-assessment 4.1
1 Define the characteristics of the first and second stages of labor including
contractions and dilation.
2. Describe the three phases of the first stage of labor and the changes that
occur during each phase?
4.2. Care during the first stage of labour
Learning Activity 4.2
Using different source of information (internet, library) discuss in group, the care
provided to a pregnant woman during the first stage of labour.
During labour a pregnant woman receives the care that is centered to her.
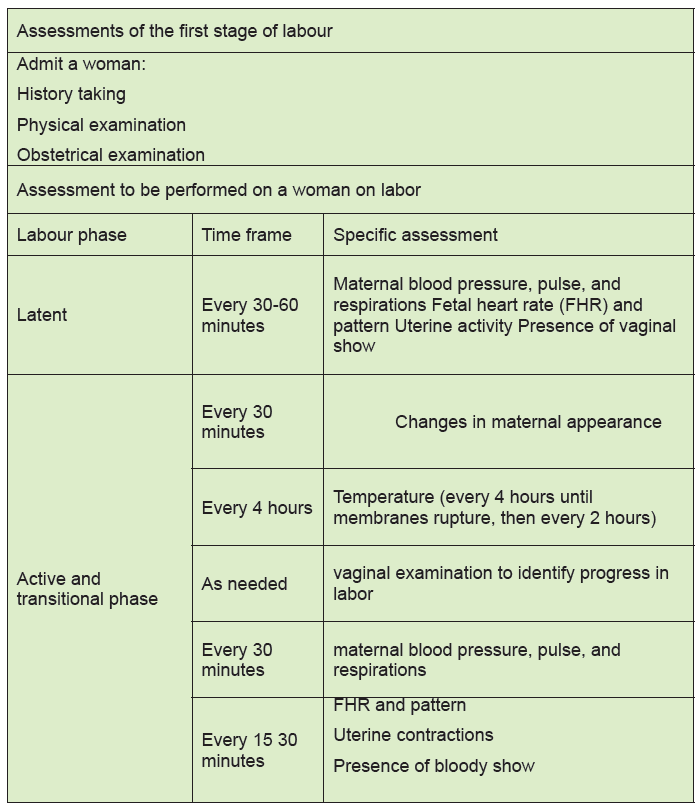
The following table is showing the care provided during management of the first
stage of labour.Table 4.2 Care during the first stage of labour
Self-assessment 4.2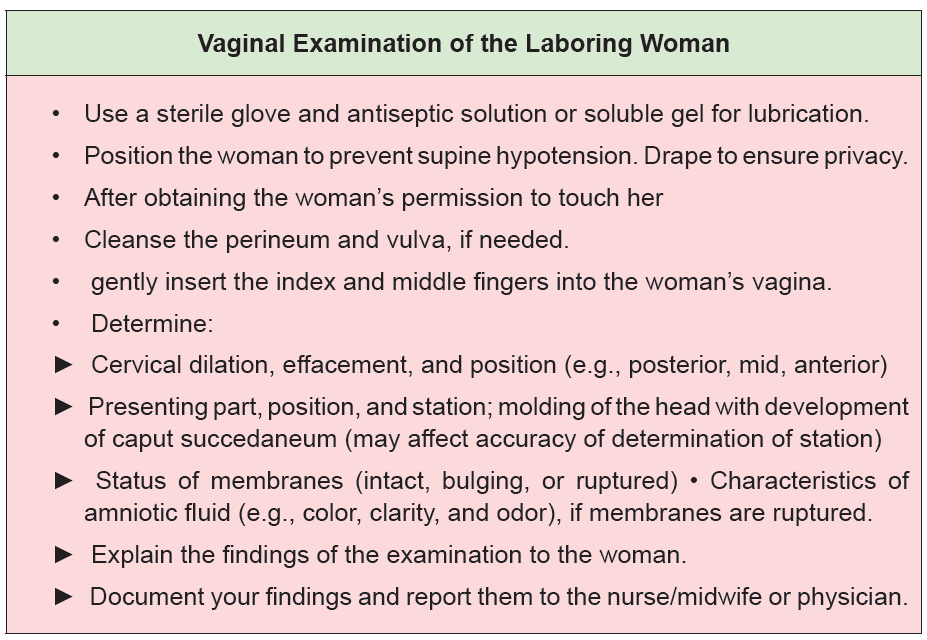
1. If a pregnant woman’s cervix is 2 cm dilated, when should you perform the
next vaginal examination?
a. After 2 hours of admission.
b. After 8 hours of physical exercises.
c. When the woman wants to bear down.
d. When there are signs that the woman is in established labour with more
regular and painful uterine contractions.2. In general, what must be monitored during the first stage of labor?
