UNIT 6 MEDICAL PATHOLOGIES OF NEUROLOGICAL SYSTEM
Key Unit Competences
To take an appropriate decision on management of common pathologies ofNeurological system (Headache, Migraine, and Epilepsy)
Introductory activity 6.0
Carefully observe the picture below and answer the following questions:
Figure 6.1 Person with neurologic disorder
1. What are the abnormal observations can you recognize from this person?
2. What might be the pathologies that this person might be experiencing?
The nervous system is divided into two anatomic divisions: the central nervous
system (CNS) and the peripheral nervous system (PNS). The basic structure of the
nervous system is the nerve cell or neuron. Neurons are either sensory or motor.
Sensory neurons transmit impulses to the CNS; motor neurons transmit impulses
from the CNS. The nervous system consists of the brain, spinal cord, and peripheral
nerves. It is responsible for coordinating body functions and responding to changes
in or stimuli from the internal and external environment. Changes in the functioning
of the nervous system can profoundly affect the entire body.
Neurological disorders are diseases of the central and peripheral nervous system.
In other words, the brain, spinal cord, cranial nerves, peripheral nerves, nerve
roots, autonomic nervous system, neuromuscular junction, and muscles. Thesedisorders include epilepsy, Alzheimer disease and other dementias, cerebrovascular
diseases including stroke, migraine and other headache disorders, multiple
sclerosis, Parkinson’s disease, neuroinfections, brain tumours, traumatic disorders
of the nervous system due to head trauma, and neurological disorders as a result
of malnutrition. Examples of symptoms include paralysis, muscle weakness, poor
coordination, loss of sensation, seizures, confusion, pain and altered levels of
consciousness. The specific causes of neurological problems vary, but can include
genetic disorders, congenital abnormalities or disorders, infections, lifestyle or
environmental health problems including malnutrition, and brain injury, spinal cordinjury or nerve injury.
6.1 HEADACHE/CEPHALGIAS
Learning Activity 6.1
Carefully read the clinical case scenario and answer the followingquestions:
A 31-yr-old woman comes to the emergency department because of a severe
headache in the occipital region. She says the headache began suddenly about
1 h ago, and she describes it as “the worst headache of my life.” She says the
pain is constant and is accompanied by nausea but not vomiting. She deniesvisual symptoms, focal weakness, and problems with gait and balance.
She has frequently had similar headaches beginning about 2years ago. The
headaches have increased in frequency this past week, and this episode is by
far the worst. She says the headaches start suddenly, last about an hour, and
are associated with palpitations, unexplained anxiety, and light-headedness.
She has also had nausea and occasional swelling of the neck during these
episodes. The headaches are usually associated with exertion or with straining
during bowel movements but sometimes occur without any provocation. She
has not been evaluated for these headaches before. The woman who appears
uncomfortable because of headache, and her vital signs are temperature: 37.6°
C, pulse: 104 beats/min, BP: 150/90 mmHg, respiration rate: 20/min, oxygen
saturation of 99% on room air. She was given paracetamol 1gr TDS for 5 days,
advised to have rest for 4 days and CT scan was ordered.
1. What were abnormal signs and symptoms that the patient was presenting?
2. What might be some risk factors to the development of those symptoms?
3. What investigation was requested to lure out the cause of those symptoms?4. What was included into her plan of management?
Headache is among the most common reasons that patients seek medical
attention. A classification system developed by the International Headache Society
characterizes headache as primary or secondary.
Primary headaches are those in which headache and its associated features are
the disorder in itself. E.g. Migraine, Tension-type, exertional- type.
Secondary headaches are those caused by exogenous disorders. E.g. Systemic
infection, Head injury, Vascular disorders, Subarachnoid hemorrhage, Brain tumor.Causes, risk factors and pathophysiology
Headache pain results from signals interacting among the brain, blood vessels and
surrounding nerves. During a headache, an unknown mechanism activates specific
nerves that affect muscles and blood vessels. These nerves send pain signals tothe brain.
Migraines result when unstable nerve cells overreact to various factors (triggers).
The nerve cells send out impulses to blood vessels and cause chemical changes inthe brain. The result is disabling pain.
The patient who presents with a new, severe headache (acute, new-onset
headache) has a differential diagnosis that is quite different from the patient with
recurrent headaches over many years. In new-onset and severe headache, the
probability of finding a potentially serious cause is considerably greater than in
recurrent headache. Patients with recent onset of pain require prompt evaluation and
often treatment. Serious causes to be considered include meningitis, subarachnoid
hemorrhage, epidural or subdural hematoma, glaucoma, and purulent sinusitis.
Headaches have a tendency to run in families, especially migraines. Children who
have migraines usually have at least one parent who also suffers from them.
Headaches can also be triggered by environmental factors shared in a family’s
household, such as eating certain foods or ingredients (caffeine, alcohol, fermented
foods, chocolate and cheese, etc), exposure to allergens, secondhand smoke,
strong odors from household chemicals or perfumes. Common triggers of tension
headaches or migraines include alcohol use; dehydration, changes in eating or
sleeping patterns; depression; emotional stress related to family and friends, work
or school; excessive medication use; eye, neck or back strain caused by poor
posture; lighting; noise or weather changes.
Headaches in children: for about 20% of them, tension headaches and migraines
are a reoccurring problem. Similar to adults, triggers for headaches in children
include certain foods that trigger headaches for the individual, changes in sleep,environmental factors and stress.
The brain itself is not sensitive to pain, because it lacks pain receptors. However,
several areas of the head and neck have pain receptors and can thus sense pain.
These include the extracranial arteries, middle meningeal artery, large veins,
venous sinuses, cranial and spinal nerves, head and neck muscles, the meninges,
falx cerebri, parts of the brainstem, eyes, ears, teeth and lining of the mouth. Pial
arteries, rather than pial veins are responsible for pain production.
Headaches often result from traction to or irritation of the meninges and blood
vessels. The pain receptors may be stimulated by head trauma or tumors and
cause headaches. Blood vessel spasms, dilated blood vessels, inflammation or
infection of meninges and muscular tension can also stimulate pain receptors. Once
stimulated, a nociceptor sends a message up the length of the nerve fiber to the
nerve cells in the brain, signaling that a part of the body hurts. Primary headaches
are more difficult to understand than secondary headaches. The exact mechanisms
which cause migraines, tension headaches and cluster headaches are not known.
Migraines are currently thought to be caused by dysfunction of the nerves in thebrain.
Signs and symptoms
Headache signs and symptoms vary depending on the type of headache:
Tension headaches: tension headaches are the most common type of
headache. Tension headache pain tends to be consistent without throbbing, mild
to moderate, on both sides of the head (bilateral), responsive to over-the-counter
treatment, worse during routine activities (such as bending over or walking upstairs).
