General
- Biology SME Y2 SB File Uploaded 1/11/21, 16:48
- Biology SME Y2 TG File Uploaded 1/11/21, 16:48
UNIT 7:GAS EXCHANGE IN PLANTS, ANIMALS AND THE EFFECTS OF SMOKING
Key unit competence : Describe structures of gaseous exchange organs in plants, respiratory organs in different groups of animals and the effects of tobacco smoking on the gas exchange system.
Introductory activity 7
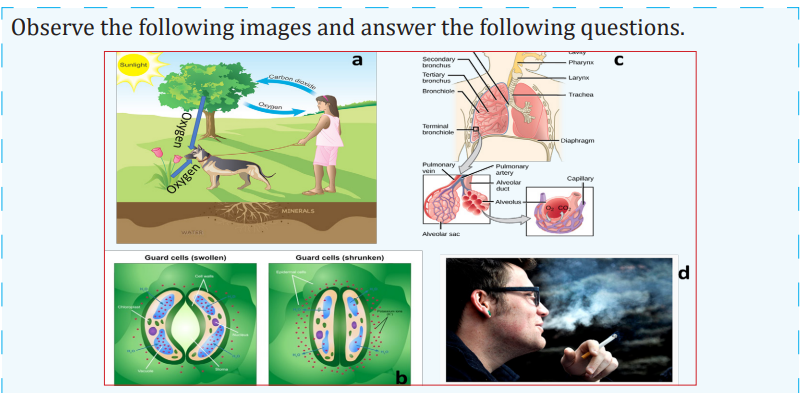
1. According to your observation, what is happening to each living organism?
2. What are the types of gas the dog is giving out?
3. Suggest the possible consequences undergone by that man who smokes.
4. Which structure are used by the plants in the process?
5. Discover the adaptations of that plant that enable the observed process to take place.
6. You are inhaling and exhaling air as shown on the figure c. Search and find the description of the pathway through which that air is passing in your body.
7.1 Gas exchange in animals and plants
Gas ehange is the one of the most impartant parts of a living orhanism in daily routine. This process is essential as it keeps that organism alive. During this process the waste product like carbon dioxide is replaced by oxygen for cellular repsitration that has been absorbed from the air through breathing and in plants the by-product of photosynthesis, oxygen is released into the air and replaced with carbon dioxide which is an essential ingredient for photosynthesis by stomata. Gas exchange is also responsible for the producing mainly oxygen as well a carbon dioxide in the air. Both plants and animals; meaning all living organisms do a form of gas exchange organs, lungs in “mammal, reptiles, birds and adult amphibians”, gills in fish and tracheae in inects. All organ for gas exchange must be kept moit by the body to be able to function. These organs differ from one another but all do essentially the same thing; they receive the carbon dioxide from the blood and release it into the air and gather oygen from the air and supply it into the blood.
7.1.1 Gas exchange in plants
Like animals, plants have breathing surfaces that are “moist, thin, cover a large surface area” and have air space in them for the gaseous diffusion to take place. Unlike animals, most the plants have very similar breathing areas and techniques and breathe in carbon dioxide and breathe out oxygen. The surface where the majority of gas exchange take plance are usually plants leaves but it can also take place in other parts like stem, roots and root hairs. Plants breath through pores in their leaves called stomata (in singular stoma).
A. Structure of stoma and theories used to explain the mechanism of opening and closure of stomata
Activity 7.1
Aim: Observation of the stomata under a light microscope
Requirements
Light microscope, glass slide, cover slip, Commelina zebrine leaves, razor blade, forceps, Pasteur dropper and iodine solution.

Procedure
i. Identify Commelina zebrina or commelina tradescantia plant nearby the school. You can also use any other monocotyledonous plant with succulent leaves.
ii. Remove a leaf from a plant. Then peel off gently the lower epidermis. It must be thin enough to allow light to pass through
iii. Smear the epidermis on a slide containing one drop of dilute iodine solution.
iv. Put on a cover slip and then observe under the lower and medium magnification.
v. Repeat the observation in morning hours and in the afternoon hours.
Questions
1. Why should the sample used in the preparation must be transparent?
2. Draw and label structures observed under light microscope.
II. Describe the theories used to explain the opening and closure of stomata present your findings in class.
a. Structure of the stoma
Stomata (stoma in singular) are microscopic pores in epidermis of the leaves and stems of terrestrial plants.
They function in gas exchange between plant and the atmosphere and in transpiration.
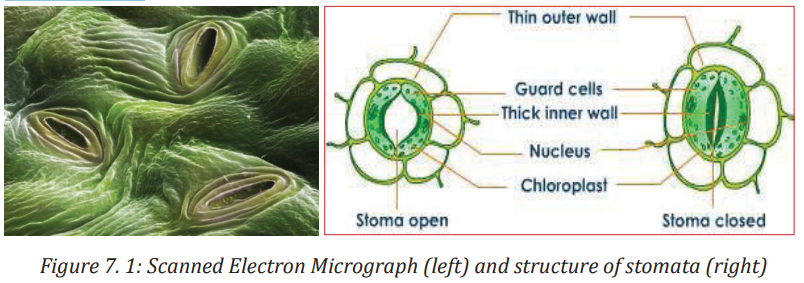
Each stoma is bordered by two saucer shaped cells called guard cells, which are specialized epidermis cells whose movements control the size of the aperture (pore). Unlike other epidermis cells, guard cells have kidney shape and have many chloroplasts. Their inner cell wall is thick and less elastic while the outer cell wall is thin and more elastic. Guard cells shrink when the plant has too little 214214 water. This closes the stomata. When the plant has enough water, the guard cells swell up again. This opens the stomata. In this way, the guard cells enable gaseous exchange. Oxygen in the atmosphere diffuses through the stomata into the air spaces between the cells of the spongy mesophyll tissue while carbon dioxide diffuses through the stomata out to the atmosphere.
b. Theories used to explain the mechanism of opening and closure of stomata
Many theories have been proposed regarding opening and closing of stomata. The four important theories of stomatal movement are the following:
i. Theory of photosynthesis in guard cells
ii. Theory of starch sugar inter-conversion
iii. Theory of glycolate metabolism and iv. Theory of active potassium pump.
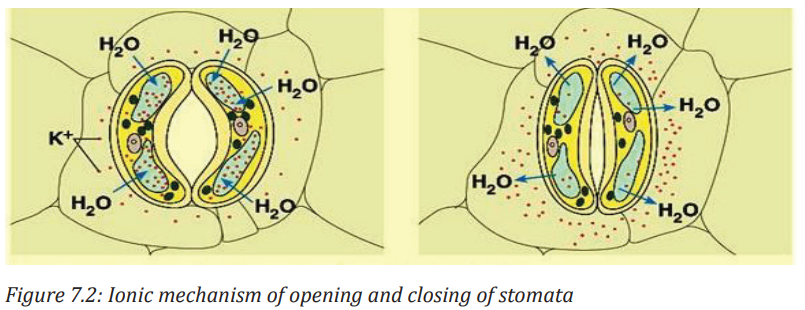
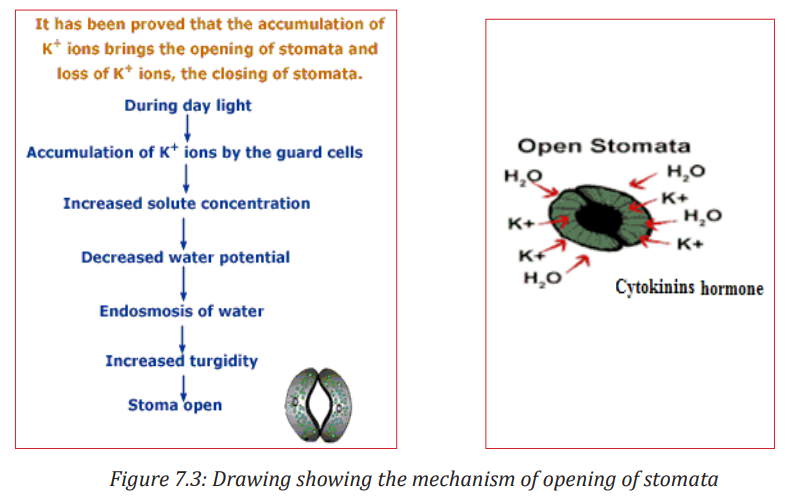
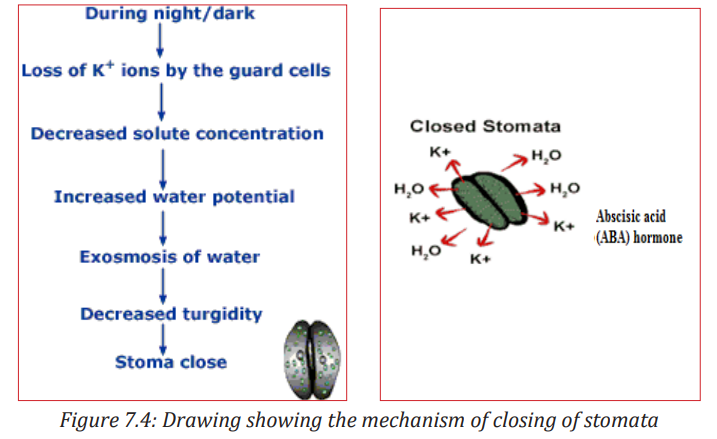
The combined outcome of the four theories shows that in general stomata open during the day (light) and close during the night (dark). But how does this happen? In light, guard cells are stimulated. They absorb K+ ions from the neighboring cells. K+ ions make the guard cells more permeable to CO2. As the guard cells perform photosynthesis, the concentration of CO2 falls and the pH rises.
Elaborated starch therefore splits into malate. The high concentration of malate and the rise of pH in guard cells develop a decrease in water potential. Hence, the guard cells withdraw water from the neighbouring cells and extend backward leaving an open pore in between whereby water is lost by evaporation.
During the night, there is no light to stimulate neither the absorption of K+ ions nor the photosynthesis. Guard cells undergo cell respiration using photosynthetic products as source of energy (carbohydrates: malate, glucose). Therefore, the concentration of malate decreases making the guard cells hypotonic than neighbouring cells. As guard-cells lose their water content, they shrive and the pore in between closes. Stomatal transpiration ceases
Plant physiologists are certain that stomatal aperture varies as a result of changes in the turgidity of the guard cells. But they are less certain about how these changes are brought about, though the following observations have been made:
a. Most stomata open during the day and close at night.
b. Some stomata show a circadian (daily) rhythm of opening and closing even when kept in constant conditions.
c. Stomata generally close when a plant suffers water stress, for example, when transpiration exceeds water absorption.
d. The stomata of some desert plants close during the day and open at night to reduce transpiration.
Plants can therefore vary the stomatal aperture. This allows a compromise between the need to conserve water and the need to exchange gases for photosynthesis.
The compensation point is the point when the rate of photosynthesis is equal to the rate of respiration. This means that the CO2 released from respiration is equivalent to that which is taken up during photosynthesis. The compensation point is reached as light intensity increases. If the light intensity is increased beyond the compensation point,
the rate of photosynthesis increases proportionally until the point of light saturation is reached, beyond which the rate of photosynthesis is no longer affected by light intensity.
For a plant under water stress, its need to conserve water is greater than its need to obtain carbon dioxide for photosynthesis. Under these conditions a plant secretes abscisic acid (ABA). This is a chemical messenger which causes stomata to close. It is thought that ABA triggers a metabolic pump which actively secretes potassium ions out of guard cells, causing the cells to lose water and become flaccid. In few words, the mechanisms of opening and closing of stomata occur in this way:
Application activity 7.1
I. Analyze the diagram below and answer to the following questions .
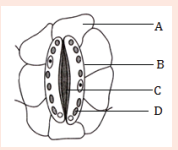
1. What title fits better to this diagram:
a. an open stoma
b. a closed stoma
c. Diagram of a guard cell and neighbouring cells
d. Diagram of a stoma and neighbouring cells
5. 2. The part labelled C is:
a. Vacuole
b. Thick inner cell wall
c. Chloroplast
d. Thin outer cell wall
3. The part which better represents the neighbouring cell is:
a. Part A
b. Part B
c. Part C
d. Part D
4. If the guard cells become more turgid, what is more likely to happen?
a. The cells A will swell
b. The pore will increase its diameter
c. The number of structures C will decrease
d. The structure B will stretch in ward
5. Which of the following statements is false about that diagram?
a. The stoma is closed
b. The inner cell wall of guard is thicker than the outer cell wall
c. There are many chloroplasts in neighboring cells
d. The guard cells have many chloroplasts.
II. Draw one diagram showing the process of opening of a stoma including an involved hormone.
B. Structural adaptation and function of stomata, lenticels, breathing roots and leaves.
Activity 7.2
Aim: Observation of leaves of aquatic and terrestrial plants.
Materials: Microscope, prepared slides of leaves of aquatic and terrestrial plants, electrical current. You can also prepare your observation sample.
Procedure
1. Place your prepared slides leaves of aquatic and terrestrial plants on the stage of the microscope.
2. Adjust for observing the leaves of aquatic and terrestrial plants.
3. Draw the leaves of aquatic and terrestrial plants.
4. Differentiate between leaves of aquatic and terrestrial plants.
II. Observe the adaptations of these plants for gas exchange.
Explain how these plants are adapted for gas exchange.
The guard cells are located in the epidermal layer of the layer of the leaf. The 2 guard cells border a stoma thereby controlling its opening and closing. The adaptations of guard cells are:
i. Guard cells have chloroplasts, they therefore carry out photosynthesis. The sugar produced offers the osmotic pressure in the guard cells. This results in the stomata opening and closing.
ii. Guard cells are bean- shaped allowing for a space between the 2 cells. The stoma enables gases to diffuse in and out.
iii. The outer walls of the guard cells are thinner than inner walls. This allows guard cells to stretch outwards when they bulge, resulting into opening of the stoma.