4.3 Labor Support
Whenever possible, continuous labor support should be given to women in labor and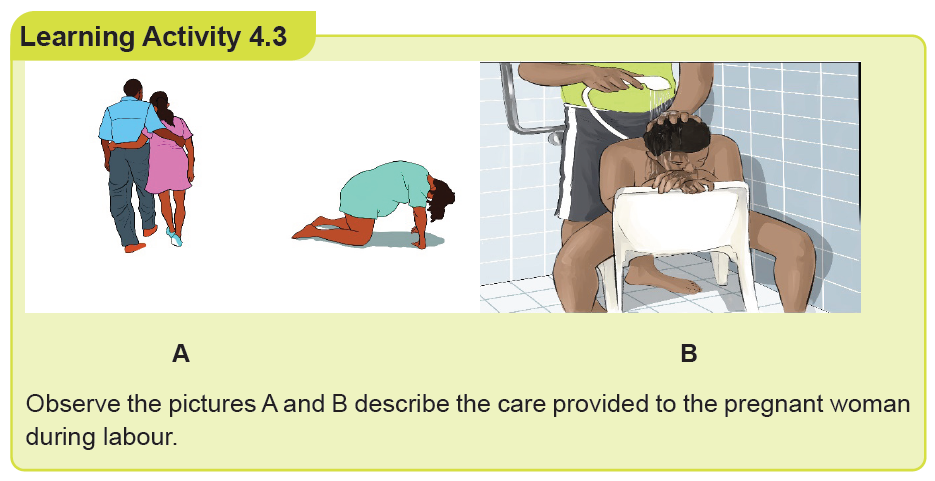
providing this level of care has been associated with positive outcomes for mothers
and infants. Continuous labor support can be provided by health professional or by
lay people and include presence, promotion of comfort, anticipatory guidance,
caring of birth partner, and ensuring culture centered care.
• Presence: Offering one’s presence in labor can be defined simply as “physically
being with the woman.” Women find that having a skilled birth attendant present
can be reassuring because they recognize that assistance is available when
needed. Women want a healthcare professional or a person of choice to be
available, to be emotionally involved, to help create a special moment, to hear
and respond to their concerns, to share the responsibilities for keeping themsafe, and to act as a go-between for their family and the medical institution.
• Promotion of comfort: Women comfort is always needed and include different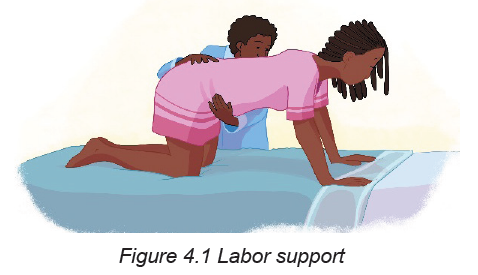
measures which are positions changes and personal comfort measures.
► Position Changes: In labor, frequent position changes are beneficial in helping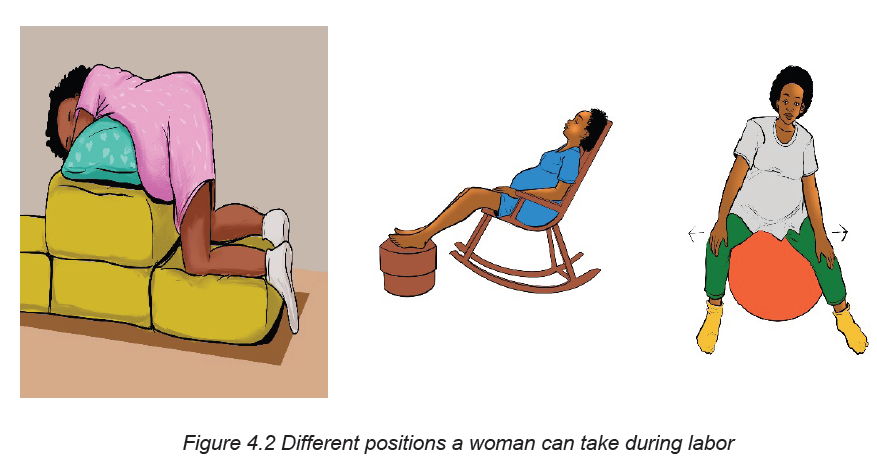
to promote the descent of the fetus. The woman’s person of choice may
assist the laboring woman to various positions and activities such as walking,
standing, sitting, squatting, leaning over a piece of furniture, or assuming ahands and knees position.