Migraines: migraines are the second most common type of primary headaches.
Symptoms of migraine include moderate to severe pain, nausea and vomiting,
pounding or throbbing pain, pain that lasts four hours to three days, sensitivity to
light, noise or odors, stomach upset or abdominal pain.
Cluster headaches: cluster headaches are the most severe type of primary
headache. Cluster headaches come in a group or cluster, usually in the spring or
fall. They occur one to eight times per day during a cluster period, which may last
two weeks to three months. The headaches may disappear completely (go into
remission) for months or years, only to recur later. The pain of a cluster headache
is intense with a burning or stabbing sensation, located behind one of your eyes or
in the eye region, without changing sides, throbbing or constant.
New daily persistent headaches: new daily persistent headaches (NDPH) come
on suddenly and last for more than three months. They typically occur in people
who weren’t having frequent headaches before. The pain of NDPH is constant and
persistent without easing up, located on both sides of the head, not responsive tomedications.
Sinus headaches: sinus headaches are the result of a sinus infection, which
causes congestion and inflammation in the sinuses (open passageways behind
the cheeks and forehead). People, and even healthcare providers, often mistake
migraines for sinus headaches. Symptoms of sinus headaches include bad taste
in mouth, deep, constant pain in your cheekbones and forehead, facial swelling,
feeling of fullness in ears, fever, pain that gets worse with sudden head movement
or straining, mucus discharge (snot).
Some headache symptoms that suggest a serious underlying disorder and that
require immediate medical care are those with a sudden, new, severe headache;
a headache that is associated with neurological symptoms such as weakness,
dizziness, sudden loss of balance or falling, numbness or tingling, paralysis,
speech difficulties, mental confusion, seizures, personality changes/inappropriate
behavior, or vision changes (blurry vision, double vision, or blind spots); headache
with a fever, shortness of breath, stiff neck, or rash; headache pain that awakens
you up at night; headaches with severe nausea and vomiting; headaches that occurafter a head injury or accident; getting a new type of headache after age 55.
Secondary headaches from: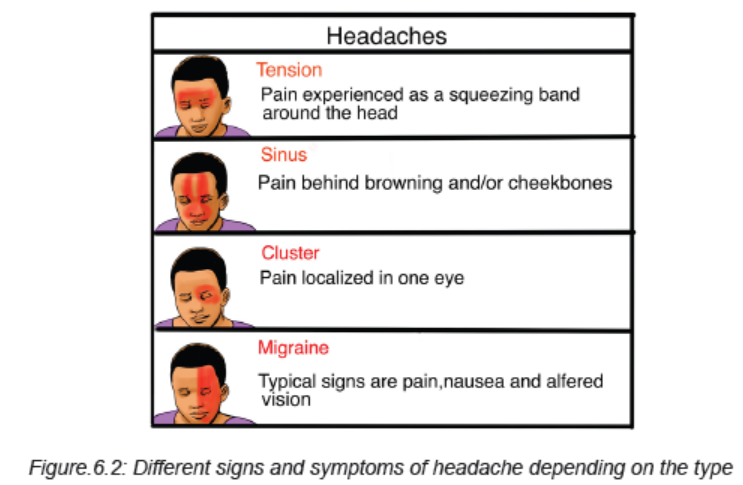
Meningitis: acute, severe headache with stiff neck and fever suggests meningitis.
Lumbar Puncture is mandatory. Often there is striking accentuation of pain with
eye movement. Meningitis can be easily mistaken for migraine in that the cardinal
symptoms of pulsative headache, photophobia, nausea, and vomiting are present.
Intracranial Hemorrhage: acute, severe headache with stiff neck but without fever
suggests subarachnoid hemorrhage. Rarely, if the hemorrhage is small or below the
foramen magnum, the head CT scan can be normal. Therefore, Lumbar Puncturemay be required to definitively diagnose subarachnoid hemorrhage.
Brain Tumor: approximately 30% of patients with brain tumors consider headache
to be their chief complaint. The head pain is usually an intermittent deep, dull aching
of moderate intensity, which may worsen with exertion or change in position and
may be associated with nausea and vomiting. The headache of brain tumor disturbs
sleep in about 10% of patients. A history of amenorrhea or galactorrhea should lead
one to question whether a prolactin-secreting pituitary adenoma is the source of
headache. Head pain appearing abruptly after bending, lifting, or coughing can be
due to a posterior fossa mass (or a Chiari malformation).
Temporal arteritis: head pain may be unilateral or bilateral and is located
temporally in 50% of patients but may involve any and all aspects of the cranium.
Pain usually appears gradually over a few hours before peak intensity is reached.
The quality of pain is only seldom agonizing; it is almost invariably described as dull
and boring, with superimposed episodic sharp pains similar to those that appear in
migraine. The pain is usually superficial, external to the skull, rather than originating
deep within the cranium. Scalp tenderness is present, often to a marked degree;
brushing the hair or resting the head on a pillow may be impossible because of
pain. Headache is usually worse at night and often aggravated by exposure to cold.
Glaucoma: glaucoma may present with a prostrating headache associated with
nausea and vomiting. The headache often starts with severe eye pain. On physicalexamination, the eye is often red with a fixed, moderately dilated pupil.
Investigations
Investigating headache might focus on:
Obtaining complete medical history and performing the holistic physical examination
where to look for signs and symptoms of an illness that may be causing the headacheand neurological examination and neurological tests.
Although scans and other imagining tests can be important when ruling out
other diseases, they do not help in diagnosing migraines, cluster or tension-type
headaches. However, if the healthcare provider thinks that the headaches are being
caused by another medical condition, there are several imaging tests that may be
done like a CT Scan or MRI (if headaches are connected to an issue with the central
nervous system. Both of these tests produce cross-sectional images of the brain
that can show any abnormal areas or problems). An EEG (electroencephalogram)may also be needed. Electromyography
Electromyography (EMG) studies the changes in the electrical potential of muscles
and the nerves supplying the muscles. An EMG is useful in determining the presenceof neuromuscular disorders.
Lumbar Puncture: changes in CSF occur in many neurologic disorders. A lumbar
puncture (spinal tap) is performed to obtain samples of CSF from the subarachnoid
space for laboratory examination and to measure CSF pressure. Bacteriologic tests
on specimens of CSF reveal the presence of pathogenic microorganisms. Strictaseptic technique is required during the procedure.
Other laboratory investigations might be helpful especially if there is high suspiciousof other underlying factors/causes.