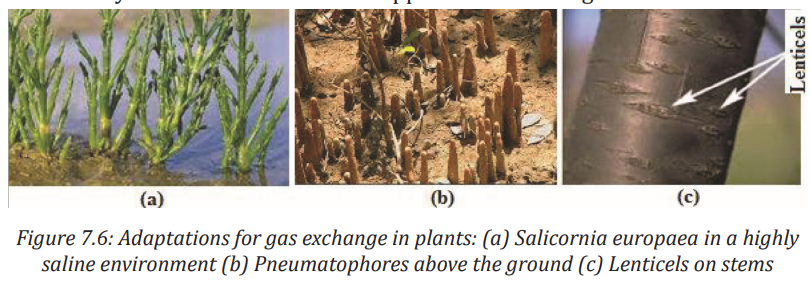
A lenticel is a porous tissue consisting of cells with large intercellular spaces in the periderm of the secondarily thickened organs and the bark of woody stems and roots of dicotyledonous flowering plants. It functions as a pore, providing a pathway for the direct exchange of gases between the internal tissues and atmosphere through the bark, which is otherwise impermeable to gases. The shape of lenticels is one of the characteristics used for tree identification: Lenticels are found as raised circular, oval or elongated areas on stems and roots. Lenticels are also found in pneumatophorous roots (respiratory or breathing roots).
The exchange of atmospheric gases is essential to photosynthesis and cell respiration. In plants, the gas exchange takes place through stomata, breathing roots, lenticels and cuticles. Most stomata are on the lower epidermis of the leaves on plants.
Unlike other plant epidermal cells, the guard cells contain chlorophyll to carry out photosynthesis. This allows the cells to expand or contract to open or close the stomata.
Guard cells swells, through the process of osmosis, to allow opening of the stomata for CO2 to enter and excess O2 and H2 O to leave, and they shrink in order to force the stomata shut either partially or completely to prevent dehydration. The number of stomata on the epidermal surface depends on the ecology of plants. Usually, plants on wet climate have fast growth and a high concentration of stomata. Plants on dry weather have lower rates of photosynthesis, lower growth and lower concentrations of stomata.
C. Structural adaptation of leaves of aquatic and terrestrial plants to their habitats
Hydrophytes(aquatic plants)
Hydrophytes or water plants are plants that grow submerged or partially submerged in water. To thrive in this environment, hydrophytes have the following features:
i. Developed stomata on large upper surface of their leaves (rather than underside) making gas exchange more efficient.
ii. Large air space to facilitate evaporation from the mesophyll. This large air filled tissue is called aerenchyma. The air in the aerenchyma reduces density giving buoyancy (ability to float) to the plant and also assist in gaseous exchange.
iii. Little or no lignified supporting tissues on the submerged parts.
iv. Poorly developed transport tissue, stems and leaves have little or no lower cuticle but large continuous air spaces, forming reservoir of oxygen and CO2 which also provides buoyancy to the plant tissues when submerged.
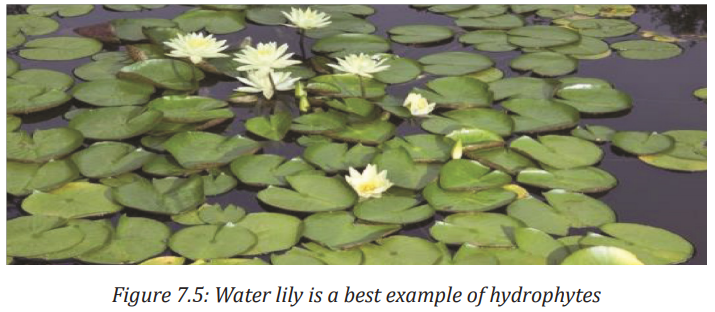
v. Emergent and floating types have broad leaves with maximum number of stomata on the upper surface to offer a large surface area for gaseous exchange and transpiration.
vi. Submerged hydrophytes have deeply dissected leaves to provide a large surface area for absorption of light energy.
Terrestrial plants
i. Mesophytes
Mesophytes are terrestrial plants plants that are adapted to grow in soil that is well supplied with water mineral salts. Such plants wilt easily when exposd to drought conditions as they are not adapted to conserve water. The majority of flowering plants are mesophytes. The following are their adaptations :
2. Show leaf mosaic that minimizes overlapping hence each leaf canopy is able to receive light energy.
3. In areas with ample water, they possess broad leaves with thick cuticle and many stomata on both leaf surfaces to encourage high rate of transpiration. - In dry/arid areas, they have more stomata on the lower side of the leaf surface to reduce water loss.
ii. Xerophytes
Xerophytic plants or xerophytes are plants that inhabit arid regions (such as a desert). They have the following adaptations:
1. They have few sunken stomata in grooves. The sunken stomata accumulate moisture in the sub-stomatal air spaces, leading to low diffusion gradient thus reducing the rate of transpiration.
2. They have ability to fix CO2 at night, so the stomata are closed during the day.
3. Epidermis folded to reduce the surface area for transpiration.
4. Leaves reduced to scales or thorns to reduce the surface area for transpiration.
5. Leaves are reduced in size such as scale leaves of whispering pine to reduce water loss.
6. Leaves have thick waxy cuticles to minimize cuticular transpiration.
7. Leaves are folded to reduce transpiration, for example, in marram grass.
8. Others have reversed stomatal rhythm to prevent excessive water loss.
iv. Halophytes
A halophyte is a plant that grows in water of high salinity and they come into contact with saline water through its roots or by salt spray, such as in saline semi-deserts, mangrove swamps, and marshes. Halophytes are adapted in the flowing ways:
1. They store water in succulent tissues which have high concentration of salt. They can thus take up water from the sea water by osmosis.
2. They have extensive air spaces throughout the stem and roots making air available to all cells, and giving buoyancy to the stem and leaves at highest tides.
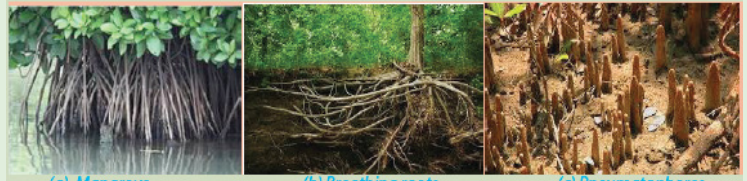
3. They develop breathing roots called pneumatophores which grow upward and protrude out of the ground. e.g. mangrove tress.
4. They have root cells that concentrate a lot of salt in them and this enables them to take in water by osmosis.
5. Some have salt glands that secrete excess salt.
6. They have pneumatophores (breathing roots) which are used to obtain atmospheric oxygen for respiration.
7. They have buttress roots for support and anchorage.
Application activity 7.2
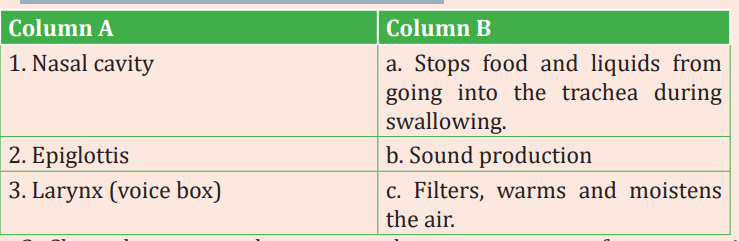
1. Associate the terms of column A and B
2. Salicornia europaea is adapted to a highly saline environment. Organize adaptations which prove this statement.
7.1.2 Gas exchange in animals
Mammals, reptiles, birds of all the shapes and size have lungs, but their lung are not always like each other, they have different shapes and structures. The lungs are made of “air filled paces and because of that they are moist and spongy”. The air route through the body of most animals is similar to one another, in general after breathing; air moves to the “naal cavity” where it becomes moist, is warmed by the capillaries and is filtered next air moves into pharynx “or the throat” which is a tube, then larynx which is the “ voice box” and is in front of the oesophagus, after that air enters the tgrachea also called :the windpipe” which like its name is pipe like structure, from there air goes into bronchi which are two smaller pipes to compared with trachea and they branch into even smaller structure called bronchioles; “because of the similarities between this branching and tree branching this is something referred to as the branchial tree.
A. Gaseous exchanges in insects, fish and amphibians
Activity 7.3
Aim: To dissect an insect (cockroach or grasshopper) and study its tracheal system.
Materials required Cockroach, dissecting microscope, surgical scissors, chloroform, forceps, scalpels, pins, dissecting tray etc.
Procedure
1. Obtain a live cockroach (Periplaneta americana) and anaesthesize it with chloroform.
2. Locate the position of spiracles on thorax and abdomen and record their position by making a rough sketch on the record book.
3. Pin the animal on the dorsal side with the ventral surface facing upwards on a dissecting tray.
4. Carefully remove the abdominal sterna (exoskeleton covering of the abdomen) without disturbing the internal tissues.
5. Remove the fat bodies and reproductive organs carefully to expose the tracheal system.
Observation
The tracheal system should be easily identified by its silvery appearance due to entrapped air in it. Can you locate the taenidia? Label the different parts of the tracheal system. Notice that in grasshopper, thoraxic spiracles are used for inspiration while abdominal spiracles are used for expiration.
II. Observe the fish and answer the following questions.
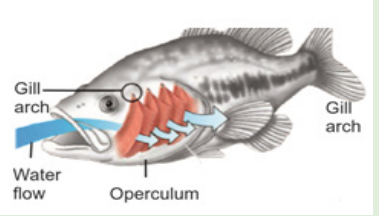
1. Search using internet and textbooks to discover and draw the labelled structures of a fish involved in gaseous exchange. 2. Observe a fish in aquaria to monitor and sequence mouth and operculum movements during gas exchange.
3. Explain on counter and parallel flow in fish.
III. Observe the amphibian and answer the following questions.

Observe a live frog or toad in a glass tank and discuss its gas exchange surfaces.
B. Gaseous exchanges in insects
Trachea in insects
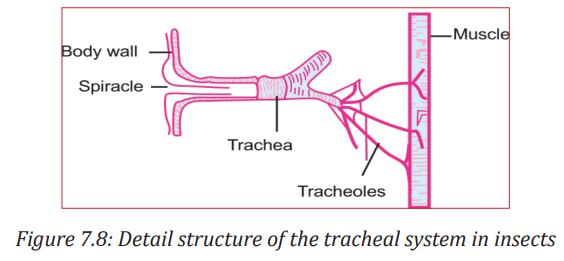
Air breathing animals (aerobic) require a continuous supply of oxygen for various metabolic activities. They also require continuous removal of carbon dioxide formed as a by-product of these metabolic activities. Insects do not breathe through their mouths as we do. The do not have lungs and, their blood which is a watery, yellowish liquid, does not carry oxygen and carbon dioxide around their bodies.
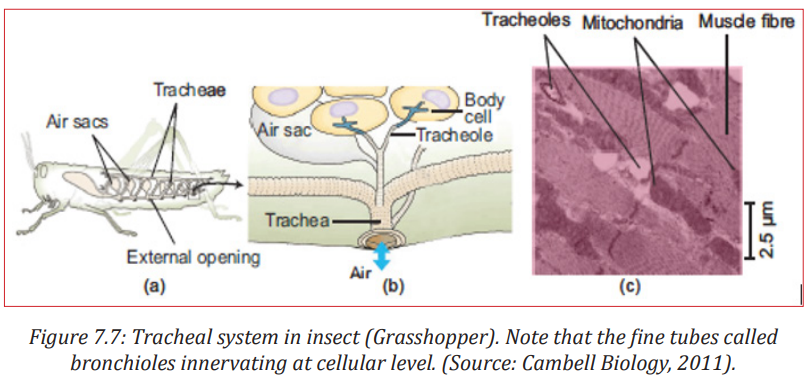
Insects have a system of tubes, called tracheae, instead of lungs. Sometimes larger tracheas have thickenings called taenidia. These are spiral cuticular layers which gives strength and elasticity. The trachea are tubes that are strengthened by rings of cuticle. These tracheae penetrate right through the insect’s body. Air enters the tracheae by pores called spiracles. These spiracles are found on each side of the insect’s abdomen.
Each segment of the abdomen has a pair of spiracles. Spiracles are respiratory openings found on the thorax and abdomen of insects. The spiracles are connected to trachea - tubes within the insect’s body. Air enters the trachea via the spiracles and the oxygen then diffuses into the insect’s body. This system consists of a vast network of cuticular (i.e., made of chitin, a long-chain polymer of an N-acetyl glucosamine) tubes penetrating to almost each individual cells of the body. This system serves two functions: it brings air into the body, and also distributes it to the cells. This pattern of tracheal system is very much similar to the system of blood vessels in higher animals.
Mechanism of Ventilation in Insects
Normally there is no active ventilation in most tracheates (i.e., animals possessing trachea). Many of the tracheates (like onychophora, myriapoda, and insect larvae and pupae) depend on simple diffusion of gases in the air tubes. But ventilation and control of direction and volume of the air flowing through the system is present in adult insects. This is because adult insects are larger and so have higher metabolic rate which demands more oxygen. The spiracles and air sacs help the insect in ventilation and creating unidirectional flow of air. In grasshopper, thoraxic spiracles are used for inspiration while abdominal spiracles are used for expiration. This creates a unidirectional flow of air. Air sacs greatly increase the efficiency of ventilation. These are balloon-like structures of the trachea with a variety of size and shape. Active ventilation is brought about by rhythmic contraction and relaxation of body walls. This forces the air movement in and out of the tracheal system. Dorso-ventral flattening of abdomen is observed in grasshopper and beetles.
C. Gaseous exchanges in fish
Gills in fish
Gills are typical respiratory organs of aquatic animals, including fishes. Gills range in shape and size. It may be finger-like projections or simple epithelial extensions. The fish have evolved in the water, so their breathing organ is also made for that environment.