► Maternal preferences can guide the healthcare professional or her person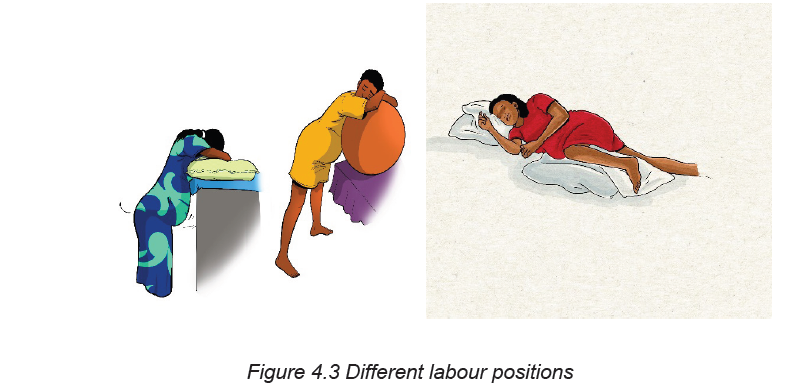
of choice in assessing which positions or activities the woman finds most
comfortable. Changes in the woman’s status may necessitate a need of bed
rest and the nurse should encourage the laboring woman to rest on her left
side to facilitate optimal uteroplacental blood flow.
In addition, position changes should be encouraged even if the woman must
remain in bed. It is important to avoid the supine position since the pressure of
the uterus on the maternal spine can cause compression of the inferior vena
cava and lead to decreased blood pressure and diminished uteroplacentalblood flow.
► Personal comfort measures: Based on laboring woman’s preferences and
needs, the nurse can provide personal comfort measures (good environment,
personal hygiene, elimination, and supportive relaxation techniques)
and encourage family members and support persons to help woman tomeet them.
• Environment: The healthcare provider will need to assess the women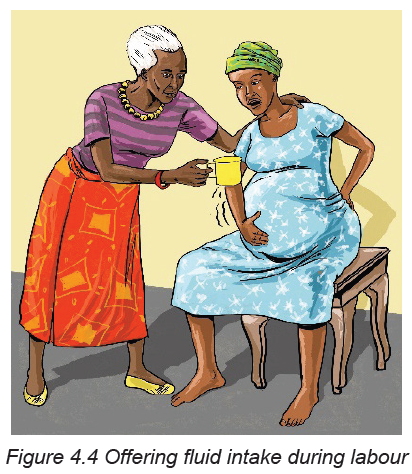
environmental preferences sun streaming, lights dimmed, intolerance to hot
and remember to turn off the fan or assess the room temperature during
childbirth to ensure that the infant does not get unnecessarily chilled.
• Personal hygiene: The nurse can help promote the patient’s sense of
cleanliness and well-being by changing pads, linens, or gown especially
if the woman is leaking amniotic fluid or bloody show. Many women who
remain ambulatory are able to perform their own personal care. However,
if the laboring woman is confined to bed or exhausted from the exertion of
labor, full assistance should be provided. Frequent mouth care should be
encouraged since dry mouth is common during labor. Providing drinks, ice
chips, popsicles, or hard candy may help to alleviate the symptoms.
• Elimination: A full bladder can inhibit the descent of the fetus and contribute
to increased pain with contractions. Encouraging and assisting the woman to
the toilet (or bedpan) to void at least every 2 hours is recommended. If the
woman is unable to void and has a distended bladder a urinary catheter may
be required.