Plan of treatment of headache
One of the most crucial aspect of treating headaches is figuring out the triggers,
and once the triggers are known, the treatment choices can be very easy. Triggers
are very specific to each person and once every patient determines his/her triggers,he/she can avoid or minimize them.
Counseling and stress management techniques can help the patient to handle
the triggers better. By lowering the stress level, patient can avoid stress-induced
headaches. Stress management teaches the patient ways to cope with stressful
situations. Relaxations technics are helpful in managing stress. Patient can use
deep breathing, muscle relaxation, mental images and music to ease the tension.
Biofeedback teaches the patient to recognize when tension is building in the
body. During biofeedback, sensors are connected to the body. They monitor the
involuntary physical responses to headaches, which include increases in breathingrate, pulse, heart rate, temperature, muscle tension, and brain activity.
Not every headache requires medication. Occasional tension headaches usually
respond well to NSAIDs (paracetamol, ibuprofen, etc), but be aware that using
these medications too often can lead to a long-term daily headache. For frequent orsevere headaches, the triptans and other types of drugs can stop a migraine attack.
Drugs for high blood pressure, seizures and depression can sometimes prevent
migraines. The healthcare provider may recommend trying one of these medicationsto reduce headache frequency.
6.2 MIGRAINE
Migraine headaches are chronic headaches that can be significant for hours or
even days. Symptoms can be very severe and it may be necessary to find a dark,
quiet place to lie down. It is usually an episodic headache that is associated with
certain features such as sensitivity to light, sound, or movement; nausea and
vomiting often accompany the headache. A useful description of migraine is a
benign and recurring syndrome of headache associated with other symptoms of
neurologic dysfunction in varying admixtures. Migraine can often be recognized byits activators, referred to as triggers.
Causes, risk factors and pathophysiology
Although many of the causes of migraines are not well understood, both genetic
and environmental factors appear to play a role. Many people with migraines have
a family history of migraines. If one or both parents have migraines, chances arethey will.
Whatever the mechanism of migraine, some of the following can trigger the migraine:
Hormonal changes in women: fluctuations in estrogen seem to cause headaches in
women known as migraines. Women with a history of migraines often get headaches
just before or during their periods, when they have high levels of estrogen. Others
tend to develop increased migraines during pregnancy or menopause. Hormonal
medications, such as birth control pills and hormone replacement therapy, can alsoworsen migraines, although some women find it beneficial.
Food: some migraines are triggered by certain foods. Common include wine, beer
and wine, cheese, chocolate; aspartame, overuse of caffeine, and processed foods.
Skipping meals or fasting can also trigger migraines. Stress at work or at home cantrigger migraines.
Feeling of stimulation: bright lights and the sun can trigger migraines, as can loud
sounds. Unusual odors including pleasant scents, such as perfume, and unpleasant
odors, such as paint and cigarette smoke, can also trigger migraines. Change
the sleep-wake cycle (either lack of sleep or too much sleep) can be a trigger formigraine attacks in some people.
Physical exertion, change the environment (changes in weather or barometricpressure) or medicines can trigger migraines or make migraines very worse.
Migraines can be caused by changes in the trigeminal nerve. An imbalance in brain
chemicals, including serotonin, may also be involved. Serotonin levels decrease
during migraines. This can trigger the trigeminal nervous system to release
substances called neuropeptides, which travel to the outer covering of the brain(meninges). The result is a headache.
The sensory sensitivity that is characteristic of migraine is probably due to
dysfunction of monoaminergic sensory control systems located in the brainstemand thalamus.
There is involvement of the neurotransmitter serotonin in migraine. The introduction
of serotonine agonist, methysergide was found as the first drug capable of preventingmigraine attacks.
Data also support a role for dopamine in the pathophysiology of certain subtypes
of migraine. Most migraine symptoms can be induced by dopaminergic stimulation.
Moreover, there is dopamine receptor hypersensitivity in migraineurs, as
demonstrated by the induction of yawning, nausea, vomiting, hypotension, and
other symptoms of a migraine attack by dopaminergic agonists at doses that do
not affect nonmigraineurs. Dopamine receptor antagonists are effective therapeutic
agents in migraine, especially when given parenterally or concurrently with otherantimigraine agents.
Migraine genes identified by studying families with familial hemiplegic migraine
(FHM) reveal involvement of ion channels (Ca++, Na+, K+) suggesting thatalterations in membrane excitability can predispose to migraine.
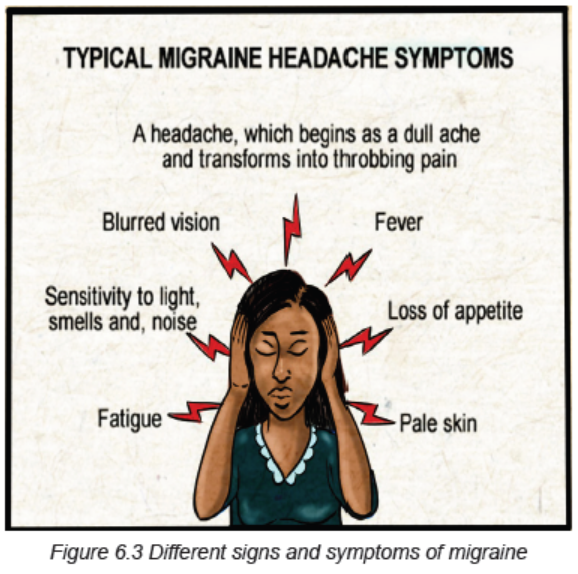
Signs and symptoms of Migraine
A typical migraine attack causes some or all of the following signs and
symptoms: moderate to severe headache, which may be limited to one side of
the head or may affect both sides, fluctuating headache, pain that gets worse
with physical activity, pain interferes with regular activities, nausea with or without
vomiting, sensitive to light (photophobia) and sound, lightheadedness, scalp
tenderness, visual disturbances (Photopsia), paresthesias, vertigo, alteration of
consciousness (syncope, seizures, confusional state) and sometimes diarrhea.
When left untreated, migraines typically last four to 72 hours, but how oftenheadaches occur vary from person to person.
Not all migraines are the same. Most people experience migraines without warning
signs. Some people have migraines with warning signs, formerly known as classic
migraines. The prodromal warning may include vision changes, such as seeingflashing lights or pins and needles feeling in the arms or legs.
Stages of a migraine headache:
1. Prodrome: one or two days before a migraine, person might notice subtle
changes that warn of an upcoming migraine, including constipation, mood
changes from depression to euphoria, food cravings, neck stiffness, increased
thirst and urination or frequent yawning.