They use their gills for extracting oxygen from the water; there is very little water around “three to five percent of what is on the land”. This means fish can’t get that much energy from the oxygen they breathe but they do not need that much energy as they live in water, so their respiratory organ is constantly kept moist and also by being in water, fish are in a state of almost weightlessness and do not need to keep themselves upright and in balalnced position.
These together reduce the need for energy consumption. Fish breathe through their gills that are protected by flaps of operculum on each side of the head and are made of filaments of lamellae. Lamellae are flat plates and contain the capillaries, these are the places where the gas exchange takes place. Lamellae have surface and have thin walls, so diffusion of gasses happens with ease. There are some exceptions among fishes when it comes to breathing; lung fishes are the only fishes have lungs as well as gills and adapt from Australian lungfish rely heavily on their lungs lungs for breathing and cannot use their gills that much.
Gills are more developed in fishes. Fish gills consist of thousands of highly specialised gill lamellae enclosed in a gill cavity. The gill cavity is covered by an operculum and continuously ventilated by flowing water. Respiration through gills is also known as branchial respiration. All gill surfaces are provided with a dense network of thin capillary vessels and supported by skeletal elements called the branchial arches.
Types of gills
Gills can be of two types:
External gills: These gills are exposed to the environment and not enclosed within a pouch or cavity. They are found in the larvae of many vertebrates, including lungfishes, actinopterygians, and amphibians.
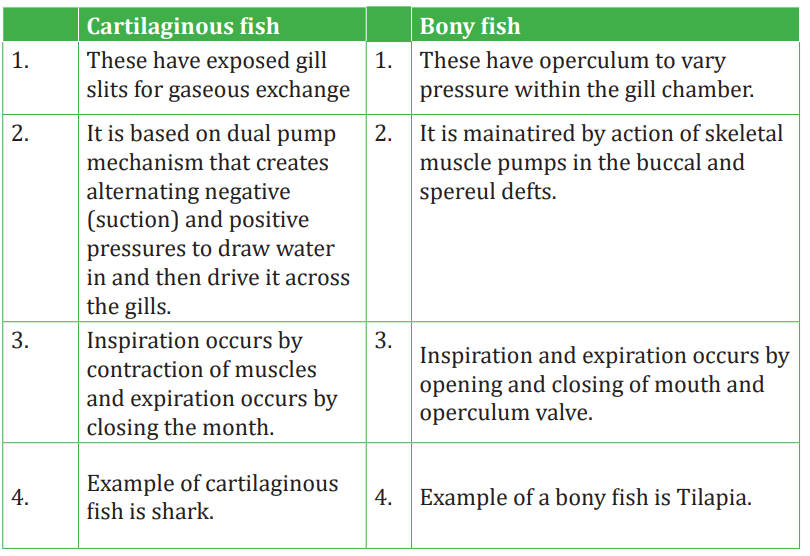
Internal gills: Gills are covered and protected laterally by soft skin folds, like the interbranchial septum in cartilaginous fishes, or by a firm operculum in many bony fishes. They are found within pharyngeal gills slits or pouches of most cartilaginous and bony fishes.
In cartilaginous fishes, the gills are found on the lateral side of the branchial arch . Gills are usually five pairs in number. They are located in vertical, anterioposteriorly compressed branchial chambers or gill pouches. Each branchial pouch is separated from each other by a stout interbranchial septum. This septum is made up of fibro-muscular tissue with blood vessels. A branchial pouch communicates to exterior with the help of narrow external branchial aperture or gill slits. Each gill has a central partition called the interbranchial septum. Within this septum, a stiff structure called gill ray gives support to the gills.
This septum is covered on each face by primary lamellae or gill filaments. Gill filaments are series of raised thin, highly vascular horizontal lamellar folds of 227 the interbranchial septum. The primary lamellae are again made up of standing rows of secondary lamellae. Water flows across their sides to irrigate the gills.
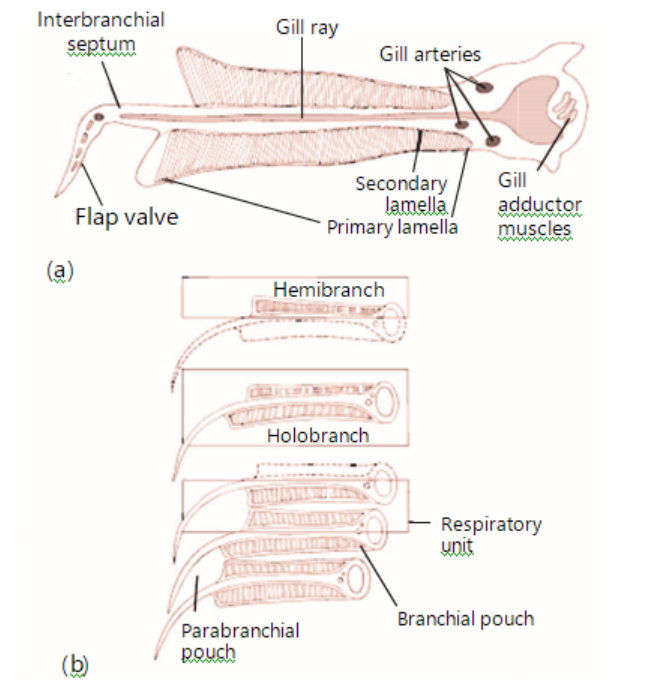
Figure 7.9: Structure of gills in shark. (Source: Kardong, Vertebrates: Comparative anatomy, Function, Evolution, 2012)
it is called a holobranch or complete gill. However, when lamellae is present on only one face, it is called a hemibranch. Facing plates of lamellae on adjacent gills constitute a respiratory unit.
A branchial pouch therefore consists of posterior hemibranch of one gill and anterior hemibranch of the succeeding gill.
The pharyngeal structural region in bony fishes is almost similar to that of cartilaginous fishes.
The gill/branchial chamber on each side is covered by a fold of integument called the operculum (gill covering). It is supported by four opercular bones. The operculum protects the branchial arches and its gill lamellae and also helps in gill ventilation. There are five pair of gill pouches and four pairs of holobranchs or complete gills. In cross section, each gill is V-shaped and composed of primary lamellae (gill filaments) that are subdivided into secondary lamellae and supported on a branchial arch.
Mechanism of Gill Ventilation
Ventilation rate is much higher in aquatic animals than air breathing animals. This is because water has lower oxygen and greater density than air. So, more ventilation is required for oxygen uptake. This is achieved in gills by having a unidirectional flow of water. Ventilation of fish gills is achieved by rhythmic movement of various muscles. This generates a continuous current of water through the gills. The muscular pump of the buccal cavity actively drives water across the internal gills bringing about ventilation. First the mouth is opened, buccal floor drops and the pharyngeal floor lowered at the same time. This creates a vacuum inside pharyngeal cavity. At the same time, external branchial openings are closed. This results in water rushing into the pharyngeal cavity through mouth. Now mouth gets closed and the external aperture opens. This makes water flow out through the branchial apertures. As water passes through the gills, it washes the gill lamellae. Exchange of gases takes place between the blood flowing in the gill lamellae and the water current.
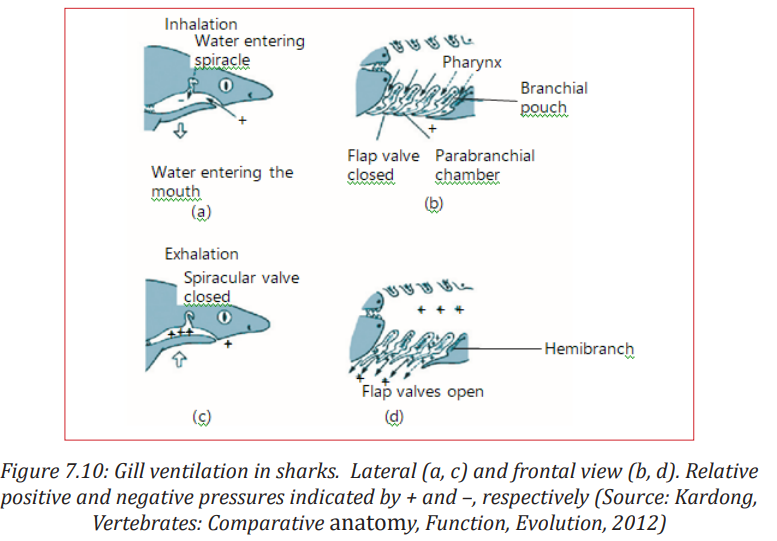
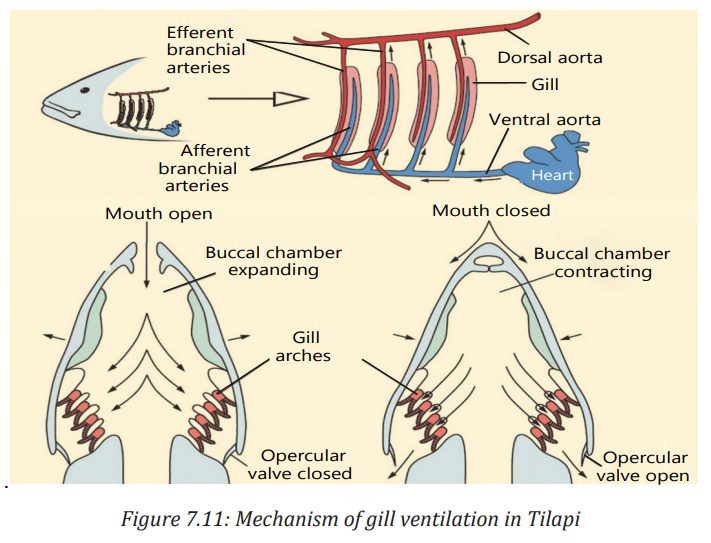
Table 7.1: Difference between gaseous exchange of cartilaginous and bony fish
Counter current mechanism
The high efficiency of fish gills, especially teleost in gas exchange is due to the presence of a counter current flow of blood and water through the system. In ‘counter current’ system, two channels in close proximity carry fluids in opposite directions. In such a system, equilibria will be established in the concentration of any permeable materials under two conditions i.e., if the channels walls are freely permeable to the particular materials and if the channels are long enough. The flow of blood in the gill lamellae and nearby water is a countercurrent type.
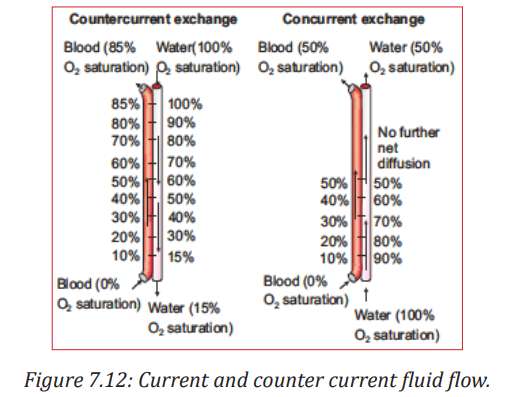
In most fish gills, the blood in the secondary lamellae flows in one direction and water flows in the opposite direction. This establishes a countercurrent exchange system. The counter current system maintains a continuous gradient of oxygen concentration between blood and water which is not found in case of concurrent exchange system.
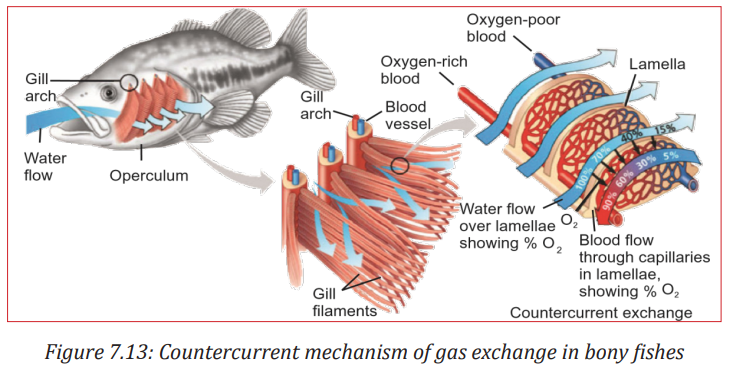
This countercurrent flow maximizes difference in oxygen (and carbon dioxide) concentration between water and blood. Countercurrent exchange arrangement results in blood always being exposed to water with a higher oxygen concentration. A diffusion gradient is, therefore, maintained across the surface of gill. Blood in gill lamellae capillaries contains less oxygen and more carbon dioxide as it comes from different tissues after metabolism.
However, the water ventilating the gills has a greater concentration of oxygen compared to that of blood. Hence, oxygen diffuses readily from water to blood in capillaries of gill lamellae continuously till equilibrium is maintained. Due to the presence of a countercurrent exchanger system, a continuous difference in the concentration of the gases is maintained all throughout the length of the gill lamellae, and therefore, a continuous efficient gas exchanger system is obtained.
Significance of countercurrent mechanism in bony fishes
• A larger difference in pO2 (i.e., partial pressure of O2 ; the pressure of a specific gas in a mixture is called its partial pressure) can be maintained across the exchange surface.
• The larger the difference, the more the exchange of gases; thus, allowing more transfer of gas.
• The system is so efficient that in some teleost 85% of oxygen may be extracted from water passing over the gills using this system.
• This type of exchanger is also found in temperature control system of cold arctic animals, in air bladders of fish and even in the kidneys of vertebrates.
• A few fish have some warm tissues. For example, Tuna have warm muscles, eyes, and brains. This is only possible because of a countercurrent blood supply to selected tissues.