• Supportive relaxation techniques: During labor, the healthcare providers
may encourage, assist, or teach the woman about different interventions to
help decrease pain and relieve anxiety. Relaxation techniques may include
visualization, focal points, imagery, hydrotherapy, and breathing techniques.
In addition, patients may bring items from home to enhance relaxation suchas music, a picture, or a stuffed animal.
• Anticipatory guidance: Regardless of whether or not they have attended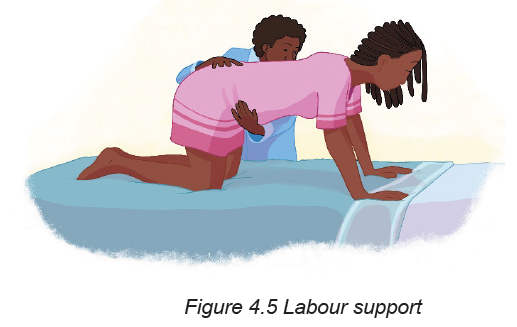
prenatal classes, most women and their families have many questions.
Women and families usually want to know what to expect. While the nurse/
midwife cannot predict exactly what will happen, helpful information can be
provided in general terms.
For example, a woman in early active labor may comment: “These contractions
are getting stronger, how strong will they get?” The nurse can empower the
woman by identifying the progress she has made to that point. Explaining
how the contractions have gradually become stronger and emphasizing how
successful the patient has been in adjusting to the changes provides factual
feedback and positive reinforcement of the progress made.
• Keeping the woman and her family informed about the process of labor and
birth is a constant and ever-changing task. For example, during the transition
phase the nurse may be teaching the woman breathing techniques to avoid
pushing with a partially dilated cervix and then with full cervical dilation, the
nurse teaches her how to push and may need to assist the woman into an
effective pushing position.
• Caring for the birth partner: Most of the nurse’s attention focuses on the
woman in labor. Efforts also should be made to help the support person feel
welcome and included whenever possible according to the woman’s wishes.
Orientation to the birth unit is helpful in identifying where to locate items such
as towels and washcloths, kitchen supplies and the restroom. Assessment of
the degree of involvement the support person would like to assume is also
important.
• Ensuring culture-centered care: It is important for nurses to remain open
minded and aware that there are a myriad of values, attitudes, beliefs, and
practices regarding childbearing that vary among cultures just as there
may be wide variations within cultures. Body language and communication
approaches provide examples of how differences in cultural practices can
be applied when caring for a woman and her family during the childbirth
experience.
Self-assessment 4.3
Max and Kate are a couple that attends the clinic and they ask a midwife on
duty to explain to them about labour support so that Kate can get a smooth and
enjoyable labour process.
1. Explain the components of the continuous labour support to Kate and Max.
4.4 Obstetric danger signs
Learning Activity 4.4
Using books and internet resources search for what can indicate a sign of danger
of a pregnant woman in the first stage of labour.
Knowledge of obstetric danger signs during labour is an important first step for
appropriate management and timely referral. Increasing knowledge of obstetric
danger signs for pregnant women would reduce delay in seeking care and improve
early detection of obstetric complications. The following are the key danger signsthat a laboring woman may present during the first stage of labour.