2. Aura: For some people, aura might occur before or during migraines. Auras are
reversible symptoms of the nervous system. They’re usually visual, but they
also can include other disturbances. Each symptom usually begins gradually,
builds up over several minutes and lasts 20 minutes to one hour. Examples of
auras include visual phenomena (such as seeing various shapes, bright spots or
flashes of light, etc), vision loss, pins-and-needles sensations in an arm or leg,
weakness or numbness in the face, or one side of the body, difficulty speaking,
hearing noises or music, and Uncontrollable jerking or other movements.
3. Attack: A migraine usually lasts from four to 72 hours if untreated, and the
frequency varies by the person. Migraines might occur rarely or strike several
times a month. During a migraine, patient might have pain (usually on one side
of the head, but often on both sides), pain that throbs or pulses, sensitivity to
light, sound, and sometimes smell and touch, nausea and vomiting.
4. Post-drome/recovery: after a migraine attack, patient might feel drained,
confused and washed out for up to a day. Some people report feeling elated.Sudden head movement might bring on pain again briefly.
Investigations
Diagnosis and confirmation of migraine starts from using the simplified diagnostic
criteria for Migraine (from Headache Classification Committee of the International
Headache Society):
• Repeated attacks of headache lasting 4–72 h in patients with a normal
physical examination, no other reasonable cause for the headache, and:
• At least 2 of the following features: Unilateral pain, Throbbing pain, Aggravation
by movement, Moderate or severe intensity.
• Plus at least 1 of the following features: Nausea/vomiting, Photophobia and
phonophobia
The migraine aura, consisting of visual disturbances with flashing lights or zigzag
lines moving across the visual field or of other neurologic symptoms, is reported in
only 20–25% of patients.
If migraines are typical or there is a family history of migraines, the doctor is likely
to diagnose the underlying problem based on the medical history and examination.
However, if the headache is unusual, severe, or unexpected, the doctor mayrecommend a series of tests to rule out other possible causes:
Computed tomography (CT): this helps the doctor diagnose tumors, infections, and
possibly other medical problems that can cause headaches.
Magnetic resonance imaging (MRI): using powerful radio waves, an MRI creates
a very detailed cross-section of the brain. MRI helps diagnose tumors, strokes,
aneurysms, neurological diseases, and other brain abnormalities. An MRI can also
be used to examine the blood vessels that supply the brain.
Lumbar puncture: if the doctor suspects an underlying problem, such as meningitis
and the cerebrospinal fluid that surrounds the brain and spinal cord, a lumbar
puncture may be ordered. During this procedure, a fine needle is inserted between
two vertebrae in the lower back to extract a sample of cerebrospinal fluid (CSF) for
laboratory investigations.EEG (electroencephalogram) might also be helpful.
Plan of treatment
Choosing a strategy for migraine management depends on the frequency and
severity of headaches, the extent of the disability causing the headache, and themedical problem. Treatment of migraine might focus on:
A. Analgesics
For best results, use a pain reliever as soon as you experience signs or symptomsof a migraine.
Non-steroidal anti-inflammatory drugs (NSAIDs): these medications, such
as ibuprofen, paracetamol or aspirin, can help relieve mild migraines. Medicines
marketed specifically for migraines, such as a combination of acetaminophen,
aspirin, and caffeine may also be helpful for moderate migraines but alone are
ineffective for severe migraine. If taken too often or for a long time, NSAIDs canlead to ulcers, gastrointestinal bleeding, and rebound headaches.
Triptans: for many people with severe migraine attacks, triptans are the drug of
choice. They are effective in reducing pain, nausea, and sensitivity to light and
sound associated with migraines. Medications include sumatriptan (Imitrex),
rizatriptan (Maxalt), naratriptan (Amerge), zolmitriptan (Zomig), almotriptan (Axert),
frovatriptan (Frova), and eletriptan (Relpax). Side effects of triptans include nausea,
dizziness, and muscle weakness. These medications are not recommended forpeople at risk of stroke and heart attack.
Serotonin agonists (Ergot): Ergotamine (Migergot, Cafergot) is less expensive,
but also less effective than triptans. It seems to be most effective for people with
pain that lasts more than 48 hours. Dihydroergotamine (Migranal) is a more effectiveergot derivative with fewer side effects than ergotamine.
Anti-nausea medication: because migraine attacks are often accompanied by
nausea with or without vomiting, the use of anti-nausea medications is appropriate
and is often combined with other medications. Frequently prescribed medications
are dopamine antagonists like metoclopramide (oral) or chlorpromazine (oral orsuppository).
Butalbital combination: drugs that combine the sedative butalbital with aspirin or
acetaminophen (Butapap, Phrenlin Forte) are sometimes used to treat migraine
attacks. Some combinations also include coffee or codeine (Esgic-Plus, Fioricet).
However, these drugs carry a high risk of headache symptoms returning whenstopped.
Narcotic drugs: especially codeine, are sometimes used to treat migraines when
triptans or ergot cannot be taken. Drugs form a habit and are often used only as alast resort.
B. Other medications that may be helpful in management of migraine:
Antidepressants: some antidepressants help prevent certain types of headaches,
including migraines. The most effective are tricyclic antidepressants, such as
amitriptyline, nortriptyline (Pamelor), and protriptyline (Vivactil). These medications
are considered first-line and can relieve migraines by affecting levels of serotonin
and other brain chemicals. Other types of antidepressants, called selective serotonin
reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors(SNRIs), have not been shown to be effective for prevention. migraine headache.
Antiepileptic drugs: some antiepileptic drugs, such as Divalproex (Depakote) and
topiramate (Topamax), and gabapentin (Neurontin), seem to reduce the frequency
of migraines. However, at high doses, antiepileptic drugs can cause side effectssuch as nausea and vomiting, diarrhea, abdominal pain, hair loss, and dizziness.
C. Lifestyle and remedy
Self-care measures can help relieve migraine pain:
Try muscle relaxation exercises: muscle relaxation, relaxation meditation, and yoga
do not require any equipment. They can be learned in the classroom or at home
using books or tapes. Or spend at least half an hour a day doing something relaxing- gardening, music, taking a hot bath or reading a book.
Get enough sleep but don’t oversleep: middle-aged adults need six to eight hoursof sleep a night. It is best to go to bed and wake up at the same time.
Rest and relax: if possible, rest in a quiet room in the dark when you feel a headache
coming on. Place an ice pack wrapped in a cloth on the back of the neck and applygentle pressure to the painful areas of the scalp.
Biofeedback: biofeedback seems to be particularly effective at reducing migraines.
This technique uses special relaxation equipment to teach how to monitor andcontrol certain responses related to stress, such as muscle tension.
Massage: massage can help reduce the frequency of migraines. And it can improvesleep quality, which can help prevent migraines.