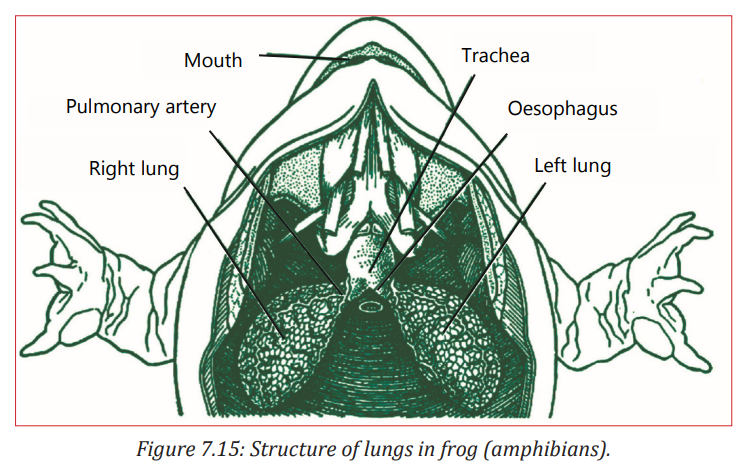
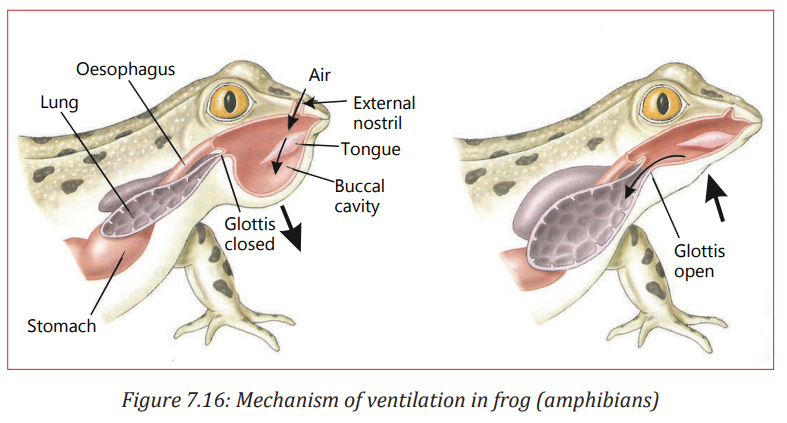
7.1. 3.Gaseous exchanges in amphibians.
Also note the continuous ventilation of the lungs when in land by alternate lowering and raising of the buccal chamber. Amphibians use the moist skin, gills or the lungs for gas exchange. Gas exchange occurring through the skin is known as cutaneous respiration. In some larval Salamanders and adult, external gills are also used for respiration. Modern amphibians rely heavily on cutaneous respiration. Sometimes, they develop accessory skin structures to increase the surface area available for gas exchange.
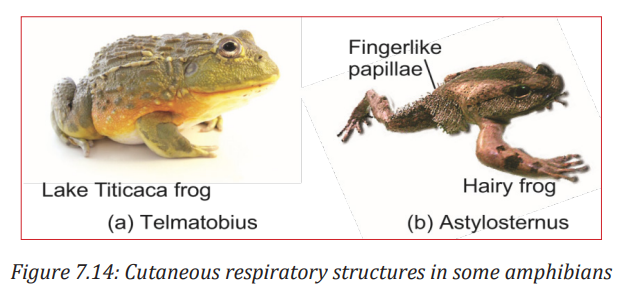
In salamanders of the family Plethodontidae, adults do not have lungs and gills. They depend entirely on cutaneous respiration for metabolism. Lake Titicaca frog, Telmatobius culeus, has prominent loose skinfolds on its back and limbs for cutaneous respiration. In the male hairy frog, Astylosternus robustus, numerous papillae appear on its sides and hindlimbs during the breeding season, forming supplementary respiratory organ. The amphibian skin is thin, moist, and rich supplied with capillaries making it best suited for gas exchange by diffusion. In aquatic amphibians, pharyngeal slits often persist with internal gills. Feathery external gills are often present, especially among larval amphibians.
Amphibian larvae like Salamander larvae typically have both internal and external gills. Pumping action of the throat irrigates the internal gills with a unidirectional stream of water across their surfaces. Feathery external gills are held out in the passing current of water. In modern amphibians, ventilation depends not on ribs but on pumping movements of the throat to irrigate gills or fill lungs.
Most adult amphibians have lungs for breathing air . Normally, the respiratory surface within the lungs on the anterior region is more developed than the posterior along the inner walls. The inner surface of lungs forms partitions and divides to increase the surface area for gas exchange. Such a surface is called septal. The interconnecting septa divide the internal wall into compartments called faveoli. These faveoli open into the central chamber within each lung. Faveoli differ from the alveoli of mammalian lungs. Alveoli are found at the end of a highly branched tracheal system but faveoli are not. Faveoli are internal subdivisions of the lung wall that open into a common central chamber. Inspired air travels along the trachea into the central lumen of the lung and from here diffuses into the surrounding faveoli. Capillaries located within the thin septal walls of the faveoli take up oxygen and give up carbon dioxide.
Application activity 7.3
1. Observe the following figure and answer the following questions.
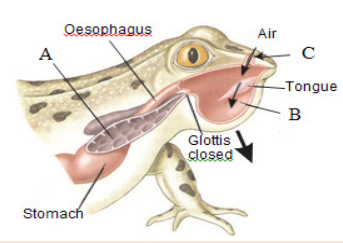
a. Identify the parts labeled A, B and C.
b. Draw this figure illustrating the organ responsible of gaseous exchange inside the body.
2. You are provided with the list of organs: gill, spiracle, operculum, skin, tracheole, air sacs.
Select the organs contributing to the gaseous exchange in fish and insect.
D. Mechanism of ventilation and gas exchange in the alveoli of humans
Activity 7.4:Research
1. Make a computer model/simulation of the human respiratory system. This can also be downloaded from the internet. Use the internet to search videos, graphics and simulation or animations showing the different part and surface of the gas exchanges system in human. Also study the process of gas exchange and the mechanism of ventilation. Now, present your finding to your classmates. You can also clay models of the respiratory system in humans.
2. Design a model of the spirometer based on its main features.
Higher vertebrates including humans have specialized organs called lungs for gas exchange.
The process of gas exchange in the body, called respiration, has three basic steps:
1. Pulmonary ventilation or breathing is the inhalation (inflow) and exhalation (outflow) of air and involves the exchange of air between the atmosphere and the alveoli of the lungs.
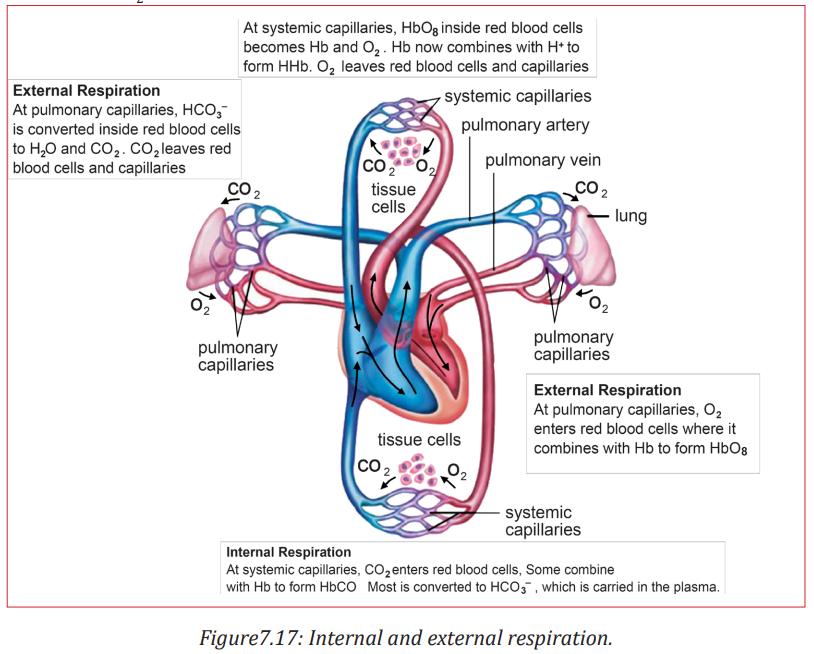
2. External (pulmonary) respiration is the exchange of gases between the alveoli of the lungs and the blood in pulmonary capillaries across the respiratory membrane. In this process, pulmonary capillary blood gains O2 and loses CO2 .
3. Internal (tissue) respiration is the exchange of gases between blood in systemic capillaries and tissue cells. In this step, the blood loses O2 and gains CO2 . Within cells, the metabolic reactions that consume O2 and give off CO2 during the production of ATP are termed cellular respiration.
a. Structure of gaseous exchange in humans
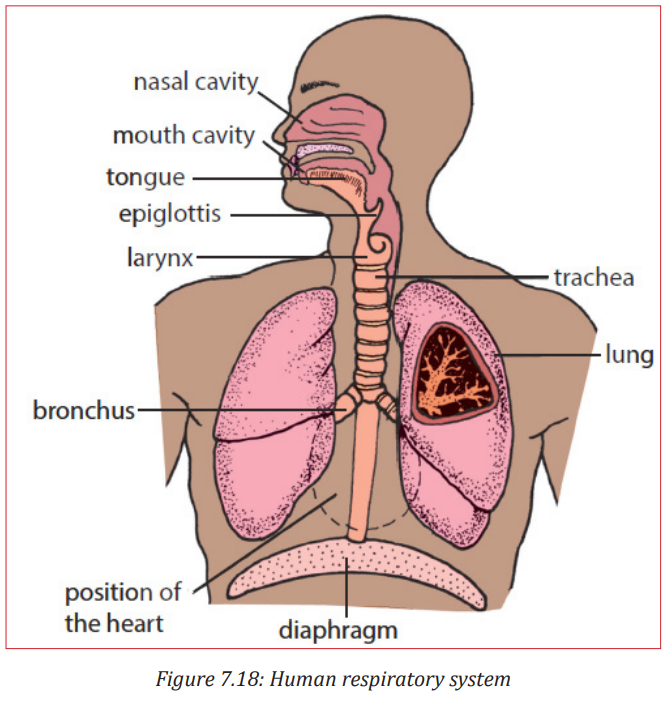
Air is inhaled through the nose into the pharynx (throat). Pharynx is a common passage for both air and food. The pharynx branches into two tubes, the oesophagus or food pipe and the larynx. The larynx is part of the airways and it houses the vocal cords. The nose, mouth, pharynx, and larynx are also called the upper airways. The larynx opens into a long tube, the trachea. The trachea then branches into two bronchi, the right primary bronchus enters the right lung and the left primary bronchus enters the left lung. The walls of the trachea and bronchi contain cartilage, which supports them and gives them their characteristic cylindrical shape. The right primary bronchus is more vertical, shorter, and wider than the left. Within each lung, the bronchi branch continuously into narrower, shorter, and more numerous tubes, more than 20 generations of branching
The primary bronchi divide to form smaller bronchi which are known as the secondary (lobar) bronchi, one for each lobe of the lung.
The secondary bronchi continue to branch, forming still smaller bronchi called tertiary (segmental) bronchi.
Tertiary bronchi divide to form smaller bronchioles. Bronchioles are without cartilage. Alveoli (explained later) first begin to appear in them attached to their walls. Alveoli normally form grapelike clusters terminally. The airways are surrounded by smooth muscle whose contraction or relaxation can alter airway radius. Bronchioles in turn branch repeatedly, and the smallest ones branch into even smaller tubes called terminal bronchioles. This extensive branching from the trachea resembles an inverted tree and is sometimes commonly referred to as the bronchial tree.
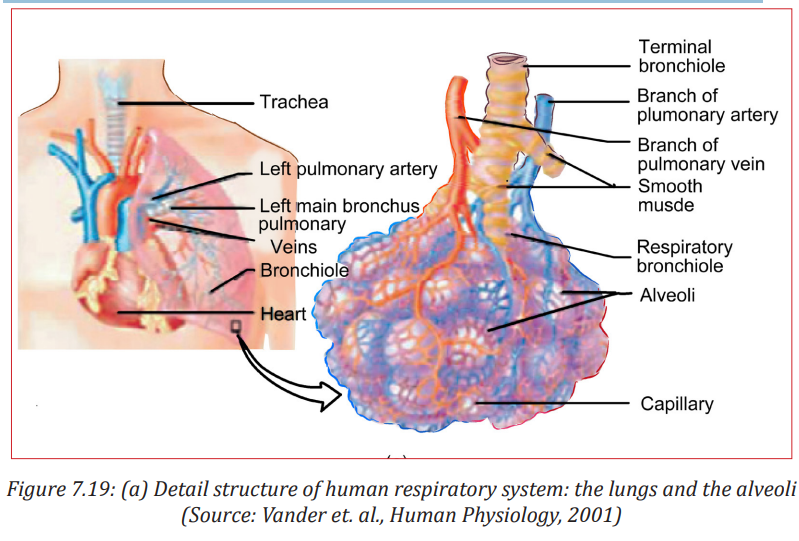
The lung is a paired cone-shaped organ in the thoracic cavity. The lungs extend from the diaphragm to just slightly superior to the clavicles (collarbone). They are guarded by the ribs anteriorly and posteriorly. The mid region of left lung also has concavity called the cardiac notch, in which the heart lies. This makes the left lung about 10% smaller than the right lung. Each lung is divided into several lobes; three lobes in right and two in left lungs. Tiny air containing sacs called alveoli (singular, alveolus) arranged like bunch of grapes at the end of each bronchioles are the respiratory unit of the lungs. Alveoli are approximately 300 million in number in an adult and are the actual sites for gas exchange.