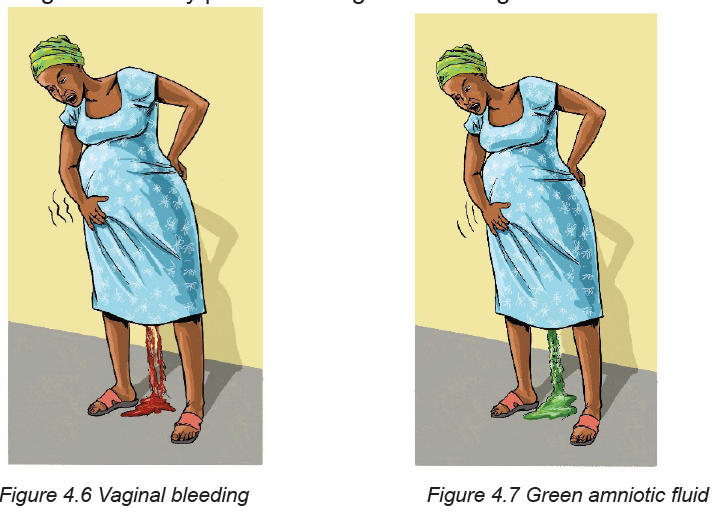
They key danger signs during labour includes severe vaginal bleeding (Figure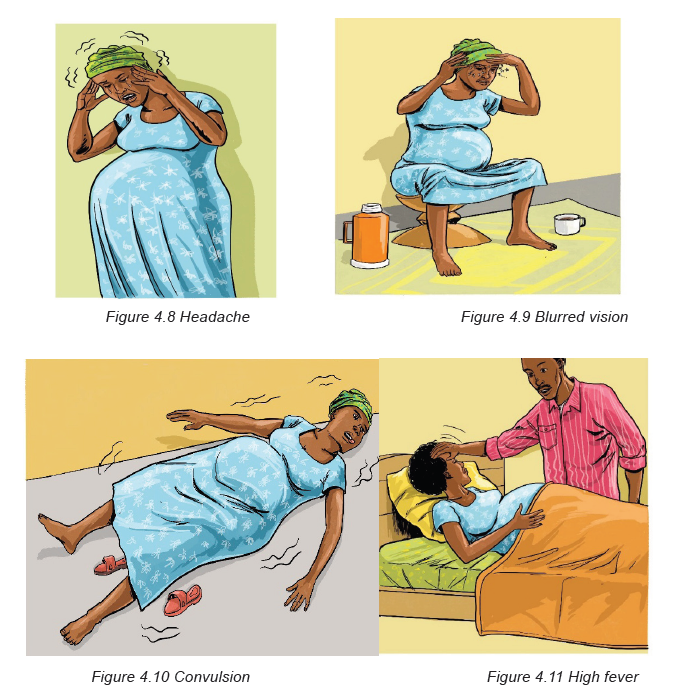
4.6) before the baby is born. Vaginal bleeding is very dangerous especially when
the bleeding is bright red because it could mean that the placenta is separating from
the uterine wall. Lack of fetal heart rate or fetal movement during labour, brown or
green amniotic fluid (figure 4.7)
Headache (Figure 4.8), blurred vision (Figure 4.9) and convulsion (Figure 4.10)
may be the results of a woman having a high blood pressure. A woman on labour
may experience also high fever (Figure 4.11), this high fever is usually a sign of
infection. Labour lasting for more than 24hours (first stage of labour) may be due
to cephalo-pelvic disproportion, malposition or malpresentation of the fetus or due
to maternal causes: insufficient contractions or inadequate pelvis.
indicates that the baby is in danger.
A woman experiencing all the above cited signs of danger is needs more attention
from healthcare and she must be transported to the nearest hospital for more
advanced obstetrical care.
Self-assessment 4.4
Zubeda is a 29 years old mother of 2 who comes in health post she stated that
she is about to give birth as her pregnancy is at term but she needs to know the
danger signs that can make her consult immediately.
1. Tell her the danger signs of the fetus and those that are maternal related
during labour.
End unit assessment 4
During labour monitoring, Olga a 23 years old prim gravida took tightly my hand
and asks me a soft drink and some snacks. Few minutes later she requested me
to rub her back because she was feeling backaches with slight lower abdominal
pain and confirm that 2 days ago a bloody show was expelled out from the
vagina. She was bed ridden for the past three days without taking anything.
“These mothers that are suffering are scaring me, it seems so hard and painful”:
She said!
“Can you please help me to get up? Now I feel better with you! At least I can cope
with my pain. Let’s turn around before the midwife come to assess me again”.
She added. As long as she continues ambulating, contractions increased, the
associate nurse continues rubbing her back, wiping her face with a cold tower and
offering drinks frequently. Suddenly Olga feels a strong contraction, and a gush
of reddish bloody amniotic fluid spreads on the flow. The associate nurse shout
out for help and the cervix was 6cm dilated and FHB were 101beats/min and the
patient was referred at the nearest district hospital for further management.
a. Throughout the scenario above remind clinical signs that characterize the
first stage of labor.
b. Compare the elements that differentiate the first and second phase of the
first stage
c. Using the text words indicate the elements that express the labor support
and monitoringd. Identify the danger signs occurred during Olga’s labor