Herbs, vitamins, and minerals: there is some evidence that herbs can prevent or
reduce migraine severity. High doses of riboflavin (vitamin B-2) may also preventmigraines by correcting small deficiencies in brain cells.
Lifestyle changes can help reduce the number and severity of migraines. One or
more of these suggestions may be helpful: to avoid triggers, exercise regularly,reduces the effects of estrogen.
Evolution and Complications
Migraine headaches are common and among the most disabling nonfatal conditions
of humankind. They are frequently misdiagnosed which can lead to under treatment.
Patients might also often self-diagnose and self-medicate resulting to inadequate
treatment. With adequate treatment, a patient’s condition and quality of life may
improve considerably. Patient education is extremely important to help patients
identify appropriate self-care measures such as identification of triggering events
and coping with chronic nature of their conditions. Treating health problems thatcause headaches, such as high blood pressure, can eliminate head pain.
If poorly managed, severe headache or migraine can lead to Status Migrainosus (a
relentless attack that lasts for more than 3 days, it can leave you feeling drained or
even disabled), Migrainous Infarction/stroke, where the blood vessel from brain get
narrowed and cut off the oxygen supply, Persistent Aura Without Infarction(patient
can have aura and symptoms like trouble breathing and numbness for months
or even years, the signs seem close to bleeding in the brain but without actualbleeding), Migraine-Triggered Seizure ( this is rare and look like epileptic seizure).
Migraines can also lead to other very serious health issues like depression and
anxiety, vertigo, sleeplessness/insomnia, nausea and vomiting, serotonin
syndrome (use of combined triptans and antidepressants can cause the
serotonin levels which can cause agitation, confusion, diarrhea, twitchy
muscles), stomach problems, rebound headache, etc. Migraines are
associated with a small increased risk of ischaemic strokes, and a very small
increased risk of mental health problems (depression, bipolar disorders,anxiety disorders, panic disorders, etc).
Self-assessment 6.1 and 6.2
1. Basing on signs and symptoms, differentiate different types of headache.
2. What are different risk factors of migraine?
3. What are the signs and symptoms of migraine?
4. What are different treatment options of migraine?
5. List 5 complications of migraine.
6.3 EPILEPSY
Learning Activity 6.3
Carefully read the clinical case scenario below and answer the followingquestions:
A 27 year-old woman was brought by her husband at the district hospital with
seizures. During the history taking, they revealed that patient had episode of
seizures even before and sometimes felt down. They also reported that at the
age of 20 she was experiencing multiple daily episodes of seizures and leftsided
face, arm and leg twitching with loss of consciousness and had multiple
hospitalizations. She has been receiving carbamazepine/tegretol 200mg BID for
the past 7 years but without improvement. She graduated from high school and
worked as a teacher in nearby primary school but was forced to quit due to herseizures.
At the hospital admission, the vital signs were BP of 124/65 mmHg, pulse rate
of 112 beats/ min, temperature of 36.7 degree Celsius, oxygen saturation of
96% on room air and was having hyper-salivation. The neurological examination
showed episodes of left facial twitching every 5 minutes. Her memory, orientation
to place, person and time were impaired. The patient was admitted in secured
room where she was alone and the care giver was instructed to be near the
patient and always turn the head to left and right side. She was placed on
injectable anti-epileptic drugs (phenobarbital inj 600mg to be given into 500ml
of NS 0.9%) to control her seizures, and was also given IV fluids (normal saline
1.5liters per 24 hours) for maintenance. The admitting doctor also ordered the
FBC, electrolytes, EEG and also brain CT scan.
1. Basing on case above, what are the abnormal signs and symptoms was
the patient presenting?
2. What do you think was the medical diagnosis that she had?3. What are the investigations requested to investigate that medical diagnosis?
4. What was included into her plan of management?
5. What do you think can happen to that woman if the condition was not wellmanaged or not responding to treatment?
Epilepsy is a central nervous system (neurological) disorder in which brain
activity becomes abnormal, and is a chronic non-communicable disease of the
brain characterized by recurrent seizures, which are brief episodes of involuntary
movement that may involve a part of the body (partial) or the entire body (generalized)
and are sometimes accompanied by loss of consciousness and control of bowel or
bladder function.
Seizure episodes are a result of excessive electrical discharges in a group of brain
cells. Different parts of the brain can be the site of such discharges. Seizures can
vary from the briefest lapses of attention or muscle jerks to severe and prolonged
convulsions. Seizures can also vary in frequency, from less than one per year
to several per day. One seizure does not signify epilepsy (up to 10% of people
worldwide have one seizure during their lifetime). Epilepsy is defined as having two
or more unprovoked seizures.
Seizures are sudden, explosive, disorderly discharge of cerebral neurons and are
characterized by a sudden, transient alteration in brain function, usually involving
motor, sensory and autonomic or psychic clinical manifestations and altered level
of arousal (awareness). There is a brief disruption in the brain electrical functions.
Convulsion, a term sometimes applied to seizures, refers to the jerky, contract-relax(tonic-clonic) movement associated with some seizures.
Causes, risk factors and pathophysiology
Epilepsy is not contagious. Although many underlying disease mechanisms can
lead to epilepsy, the cause of the disease is still unknown in about 50% of cases
globally. The causes of epilepsy are divided into the following categories: structural,
genetic, infectious, metabolic, immune and unknown. Examples include brain
damage from prenatal or perinatal causes (loss of oxygen or trauma during birth,
low birth weight, infection to the mother, poor nutrition, etc), congenital abnormalities
or genetic conditions with associated brain malformations or abnormalities (brain
tumors or vascular malformations such as arteriovenous malformations (AVMs)
and cavernous malformations, etc), a severe head injury, a stroke that restricts
the amount of oxygen to the brain, an infection of the brain (meningitis, viral
encephalitis or neurocysticercosis, some parasitic infections, etc), certain genetic
syndromes or some developmental disorders (like autism, dementia in older
adults), biochemical disorders (metabolic defects like hypoglycemia, hypocalcemia,drugs and alcohol abuse, etc) and a brain tumor.
There are two phenomenon in the pathophysiology of a seizure:
Hyper-excitability of a neuron: neuronal messages are transmitted by electrical
impulses called the Action Potential. This is actually a net positive inward ion flux
that leads to depolarization or voltage change in the neuronal membrane. The ions
involved include sodium, potassium, calcium and chloride. Normally brain tissues
prevent hyper excitability by several inhibitory mechanisms involving negative ions
like chloride ions. Disturbance in this normal excitability leads to hyper-excitability.