Each lung is enclosed and protected by a double-layered serous membrane called the pleural membrane. It consists of two layers: the outer parietal pleura and the deeper visceral pleura. The space between the two is called the pleural cavity and contains a small amount of lubricating fluid secreted by the membranes. The important function of this pleural fluid is to reduce friction between the membranes during breathing movement.
b. Functions of tissues within the gas exchange system
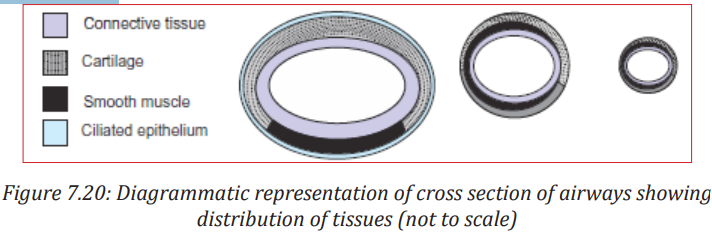
The respiratory system consists of four main layers
i. The respiratory mucosa (epithelium and supporting lamina propria)
ii. Submuscosa
iii. Cartilage and/or muscle layer
iv. Adventitia
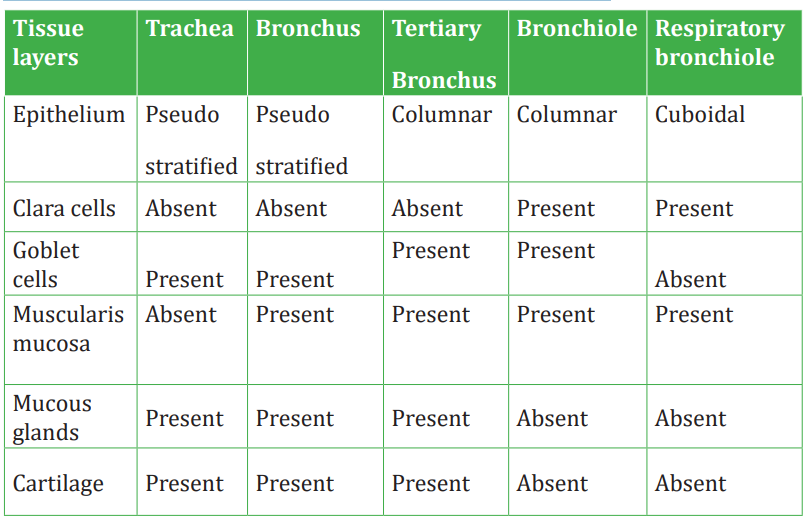
Trachea
The trachea is a wide flexible tube. The respiratory mucosa and submucosa are adapted to warm and moisten the air, and to trap particles in mucous. It consists of pseudostratifed columnar, ciliated epithelium with mucous secreting goblet cells. It has twenty C-shaped rings of hyaline tracheal cartilage which supports the trachea and keeps its lumen open. The gaps between the rings of cartilage are filled by a bundle of smooth muscle (trachealis muscle) and fibroelastic tissue. This structures together gives flexibility for ventilation. Adventitia is the outermost fibroelastic connective tissue layer.
The respiratory mucosa is made up of the epithelium and supporting lamina propria. The epithelium is tall columnar pseudostratified with cilia and goblet cells. Lamina propia lies underneath the epithelium. It contains elastin and has a supporting role. Blood vessels warm the air. The sub-mucosa contains mixed sero-mucous glands. The watery secretions from the serous glands humidify the inspired air. The mucous, together with mucous from the goblet cells traps particles from the air which are transported upwards towards the pharynx by the cilia on the epithlium. This helps to keep the lungs free of particles and bacteria. There are lots of seromucous glands in the submucosa layer.
The epithelial surfaces of the airways up to the end of the respiratory bronchioles have cilia that constantly beat toward the pharynx. They also contain mucous secreting glands . This mucous keeps the lungs clear of particulate matter and the many bacteria that enter the body on dust particles. Macrophage present in the airways and alveoli also protect against infection.
Bronchi
Bronchi have the same basic structure as trachea. A few differences are respiratory epithelium are less tall than that of trachea and contains fewer goblet cells. Lamina propia has more elastic tissue. Muscularis mucosae begin to appear lamina propia and submucosa.
There are fewer submucosal glands and cartilage is in plates. There is less cartilage in the tertiary bronchi, It does not completely encircle the lumen.
Bronchioles
The tertiary bronchii branch into bronchioles. They have a diameter of 1mm or less, and the wall structure changes. There is no cartilage and no glands. The ring of smooth muscle is arranged in discrete bundles with a variety of organisations. The epithelium is made up of ciliated columnar cells in larger 240240 bronchioles, or nonciliated in smaller bronchioles. There are no goblet cells, but there are cells called Clara cells. These are secretory cells and they secrete one of the components of surfactant.
Terminal bronchioles
The final branches of the bronchioles are called terminal bronchioles. These have a layer smooth muscle surrounding their lumens. Stimulation of the vagus nerve (parasympathetic) causes the smooth muscle to contract, and reduce the diameter of the terminal bronchioles. Small sacs are found extending from the walls of the terminal bronchi called respiratory bronchioles. These are lined by a ciliated cuboidal epithelium, and some non-ciliated cells called clara cells. The respiratory bronchii have a few single alveoli off their walls.
Alveoli
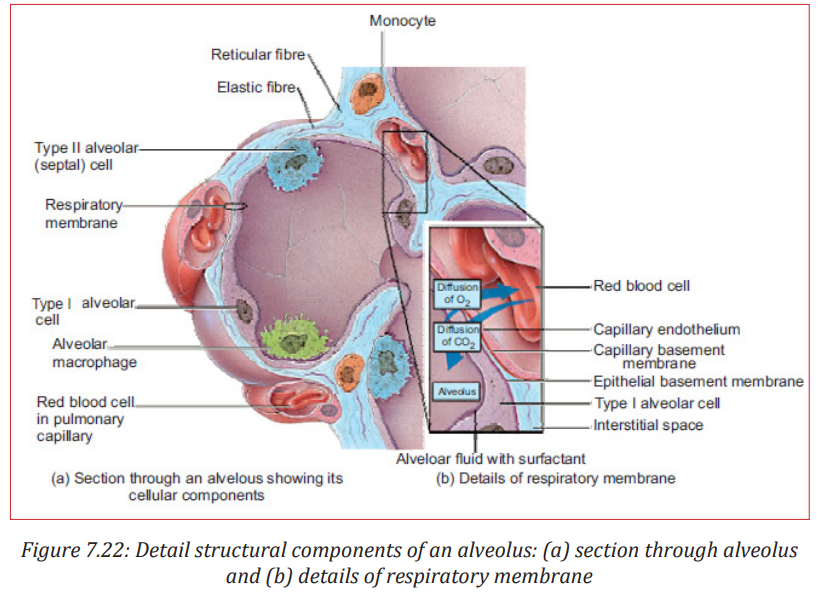
The alveoli are the sites of gas exchange with the blood. The wall of the air-facing surface(s) are lined by type I alveolar cells which is a one cell thick, continuous layer of flat epithelial cells. Type II alveolar cells are thicker specialized cells producing a detergent-like substance called surfactant and they are interspersed between type I cells.
In some of the alveolar walls, pores are present which permit the flow of air between alveoli.
The alveolar walls contain capillaries and a very small interstitial space, made of interstitial fluid and a loose meshwork of connective tissue. However, the interstitial space is absent altogether at most places and the basement membranes of the alveolar-surface epithelium and the capillary-wall endothelium fuse. As a result, the blood within an alveolar-wall capillary is separated from the air within the alveolus by an extremely thin barrier around 0.2 µm. The branching of bronchioles and the vast number of alveoli collectively increases the respiratory surface area to as much as 80 square metres. The extensive surface area of alveoli in contact with capillaries and the thin barrier results in the rapid exchange of large quantities of oxygen and carbon dioxide by diffusion.
Mechanism of ventilation (breathing)
Inspiration (inhalation or breathing in) is the movement of air from the external environment through the airways into the alveoli during breathing. Expiration (exhalation) is movement in the opposite direction. An inspiration and an expiration constitute a respiratory cycle.
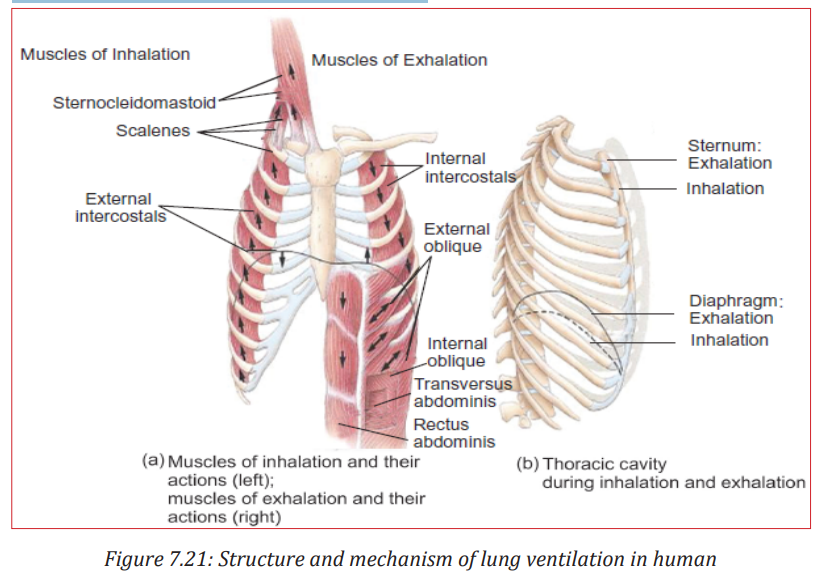
Inhalation: Air will move into the lungs when air pressure inside the lungs is less than that of outside (atmospheres). Expansion of the lungs increases the volume and so the pressure inside the lungs decreases. Expansion of the lungs 242242 during normal quiet inhalation is achieved by contraction of the diaphragm and external intercostals which are the main muscles of inhalation The diaphragm is the dome-shaped skeletal muscle that forms the floor of the thoracic cavity. Contraction of the diaphragm causes it to flatten, lowering its dome. This increases the vertical diameter of the thoracic cavity. Around 75% of air enters the lungs by this action. Also contraction of the external intercostals elevates the ribs resulting in an increase in the volume of the chest cavity. About 25% of the air that enters the lungs during normal quiet breathing is due to this action. As the volume of the lungs increases and the pressure inside the lungs (alveolar or intra-pulmonic pressure) decreases and atmospheric air rushes into the lungs.
c. Exhalation
On the other hand if the volume of the lungs decreases, pressure inside the lungs increases. As a result, air rushes out of the lungs resulting in exhalation or expiration. However, normal exhalation during quiet breathing, unlike inhalation, is a passive process because no muscular contractions are involved. Exhalation results from elastic recoil of the chest wall and lungs. Elastic recoil is the natural tendency of the chest wall and the lungs to spring back after they have been stretched. The inspiratory muscles relax with the start of exhalation. Diaphragm and external intercostal muscles also relax resulting in decrease in volume of the lungs, causing air to move out of the lungs. Interestingly, exhalation becomes an active process (requiring energy supply) only during the time of forced exhalation (for example during heavy exercise etc). During these times, the muscles of exhalation are the abdominals and internal intercostals muscles which contract to increase pressure in the abdominal region and thorax. Gas exchange in alveoli.
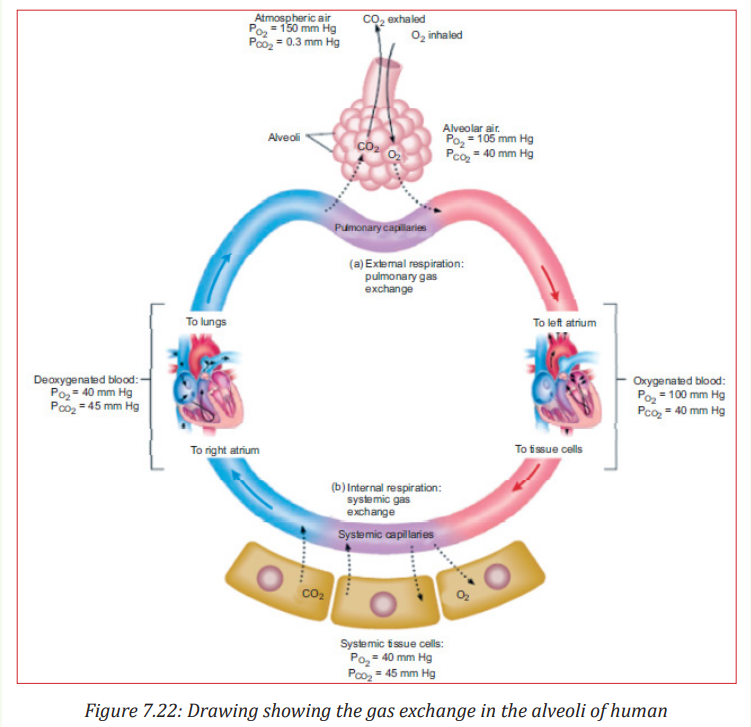
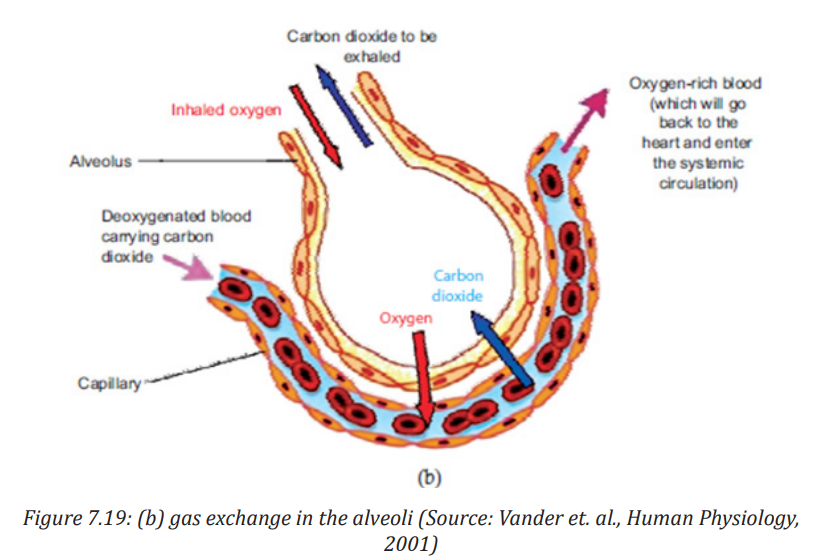
Alveoli are the respiratory units of lungs. The alveolar and capillary walls together form the respiratory membrane. The exchange of gases in the alveoli and between the air spaces in the lungs and the blood takes place by diffusion across this respiratory membrane The pressure of a specific gas (x) in a mixture is called its partial pressure (Px). The difference in partial pressures determines the movement of O2 and CO2 between the atmosphere and lungs, between the lungs and blood, and between the blood and body cells. Gas diffuses across a permeable membrane from an area where its partial pressure is higher to the area where its partial pressure is low and the rate of diffusion is directly proportional to the difference in partial pressure.