In this state there is increases excitatory transmission of impulses and decreases
inhibitory transmission. In addition there is alteration in the voltage gated ionic
channels. These ion channels normally open when the voltage difference across
the neuronal membrane is changed favorably. Once activated the impulses flow via
the neuronal circuits along the axons of the nerves. An action potential travels down
the axon to the terminal buttons and then releases neurotransmitters in the synapticcleft. This carries the action potential from one nerve to another.
Hyper synchronization: means that a hyper-excitable neuron leads to excessive
excitability of a large group of surrounding neurons. This means that when a large
electrical impulse is generated in one part of the brain from a focus of tissuesmillions of neurons in the brain fire excessively in addition bringing on a seizure.
In summary, the seizures develop into these mechanisms: excitation of a group
of nerves. This is caused by inward currents of Na, Ca and involvement of
excitatory neurotransmitters like Glutamate and Aspartate, too little inhibition, and
epileptogenesis (process whereby a previously normal brain is functionally altered
and biased towards the generation of the abnormal paroxysmal electrical activity
that defines chronic seizures) and hyperexcitability and hypersynchronization
of neurons that facilitates spread. There has to be abnormal synchronization which
is a property of a population of neurons to discharge together independently. Alone,a hyperexcitable neuron cannot generate a seizure.
Signs and symptoms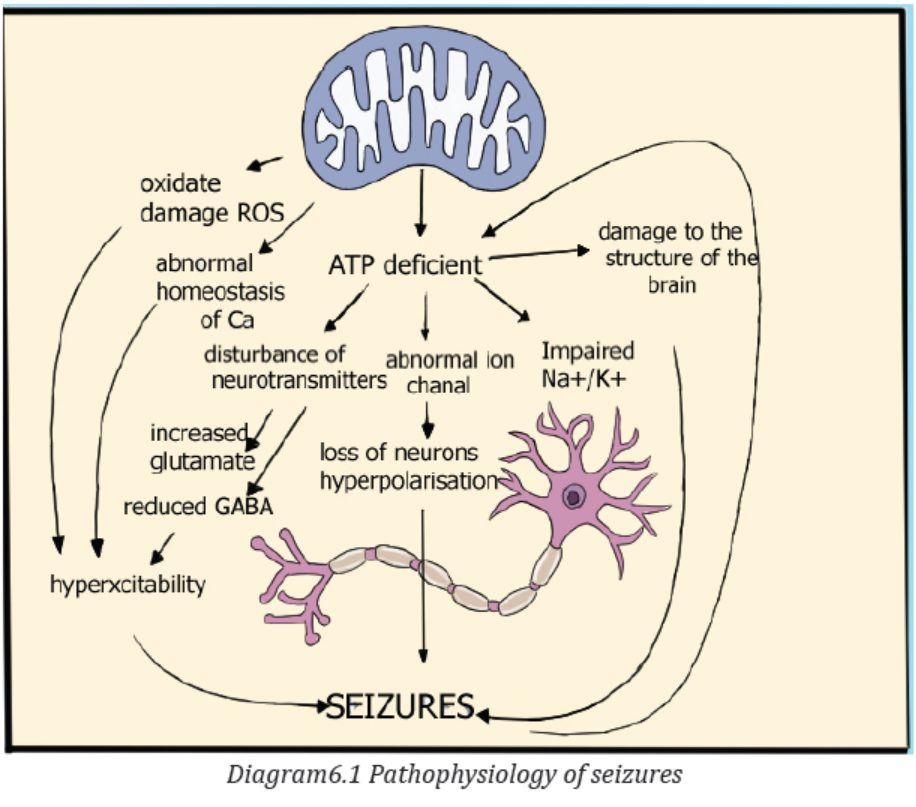
Because epilepsy is caused by abnormal activity in the brain, characteristics of
seizures vary and depend on where in the brain the disturbance first starts, and
how far it spreads. Temporary symptoms occur, such as loss of awareness or
consciousness, and disturbances of movement, sensation (including vision, hearing
and taste), mood, or other cognitive functions, temporary confusion, a staring spell,
stiff muscles, uncontrollable jerking movements of the arms and legs, psychologicalsymptoms such as fear, anxiety or déjà vu.
Signs and symptoms vary depending on the type of epilepsy/seizure. The seizures
are classified as either focal or generalized, based on how and where the abnormalbrain activity begins:
A. Partial/Focal seizures: when seizures appear to result from abnormal activity
in just one area of your brain, they’re called focal seizures. These seizures fallinto two categories:
• Focal seizures without loss of consciousness: also called simple partial
seizures, these seizures don›t cause a loss of consciousness. They may alter
emotions or change the way things look, smell, feel, taste or sound. Some
people experience deja vu. This type of seizure may also result in involuntary
jerking of one body part, such as an arm or leg, and spontaneous sensory
symptoms such as tingling, dizziness and flashing lights.
• Focal seizures with impaired awareness: also called complex partial
seizures, these seizures involve a change or loss of consciousness or
awareness. This type of seizure may seem like being in a dream. During a
focal seizure with impaired awareness, the patient may stare into space and
not respond normally to the environment or perform repetitive movements,
such as hand rubbing, chewing, swallowing or walking in circles. An important
additional subgroup comprises those seizures that begin as partial seizures
and then spread diffusely throughout the cortex, i.e., partial seizures withsecondary generalization.
Signs and symptoms of partial/focal seizures may be confused with other
neurological disorders, such as migraine, narcolepsy or mental illness. A thoroughexamination and testing are needed to distinguish epilepsy from other disorders.
B. Generalized seizures: these are the seizures that appear to involve all
areas of the brain are called generalized seizures. Six types of generalizedseizures exist:
• Absence seizures: absence seizures, previously known as petit mal seizures,
typically occur in children. They’re characterized by staring into space with or
without subtle body movements such as eye blinking or lip smacking and only
last between 5-10 seconds. These seizures may occur in clusters, happening
as often as 100 times per day, and cause a brief loss of awareness.
• Tonic seizures: tonic seizures cause stiff muscles and may affect
consciousness. These seizures usually affect muscles in your back, arms
and legs and may cause you to fall to the ground.
• Atonic seizures: atonic seizures, also known as drop seizures, cause a loss
of muscle control. Since this most often affects the legs, it often causes you
to suddenly collapse or fall down.
• Clonic seizures: clonic seizures are associated with repeated or rhythmic,
jerking muscle movements. These seizures usually affect the neck, face and
arms.
• Myoclonic seizures: myoclonic seizures usually appear as sudden brief
jerks or twitches and usually affect the upper body, arms and legs.
• Tonic-clonic seizures: tonic-clonic seizures, previously known as grand mal
seizures, are the most dramatic type of epileptic seizure. They can cause anabrupt loss of consciousness and body stiffening, twitching and shaking. They
sometimes cause loss of bladder control or biting your tongue. The tonic
clonic seizures develop into these different stages: prodromal (early clinical
manifestations such as malaise, headache, or a sense of depression, that
may occur hours to a few days before the onset of a seizure), aura (peculiar
sensation that immediately precedes the onset of generalized seizure and
may take the form of gustatory, visual or auditory experience or a feeling
of dizziness, numbness), tonic phase (tonic contraction of the muscles of
expiration and the larynx at the onset will produce a loud moan or “ictal cry”.
Respirations are impaired, secretions pool in the oropharynx, and cyanosis
develops. Contraction of the jaw muscles may cause biting of the tongue. A
marked enhancement of sympathetic tone leads to increases in heart rate,
blood pressure, and pupillary size. The duration of this phase ranges between
10 and 20 s. This is associated with loss of consciousness), clonic phase
(after 10-20 s, the tonic phase of the seizure typically evolves into the clonic
phase with alternation of contraction and relaxation of muscles. This phase
lasts no more than 1 min), the postictal (relaxation) phase (the time period
immediately following the cessation of seizure activity. It is characterized by
muscle relaxation (muscular flaccidity), and excessive salivation that can
cause stridorous breathing and partial airway obstruction). Bladder or bowel
incontinence may occur at this point. Patients gradually regain consciousness
over minutes to hours, and during this transition there is typically a period
of postictal confusion. Patients subsequently complain of headache, fatigue,and muscle ache that can last for many hours.
Investigations
To diagnose the epilepsy, there is need to review all the signs and symptoms andensure complete history taking and complete physical exam.
Several tests are used to diagnose epilepsy and determine the cause of the seizures:
A neurological exam: there is need of testing the behavior, motor abilities, mental
function and other areas to diagnose the condition and determine the type of
epilepsy the patients has. This exam included an assessment of motor skills (tested
by having the patient push and pull against the healthcare provider’s hands with his
or her arms and legs. The patient’s joints may also be checked simply by passive
and active movement) and sensory skills (the patient’s healthcare provider mayalso do a sensory test that checks his or her ability to feel.
This may be done by using different instruments: dull needles, tuning forks, alcohol
swabs, or other objects. The healthcare provider may touch the patient’s legs, arms,
or other parts of the body and have him or her identify the sensation (for example,
hot or cold, sharp or dull), balance and coordination (the patient may be asked to
walk normally or on a line on the floor. The patient may be instructed to tap his or herfingers or foot quickly or touch something, such as his or her nose with eyes closed.
Balance may be checked by assessing how the person stands and walks or having
the patient stand with his or her eyes closed while being gently pushed to one side
or the other), mental status (the patient’s level of awareness and interaction with
the environment may be assessed by conversing with the patient and establishinghis or her awareness of person, place, and time.
The person will also be observed for clear speech and making sense while talking.
This is usually done by the patient’s healthcare provider just by observing the
patient during normal interactions), reflexes (these are usually examined with the
use of a reflex hammer. The reflex hammer is used at different points on the body
to test numerous reflexes, which are noted by the movement that the hammer
causes), and functioning of the nerves (there are 12 main nerves of the brain, called
the cranial nerves. During a complete neurological exam, most of these nerves are
evaluated to help determine the functioning of the brain: Cranial nerve I (olfactory
nerve) is the nerve of smell, the patient may be asked to identify different smells
with his or her eyes closed. Cranial nerve II (optic nerve) this nerve carries visionto the brain.
A visual test may be given and the patient’s eye may be examined with a special
light. Cranial nerve III (oculomotor) is responsible for pupil size and certain
movements of the eye. The patient’s healthcare provider may examine the pupil
(the black part of the eye) with a light and have the patient follow the light in various
directions. Cranial nerve IV (trochlear nerve) helps with the movement of the eyes.
Cranial nerve V (trigeminal nerve) allows for many functions, including the ability
to feel the face, inside the mouth, and move the muscles involved with chewing.
The patient’s healthcare provider may touch the face at different areas and watch
the patient as he or she bites down. Cranial nerve VI (abducens nerve) helps with
the movement of the eyes. The patient may be asked to follow a light or finger to
move the eyes. Cranial nerve VII (facial nerve) is responsible for various functions,
including the movement of the face muscle and taste. The patient may be asked
to identify different tastes (sweet, sour, bitter), asked to smile, move the cheeks,
or show the teeth. Cranial nerve VIII (acoustic nerve) is the nerve of hearing. A
hearing test may be performed on the patient. Cranial nerve IX (glossopharyngeal
nerve) is involved with taste and swallowing. Once again, the patient may be asked
to identify different tastes on the back of the tongue. The gag reflex may be tested.
Cranial nerve X (vagus nerve) is mainly responsible for the ability to swallow, thegag reflex, some taste, and part of speech.
The patient may be asked to swallow and a tongue blade may be used to elicit the
gag response. Cranial nerve XI (accessory nerve) is involved in the movement of
the shoulders and neck. The patient may be asked to turn his or her head from
side to side against mild resistance, or to shrug the shoulders. Cranial nerve XII(hypoglossal nerve) is mainly responsible for movement of the tongue. The patient
may be instructed to stick out his or her tongue and speak). The extent of the
exam depends on many factors, including the initial problem that the patient isexperiencing, the age of the patient, and the condition of the patient.
Blood tests (FBC, renal and liver function tests, hormones dosages, lumbar
puncture to get CSF, ionograms, blood glucose, cultures, etc): helpful to check
for signs of infections, genetic conditions or other conditions that may be associatedwith seizures.
Electroencephalogram (EEG): this is the most common test used to diagnose
epilepsy. In this test, electrodes are attached to your scalp with a paste-like
substance or cap. The electrodes record the electrical activity of your brain. If the
patient has epilepsy, it’s common to have changes in your normal pattern of brain
waves, even when there is no seizure. The performer may monitor on video when
conducting an EEG while patient is awake or asleep, to record any seizures he/she
experiences. Recording the seizures may help to determine what kind of seizures
or rule out other conditions. The patient is given instructions to do something thatwill cause seizures, such as getting little sleep prior to the test, etc.
High-density EEG: in a variation of an EEG test, there may recommend highdensity
EEG, which spaces electrodes more closely than conventional EEG about
a half a centimeter apart. High-density EEG may help more precisely determinewhich areas of the brain are affected by seizures.
Computerized tomography (CT) scan: a CT scan uses X-rays to obtain crosssectional
images of the brain. CT scans can reveal abnormalities in the structure of
the brain that might be causing seizures, such as tumors, bleeding and cysts.