As a result of this diffusion, the capillary blood pO2 rises while its pCO2 falls. This process of diffusion continues as long as there is difference in partial pressure 244244 of the two gases between the two sides. An equilibrium is reached well before the end of the capillaries because blood flow in the capillaries is slow and gas exchange is rapid. Oxygenated blood now leaves the pulmonary capillaries to return to the heart from where it is pumped into the systemic arteries. The exchange of O2 and CO2 between systemic capillaries and tissue cells is called internal respiration or systemic gas exchange.
As stated earlier, external respiration or pulmonary gas exchange is the diffusion of O2 from air in the alveoli of the lungs to blood in pulmonary capillaries and the diffusion of CO2 in the opposite direction. In this process, blood picks up O2 from alveolar air and unloads CO2 into alveolar air as it flows through pulmonary capillaries. In a resting person, pO2 is 105 mmHg in the alveolar air which is higher than that of blood in pulmonary capillaries, where it is only 40 mmHg. This results in diffusion of O2 from alveolar air into pulmonary capillaries. However, CO2 diffuses in the opposite direction because the pCO2 of deoxygenated blood is 45 mmHg in a resting person, and the pCO2 of alveolar air is 40 mmHg. Hence, carbon dioxide diffuses from deoxygenated blood into the alveoli until the pCO2 of the blood decreases to 40 mmHg.
Application activity 7.4
1. Illustrate the diagram showing how the thoracic cavity appears during exhalation.
2. Associate the terms of column A and B
3. Show the process that occurs when oxygen moves from systemic capillary to the tissue cells for aerobic cell respiration.
7.2 Use of spirometer to measure ventilation rate and nervous control of breathing
Activity 7.5
Aim: Design a model of the spirometer based on its main features.
Materials Required
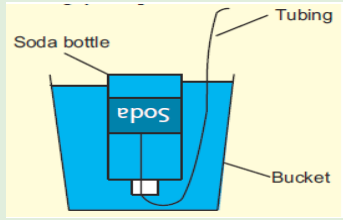
1. 2–3 litre empty soda/cold drink bottle with cap
2. One or two feet long piece of plastic tubing
3. One measuring cup with units in millilitres
4. One bucket or pan that can hold more than 3 litres of water
5. One permanent marker
Procedure
1. Marking measuring lines on the bottle: Add 500 ml of water to the soda/cold drink bottle using the measuring cup and mark a line with the marker at the top of the water level. Repeat this until the bottle is full. When the bottle is full, put the cap on the bottle.
2. Add sufficient water to the bucket or pan to submerge the soda bottle.
3. Invert the soda bottle and submerge it in the bucket, and remove the cap under the water. Open the bottle underwater to prevent any unwanted air from entering the bottle.
4. Place one end of the tubing into the soda bottle in the water, and leave the other end outside of the water.
5. Use the tubing to blow into, for determining lung capacity.
6. Remember to place the bottle in the water upside down before removing the cap.
7. Don’t forget to insert one end of the hose in the bottle after you open the cap underwater.
8. Before you exhale into the tubing, your spirometer should resemble the picture below.
9. Using the spirometer to obtain the readings:
i. One student holds the bottle to keep it from flipping over. Another student inhales normally and then exhales the air normally into the tubing connected to the spirometer. Note: Do not blow out all the “extra” air in your lungs.
ii. Note the amount of air you exhaled, remembering that each line on the bottle represents a half litre, starting from the top down.
iii. Record this volume, it is your “tidal volume.” The tidal volume is the amount of air that you normally breathe in and out.
iv. Refill the bottle with water and reinsert the tubing. One student holds the bottle while another take a few normal breaths initially. This is to get a good reading in the next step. Then inhale as much air as you can and exhale this air into the end of the tubing outside of the water. II. Use illustrations or computer aided materials to observe the role of the brain in controlling gas exchange. Search, using internet and textbooks, the role of the brain in controlling gas exchange. Then, draw a diagram showing how the brain is involved in gas exchange.
7.2.1 Spirometry
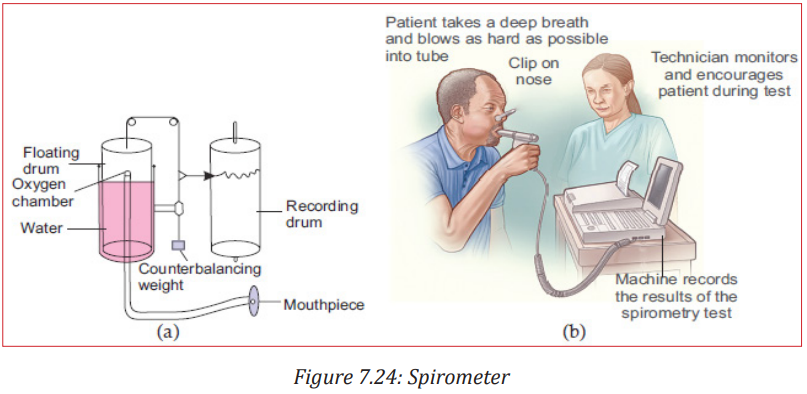
The spirometer is an apparatus for measuring inspired and expired volumes during breathing and the respiratory rate The record is called a spirogram.
Use of spirometer to measure ventilation rate
The lung volumes and capacities can be measured by routine spirometry. A typical spirometer is a tube-like instrument with an open end called the mouthpiece. The spirometer consists usually of a water-filled tank with a bell shaped floating device. A tube connects the air space within the spirometer with the airways of the person whose lung volumes is being measured. A counterweight is placed on the bell. The position of the bell indicates how much air is in the spirometer and is calibrated in volume units. A person under the test blows air into it after deep breath. Usually, the airway through nose is shut or blocked using a clip so that air can only enter or leave through the mouth. Inhalation is recorded as an upward deflection, and exhalation is recorded as a downward deflection. The bell on the spirometer rises when the person blows into the device (expiration), and falls during inspiration. If the spirometer is equipped with a recording device (spirograph), it can also be used for graphic measurement of the total ventilation per unit time. Based upon the reading indicated corresponding to each breathing in or out, an expert physician can diagnose the health of the person’s lungs and detect disorder if any.
Nowadays, the instrument is integrated with a computer system to accurately monitor the readings and give instant results.
7.2.2 Nervous control of breathing
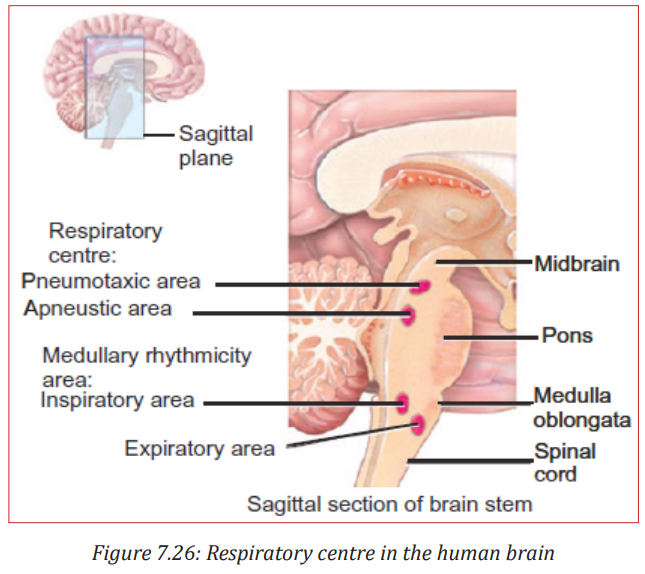
Breathing depends entirely upon cyclical respiratory muscle excitation of the diaphragm and the intercostal muscles by their motor nerves as a result of nerve impulses transmitted to them from centres in the brain. When a burst of action potentials is initiated in the nerves to the inspiratory muscles, these muscle contracts and inspiration occurs. When these action potentials stop, the inspiratory muscles relax, and expiration occurs as the elastic lungs recoil. Similarly, in situations when expiration is facilitated by contraction of expiratory muscles, the nerves to these muscles, begin firing during expiration. This neural activity is primarily controlled by neurons in the medulla oblongata.
The respiratory centre is the cluster of neurons located bilaterally in the medulla oblongata and pons of the brain stem. It can be divided into three areas on the basis of their functions.
1. The medullary rhythmicity area in the medulla oblongata:
• Controls the basic rhythm of respiration.
• There are inspiratory and expiratory areas.
• Nerve impulses generated in the inspiratory area establish the basic rhythm of breathing during quiet breathing by causing contraction of external intercostal muscle.
• The neurons of the expiratory area remain inactive during quiet breathing. However, during forceful breathing nerve impulses from the inspiratory area activate the expiratory area.
• Impulses from the expiratory area cause contraction of the internal intercostal and abdominal muscles, which decrease the size of the thoracic cavity and causes forceful exhalation.
2. The pneumotaxic area in the pons:
• Transmits inhibitory impulses to the inspiratory area.
• The major effect of these nerve impulses is to help turn off the inspiratory area before the lungs become too full of air.
• In other words, the impulses shorten the duration of inhalation. When the pneumotaxic area is more active, breathing rate is more rapid.
3. The apneustic area in the lower pons:
• This area sends stimulatory impulses to the inspiratory area that activate it and prolong inhalation.
• The result is a long, deep inhalation.
• When the pneumotaxic area is active, it overrides signals from the apneustic area.
In addition to the above, there are ‘Pulmonary stretch receptors’ in the smooth-muscle layer of the airway. They respond to stretch stimulus on this muscle. Whenever there is large lung inflation, they are activated. Electric signals in the afferent nerve fibres from the stretch receptors travel to the brain and inhibit the medullary inspiratory neurons. This phenomenon is known as the Hering-Breur inflation reflex. Thus, inspiration is terminated by feedback from the lungs. However, this pulmonary stretch-receptor reflex plays a role in setting respiratory rhythm only under conditions of very large tidal volumes, for example in rigorous exercise.
Application activity 7.5
1. Select among the following terms, those which can complete these statements:
List of terms: Lung, Spirometer , medulla oblongata, pons , Apneustic area, gill.
Statements
i. ................ is used to measure inspired and expired volumes of air.
ii. Respiratory centre is cluster of neurons located bilaterally in ................ and ................ of brain stem.
iii. ................ in brain prolongs inhalation.
2. You are provided with the sagittal section of the brain.
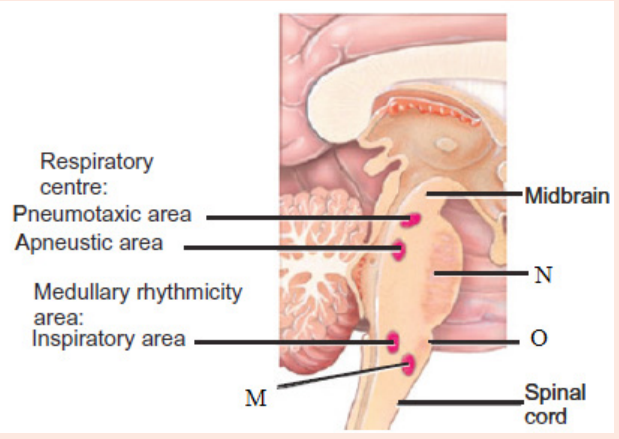
Identify the structures labeled M, N and O.
7.2.3 Lung volume and capacities
Activity 7.6
Aim: To use the illustrations of spirometer trace to define tidal volume, inspiratory reserve volume, expiratory reserve volume, vital capacity and residual volume.
Materials Required: Notebook, pen, pencil etc.
Procedure:
1. First write down the definitions of tidal volume, inspiratory reserve volume, expiratory reserve volume, vital capacity and residual volume.
2. Using a colour pencil/pen note try to locate the tidal volume in the spirometer trace provided.
3. Perform step 2 above for inspiratory reserve volume, expiratory reserve volume, vital capacity and residual volume.
4. Give a logical explanation for your labelling.
5. Show the labelled spirometer trace to your teacher and explain your results. Ask for corrections
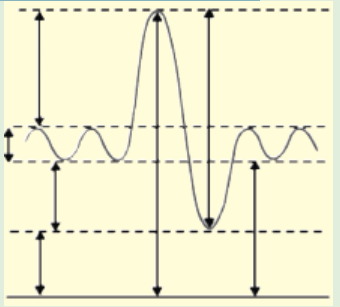
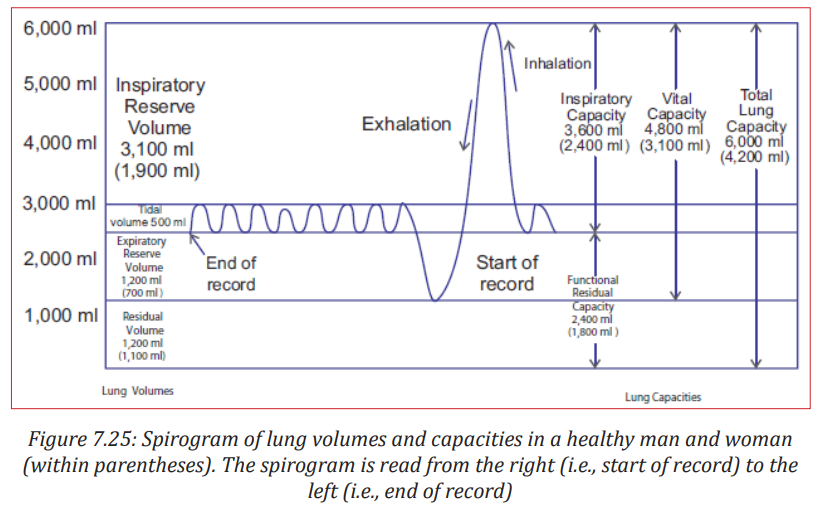
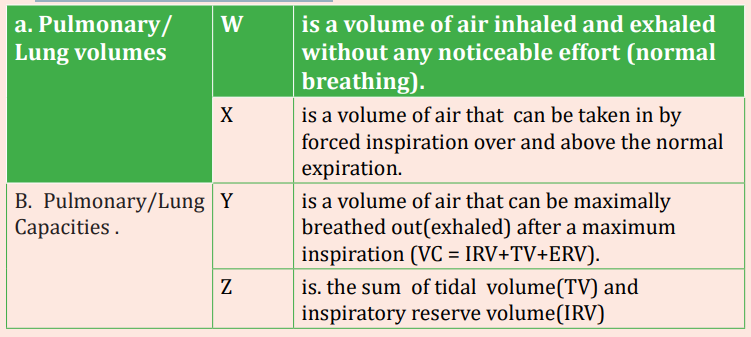
Tidal volume: It is the volume of air entering the lungs during a single inspiration during normal quiet breathing. It is about 500 ml. It is approximately equal to the volume leaving on the subsequent expiration.
Inspiratory reserve volume: The maximal amount of air that can be increased above the resting tidal volume during deepest/forced inspiration is termed the inspiratory reserve volume. It is about 3000 ml in average adult males which is six fold greater than resting tidal volume and 1900 ml in average adult females.
Expiratory reserve volume: The 500 ml of air inspired with each resting breath adds to and mixes with the much larger volume of air already in the lungs, and then 500 ml of the total is expired. However, through maximal active contraction of the expiratory muscles i.e., forced expiration, it is possible to expire much more of the air remaining after the resting tidal volume has been expired; this additional expired volume is termed the expiratory reserve volume (about 1500 ml).
Residual volume: Even after a maximal active expiration, approximately 1000 ml of air still remains in the lungs. This is because the subatmospheric intrapleural pressure keeps the alveoli slightly inflated, and some air also remains in the non-collapsible airways. This volume, which cannot be measured by spirometry, is called the residual volume and amounts to about 1200 ml in males and 1100 ml in females.
Vital capacity: It is the maximal volume of air that a person can expire after a maximal inspiration. It is a useful clinical measurement for detecting various respiratory system related conditions. It is the sum of inspiratory reserve volume, tidal volume, and expiratory reserve volume (4800 ml in males and 3100 ml in females).
Inspiratory capacity is the sum of tidal volume and inspiratory reserve volume (500 ml + 3100 ml = 3600 ml in males and 500 ml + 1900 ml = 2400 ml in females).
Total lung capacity is the sum of vital capacity and residual volume (4800 ml + 1200 ml = 6000 ml in males and 3100 ml + 1100 ml + 4200 ml in females).
However, in a normal adult only 70% (=350 ml) of tidal volume reaches the respiratory zone because of the presence of anatomical dead space. Dead Space refers to the conducting airways which have a volume of about 150 ml. Exchanges of gases with the blood does not occur in this 150 ml of the airways. It occurs only in the alveoli. Since these airways do not permit gas exchange with the blood, the space within them is termed the anatomic dead space. Thus, the volume of fresh air entering the alveoli during each inspiration equals the tidal volume minus the volume of air in the anatomic dead space.
Alveolar ventilation: The total volume of fresh air entering the alveoli per minute is called the alveolar ventilation which is given by, 253 Alveolar ventilation (ml/min) = (Tidal volume – Dead space) × Respiratory rate (ml/breath) (ml/breath) (breath/min) = (500 – 150) ml/breath × 12 breath/min = 350 × 12 = 4200 ml/min.
Importance of Lung Capacities
These pulmonary function tests are useful diagnostic tools:
An examination of ventilation function of lungs is necessary for evaluation of functional properties of human respiratory system.
It is used for estimation of defects in respiratory system and also for consideration of fitness load in sports medicine.
Various respiratory disorders may be diagnosed by comparison of actual and predicted normal values for a patient’s gender, height, and age.
Application activity 7.6
1. Use the given list, the appropriate terms to complete the following table.
- Inspiratory reserve volume (IRV)
- Tidal volume (TV)
- Expiratory reserve volume(ERV)
- Vital capacity
- Residual volume (RV)
- Functional Residual Capacity (FRC)
- Inspiratory Capacity (IC)
- Total Lung Capacity (TLC)

7.3 Effects of tar and carcinogens in tobacco smoke on the gas exchange system and symptoms of lung cancer and chronic obstructive pulmonary diseases (COPD)
Activity 7.7
I. Aim : To observe the effect of tobacco on animals.
Collect some tobacco leaves or cigarette butts and boil them with water. Allow the solution to cool. Now filter it with a stainer. Pour the solution into a large squirt bottle. Spray the solution on a plant infested with aphids. Wait for a while. Do you find the aphids stay on the plant? If no, why? what are the possible tobacco effects on human life?

II. Aim: To observe the effect of cigarette smoking.
Put some cotton bolls inside a flexible plastic bottle. Wrap some modelling clay around the cigarette as shown.
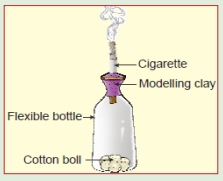
Fit the cigarette on the mouth of the bottle with the filter end inside. Light the cigarette end outside the bottle. Squeeze and release the bottle to simulate smoking. When the cigarette is almost finished, remove it from the bottle. Take out the cotton bolls on a petri dish. Touch the bolls with your finger. Do you find some black colored tar on the bolls? Where does this tar come from? Research, from the internet or the library books, the effects of smoking that cigarette or tobacco, on the gas exchange system and present their findings to your classmate.
7.3.1 Effects of tar and carcinogens in tobacco smoke on the gas exchange system
Cigarette smoking harms nearly every organ of the body, causes many diseases, and reduces the health of smokers in general. Quitting smoking lowers the risk for smoking-related diseases and can increase the longevity.
Inhaling cigarette smoke is called passive smoking and presents a health hazard to people nearby who inhale it.
Of the thousands of chemicals in tobacco smoke three important ones are:
- Carbon monoxide (CO), a poisonous gas form incomplete combustion carbon. CO in tobacco smoke combines easily, but irreversibly, with haemoglobin to form carboxyhaemoglobin and therefore reduces oxygen carrying capacity of the blood. This can lead to hypotension and heart failure.
- Nicotine, a poisonous alkaloid drug that is addictive. Nicotine in tobacco smoke stimulates the production of the hormone adrenaline by adrenal gland, leading to an increase in the heart rate and raised blood pressure. Nicotine also makes the red blood cell stickier and this leads to high risk of thrombosis and hence of the strokes.
- Tar is a sticky and brown substance. It appears in tobacco smoke minute droplets Tar in tobacco smoke is a mixture of chemicals that enter the respiratory tract. It is an irritant and causes inflammation of the mucous membranes lining the trachea, bronchi and bronchioles, resulting in producing more mucus. Tar also thickens the epithelium and paralyses the cilia on its surface. As a result, cilia cannot remove the mucus secreted by epithelium lining.
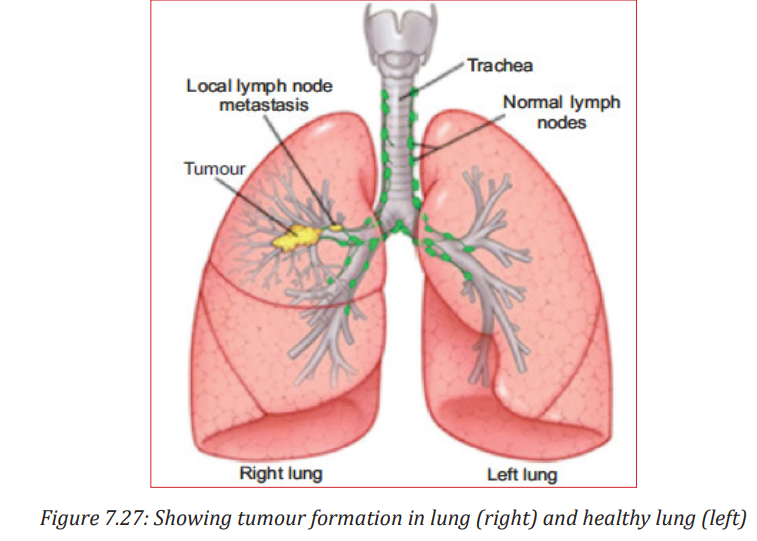
- A carcinogen is a substance capable of causing cancer in living tissue. Lung cancer is the uncontrolled growth (malignant tumor) of abnormal cells that start off in one or both lungs; usually in the cells that line the air passages. The abnormal cells do not develop into healthy lung tissue, they divide rapidly and form tumours. As tumours become larger and more numerous, they undermine the lung’s ability to provide the bloodstream with oxygen. Tumours that remain in one place and do not appear to spread are known as “benign tumours”. Malignant tumours, the more dangerous ones, spread to other parts of the body either through the bloodstream or the lymphatic system. Metastasis refers to cancer spreading beyond its site of origin to other parts of the body. When cancer spreads, it is much harder to treat successfully.
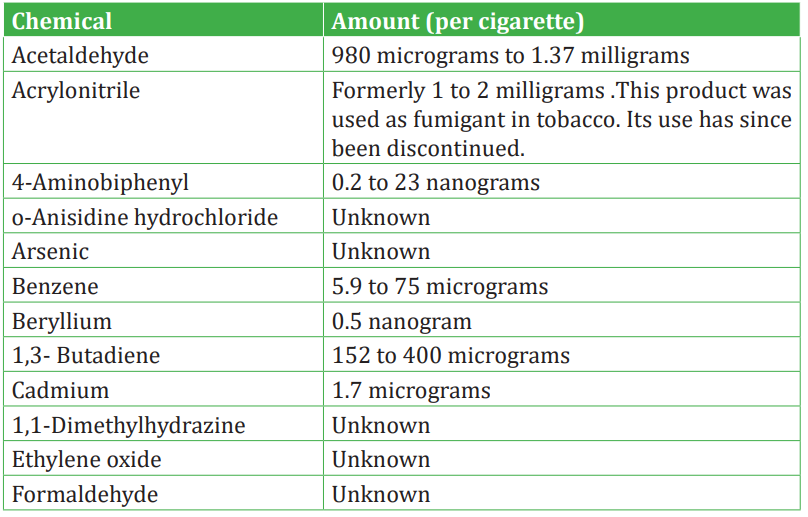
Table: List of carcinogens in cigarette smoke
7.3.2 Signs and symptoms of lung cancer
The most common symptoms of lung cancer are:
i. A cough that does not go away or gets worse
ii. Chest pain that is often worse with deep breathing, coughing, or laughing
iii.Hoarseness
iv. Weight loss and loss of appetite
v. Coughing up blood or rust-coloured sputum (spit or phlegm)
vi. Shortness of breath
vii. Feeling tired or weak
viii. Infections such as bronchitis and pneumonia that don’t go away or keep coming back
ix. New onset of wheezing
If lung cancer spreads to distant organs, it may cause:
Bone pain (like pain in the back or hips)
Nervous system changes (such as headache, weakness or numbness of an arm or leg, dizziness, balance problems, or seizures), from cancer spread to the brain or spinal cord. Yellowing of the skin and eyes (jaundice), from cancer spread to 257 the liver. Lumps near the surface of the body, due to cancer spreading to the skin or to lymph nodes (collections of immune system cells), such as those in the neck or above the collarbone.
Effect of Lung Cancer on the Lung
Tobacco smoke contains over 4,000 chemical compounds, many of which have been shown to be cancer-causing, or carcinogenic. The two primary carcinogens in tobacco smoke are chemicals known as nitrosamines and polycyclic aromatic hydrocarbons.
7.3.3 Chronic obstructive pulmonary diseases (COPD) and smoking
Chronic Obstructive Pulmonary Disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. COPD is always caused by smoking. Over time, breathing tobacco smoke irritates the airways and destroys the stretchy fibres in the lungs. It usually takes many years for the lung damage to start causing symptoms, so COPD is most common in people who are older than 60.
Other things that may put you at risk include breathing chemical fumes, dust, or air pollution over a long period of time. Secondhand smoke also may damage the lungs
The main symptoms are:
i. A long-lasting (chronic) cough.
ii. Breathing difficulty, especially during physical activities.
iii. Cough.
iv. Sputum production.
v. Wheezing.
vi. Blueness of the lips or fingernail beds (cyanosis).
vii. Frequent respiratory infections.
viii. Lack of energy.
As Chronic Obstructive Pulmonary Disease (COPD) gets worse, you may be short of breath even when you do simple things like get dressed or fix a meal. It gets harder to eat or exercise, and breathing takes much more energy. People often lose weight and get weaker. People with Chronic Obstructive Pulmonary Disease (COPD) are at increased risk of developing heart disease, lung cancer and a variety of other conditions.
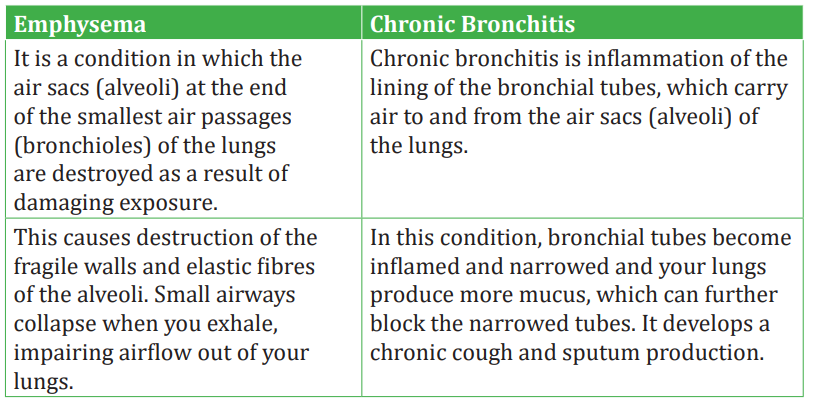
Emphysema and Chronic bronchitis are the two most common conditions that contribute to Chronic Obstructive Pulmonary Disease (COPD). It causes airway obstruction in the lungs.
Table 7.2: Comparison between emphysema and chronic bronchitis
People with Chronic Obstructive Pulmonary Disease COPD are also likely to experience episodes called exacerbations, during which their symptoms become worse than usual day-to-day variation and persist for at least several days.
• Risk factors for COPD include
i. Exposure to tobacco smoke: The most significant risk factor for COPD is long-term cigarette smoking. The pipe smokers, cigarette smokers and marijuana smokers are at risk, as are people exposed to large amounts of secondhand smoke.
ii. People with asthma who smoke: The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
iii. Occupational exposure to dusts and chemicals: Long-term exposure to chemical fumes, vapours and dusts in the workplace can irritate and inflame your lungs.
iv. Age: COPD develops slowly over years, so most people are at least 35 to 40 years old when symptoms begin.
v. Genetics: As noted above, the uncommon genetic disorder alpha-1- antitrypsin deficiency is the cause of some cases of COPD. Other genetic factors are likely to make certain smokers more susceptible to the disease.
• Complications of COPD include
i. Respiratory infections: People with COPD are more susceptible to cold, the flu and pneumonia. Any respiratory infection can make it much more difficult to breathe and could cause further damage to lung tissue.
ii. Heart problems: COPD increases the risk of heart disease, including heart attack.
iii. Lung cancer: Smokers with chronic bronchitis have a greater risk of developing lung cancer than those smokers who don’t have chronic bronchitis.
iv. High blood pressure: COPD may cause high blood pressure in the arteries that bring blood to your lungs (pulmonary hypertension).
v. Depression: Difficulty in breathing and dealing with serious illness can contribute to development of depression.
Application activity 7.7
Claudine’s parents smoke tobacco at home when they are with her but she does not smoke. After 10 years, she has the following disease symptoms:
i. A cough that does not go away or gets worse
ii. Chest pain that is often worse with deep breathing, coughing, or laughing
iii.Hoarseness
iv. Weight loss and loss of appetite
v. Coughing up blood or rust-colored sputum (spit or phlegm)
vi. Coughing up blood or rust-colored sputum (spit or phlegm)
vii. Shortness of breath
viii. Feeling tired or weak
1. Identify the disease from which she is suffering.
2. Relate her parents’s smoking and her disease
7.3.4 Effects of nicotine and carbon monoxide on the cardiovascular system, contribution of tobacco smoking to atherosclerosis and coronary heart disease related to early death.
Activity 7.8
Describe the effects of nicotine and carbon monoxide on the cardiovascular system and contribution of tobacco smoking to atherosclerosis and coronary heart disease related to early death.
a. Effects of nicotine and carbon monoxide on the cardiovascular system
You have already studied that both carbon monoxide and Nicotine along with other carcinogens affect brain and heart. They too increase the risk of developing cardio vascular diseases, which includes coronary heart disease and stroke.
• The carbon monoxide in tobacco smoke reduces the amount of oxygen in blood. This means the heart has to pump harder to supply the body with the oxygen it needs.
• The nicotine in cigarettes stimulates body to produce adrenaline, which makes heartbeat faster and raises the blood pressure, making heart work harder.
b. Contribution of tobacco smoking to atherosclerosis and coronary heart disease
Those diseases include Atherosclerosis (Arthrosclerosis) and Coronary Heart Disease (C.H.D):
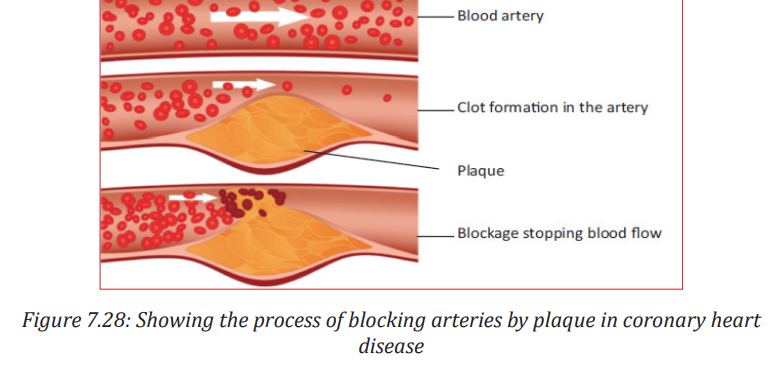
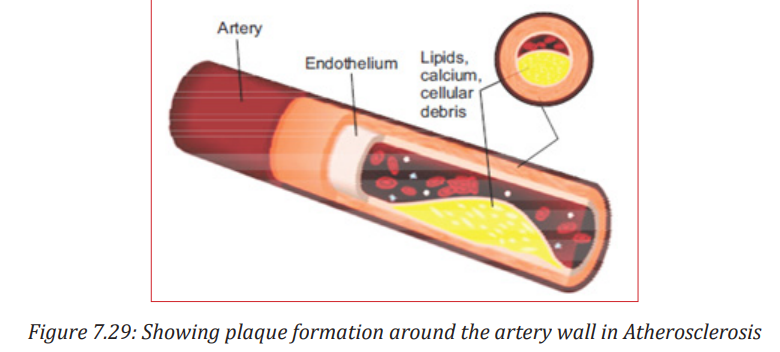
1. Atherosclerosis (or arteriosclerotic vascular disease) is a condition where the arteries become narrowed and hardened due to an excessive build up of plaque around the artery wall.
2. Coronary Heart disease, where platelets: components in the blood— stick together along with proteins to form clots which can then get stuck in the plaque in the walls of arteries and cause heart attacks. The most common symptoms of coronary artery disease are:
i. angina
ii. shortness of breath when exercising or doing other vigorous activity.
iii. Women are somewhat more likely than men to have other symptoms like nausea and back or jaw pain.
Smokers are more likely than non-smokers to develop heart disease, stroke, and lung cancer.
• Smoking is estimated to increase the risk:
i. For coronary heart disease by 2 to 4 times
ii. For stroke by 2 to 4 times
iii. Of men developing lung cancer by 25 times
iv. Of women developing lung cancer by 25.7 times
• Smoking causes diminished overall health, increased absenteeism from work, and increased health care utilization and cost.
• Smoking can make it harder for a woman to become pregnant and can affect her baby’s health before and after birth.
• Smoking increases risks for:
• Preterm (early) delivery.
i. Stillbirth (death of the baby before birth).
ii. Low birth weight.
iii. Sudden infant death syndrome (known as SIDS or crib death).
iv. Ectopic pregnancy.
• Smoking can also affect men’s sperm, which can reduce fertility and also increase risks for birth defects and miscarriage. • Smoking can affect bone health.
• Smoking affects the health of your teeth and gums and can cause tooth loss.
• Smoking can increase your risk for cataracts (clouding of the eye’s lens that makes it hard for you to see) and age-related macular degeneration (damage to a small spot near the centre of the retina, the part of the eye needed for central vision).
7.3.4 Evidence linking cigarette smoking to disease and early death
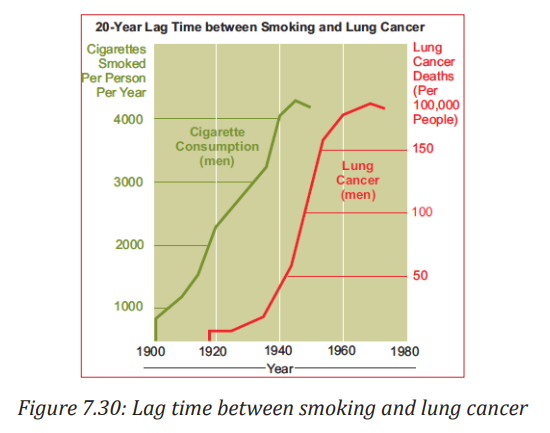
Cigarette smoking began en masse in the beginning of the twentieth century, and doctors started noticing a huge increase in cases of lung cancer from 1930 onwards, and by 1950s it was declared an epidemic.
For comparison, in 1912 there were 374 lung cancer cases, and now there are over 35,000 deaths a year, an increase of nearly 100 times.
The correlation between lung cancer and cigarette smoking is plain in the chart—it shows the 20 year ‘lag’ between the rise of cigarettes and the rise of lung cancer. Epidemiological data links smoking and cancer, and up to 50% of smokers may die of smoking-related diseases
One third of cancer deaths are as a result of cigarette smoking, and a quarter of smokers die of lung cancer. Chronic obstructive pulmonary disease is very rare in non-smokers, less than 10% of victims are non-smokers, and less than 2% of people with emphysema are non-smokers. One fifth of smokers suffer from emphysema, and as a result, deaths from pneumonia and influenza are twice as high amongst smokers.
Anti-smoking campaigns
We will continue to run ‘smoke-free’ campaigns to encourage people to change their behaviour. The campaigns are aimed at:
i. Making people aware of the health dangers of smoking.
ii. Stopping young people from taking up smoking.
iii. Encouraging smokers to try and quit, and to do so in the most effective way.
iv. Encouraging people to stop smoking in their homes and family cars— emphasizing how it affects children.
Application activity 7.8
I. Observe the following artery and answer the following questions.

1. Suggest the title of this diagram.
2. Identify C and D.
3. Interpret your observation focusing on what causes the artery to appear as it is.
II .Interpret the following graph ( 20-year lag time) between smoking and lung cancer graph focusing on relation of tobacco smoking and diseases.
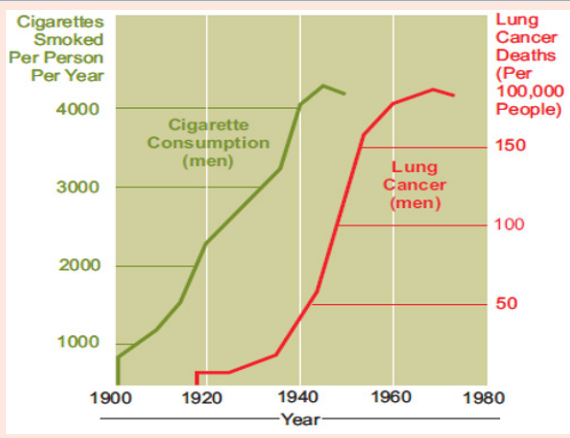
a. Interpret this graph focusing on relation of tobacco smoking and diseases.
b. Apart from cancer, identify any 2 other diseases associated with smoking.
Skills lab 7
Aim: To fight against harmful drugs such as tobacco smokes.
Materials: Tobacco plant, cigarette , match-box, capital.
Procedure
i. After getting information about the harmful effects of harmful drugs such as tobacco smokes on human health, join /found a health and social club.
ii. Tell to the club members all harmful effects of consuming those chemicals focusing on a peson’s health,family economy and country economy.
iii. Write a book or invent YouTube songs or films or comedies about all harmful drugs that particularly damage the nervous system and the body in general ; then sell them for earning money.
Portfolio Report:
i. Write your skills lab project implementation report focusing on how this skill lab has helped you to get much money and new biological skills, submit it to your teacher
End unit assessment 7
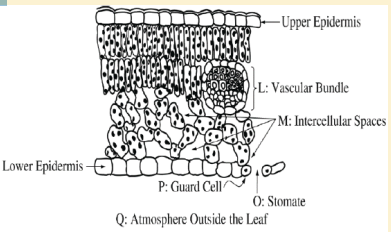
Analyze the diagram and then choose the correct answer. Transpiration in the leaf depends on the transport of potassium ions into:
a. Into O
b. Into P
c. From M to L
d. From M to Q
e. From P to L.
2. The theory that says than during the light time, potassium pumps open and this brings about diffusion of CO2 from the atmosphere to the guard cells for photosynthesis is called:
a. Theory of photosynthesis in guard cells
b. Theory of starch sugar inter-conversion
c. Theory of glycolate metabolism
d. Theory of active Potassium Pump.
3. What is the main difference between the guard cells and the other epidermal cells?
a. Guard cells have chloroplast while the remaining epidermal cells have no chloroplast
b. Guard cells have oval shape while other cells have cubic shape
c. Guard cells are beneath the spongy mesophyll
d. Guard cells are covered by a transparent cuticle
4. Water lily is:
a. Xerophytes
b. Halophyte
c. Hydrophyte
d. Helophytes
5. Mangroves are plants adapted to estuaries or marine region with high salinity.What statement does not describe the adaptations of mangroves?
a. The presence of lenticels that help in gas exchange and evaporation
b. Presence of large number of stomata on the upper side of the leaves
c. The presence of pneumatophores which are breathing roots.
d. Presence of succulent tissues that have high concentration of salt
6. Explain how gaseous exchange occurs in the leaf.
7. Describe the tracheal system of insects and relate to its function.
8. Describe the structure of the gills in relation to its function.
9. Describe the mode of gaseous exchange in amphibians.
10. Calculate vital capacity and alveolar ventilation from the data provided.