Magnetic resonance imaging (MRI): an MRI uses powerful magnets and radio
waves to create a detailed view of the brain. It is helpful to detect lesions or
abnormalities in the brain that could be causing seizures.
Functional MRI (fMRI): A functional MRI measures the changes in blood flow that
occur when specific parts of the brain are working. A fMRI is used before surgery to
identify the exact locations of critical functions, such as speech and movement, so
that surgeons can avoid injuring those places while operating.
Positron emission tomography (PET) Scans: PET scans use a small amount of
low-dose radioactive material that’s injected into a vein to help visualize metabolic
activity of the brain and detect abnormalities. Areas of the brain with low metabolism
may indicate where seizures occur.
Single-photon emission computerized tomography (SPECT): this type of test
is used primarily if an MRI and EEG that didn’t pinpoint the location in brain wherethe seizures are originating.
Neuropsychological tests: in these tests, doctors assess the thinking, memory
and speech skills. The test results help doctors determine which areas of the brain
are affected.
Plan of treatment
The treatment of epilepsy always starts from taking anti-epileptics medications,
and if these medications don’t treat the condition, there can be surgery or another
type of treatment. For better management of epilepsy, there is first need to treat the
cause if identified and provision of antiepileptic drugs.
A. Medications
Most people with epilepsy can become seizure-free by taking one anti-seizure
medication, which is also called anti-epileptic medication. Others may be able to
decrease the frequency and intensity of their seizures by taking a combination of
medications. The prescription starts from a single medication at a relatively low
dosage and may increase the dosage gradually until the seizures are well controlled.
At least half the people newly diagnosed with epilepsy will become seizure-freewhen properly taking first medication.
Monitoring of the patient and health education are keys because these medications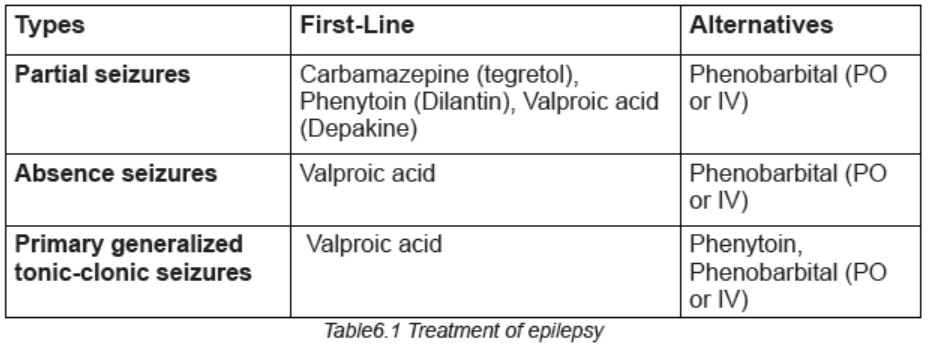
may have some side effects like fatigue, dizziness, weight gain, loss of bone density,skin rashes, loss of coordination, speech problems, memory and thinking problems.
B. Epilepsy surgery
When medications fail to provide adequate control over seizures, surgery may be
an option. With epilepsy surgery, a surgeon removes the area of the brain that is
causing seizures. Surgery is always performed when the tests show that seizures
originate in a small, well-defined area of the brain, the area in the brain to be
operated on doesn’t interfere with vital functions such as speech, language, motorfunction, vision or hearing.
For some types of epilepsy, minimally invasive approaches such as MRI-guided
stereotactic laser ablation may provide effective treatment when an open procedure
may be too risky. In these procedures, the surgeon direct a thermal laser probe at
the specific area in the brain causing seizures to destroy that tissue in an effort tobetter control the seizures.
C. Other therapies
Apart from medications and surgery, these potential therapies offer an alternativefor treating epilepsy:
Vagus nerve stimulation: in vagus nerve stimulation, a device called a vagus
nerve stimulator is implanted underneath the skin of your chest, similar to a heart
pacemaker. Wires from the stimulator are connected to the vagus nerve in the
neck. The battery-powered device sends bursts of electrical energy through thevagus nerve and to the brain.
Ketogenic diet: some children with epilepsy have been able to reduce their
seizures by following a strict diet that’s high in fats and low in carbohydrates. In this
diet, called a ketogenic diet, the body breaks down fats instead of carbohydrates
for energy. After a few years, some children may be able to stop the ketogenic dietand remain seizure-free.
Deep brain stimulation: in deep brain stimulation, surgeons implant electrodes into
a specific part of the brain, typically the thalamus. The electrodes are connected to
a generator implanted in the chest. The generator regularly sends electrical pulses
to the brain at timed intervals, and may reduce the seizures. Deep brain stimulationis often used for people whose seizures don’t get better with medication.
Responsive neurostimulation: these implantable, pacemaker-like devices can
help significantly reduce how often seizures occur. These responsive stimulation
devices analyze brain activity patterns to detect seizures as they start and deliveran electrical charge or drug to stop the seizure before it causes impairment.
D. Prevention of epilepsy
An estimated 25% of epilepsy cases are preventable through:
– Education (recognition of signs and symptoms of prodroma and aura, so that
the patient may avoid the fall in a very risk area i.e. fire, stairs…)
– Avoid driving, working with machinery, working at heights, swimming and
other activities that may cause serious injuries
– Psychosocial support (Counseling to minimize depression, anxiety due to
social stigmatization, lack of job, frequent hospitalization…)
– Preventing head injury is the most effective way to prevent post-traumaticepilepsy.
– Adequate perinatal care can reduce new cases of epilepsy caused by birth
injury.
– The use of drugs and other methods to lower the body temperature of a
feverish child can reduce the chance of febrile seizures.
– The prevention of epilepsy associated with stroke is focused on cardiovascular
risk factor reduction, e.g. measures to prevent or control high blood pressure,
diabetes and obesity, and the avoidance of tobacco and excessive alcohol
use.
– Central nervous system infections are common causes of epilepsy in tropical
areas, elimination of microorganisms/parasites in the environments and
education on how to avoid infections can be effective ways to reduce epilepsyworldwide.
Adequate medical diagnosis
Epilepsy is a type of neurological disorder known for causing seizures. These
seizures can be sporadic and occur without warning, or they might be chronic and
occur on a regular basis. Majority of epileptic patients require ongoing treatment toprevent seizures from disrupting their daily activities.
Treatment is one of the most important factors that affect the overall epilepsy
prognosis. Anti-seizures medications when taken on a regular basis, can help
control activity in the brain that leads to epileptic seizures. In turn, this helps to
also minimize risk factors and complications related to epilepsy. If not properly
managed, epilepsy leads to very life threatening complications. A great proportion
of the causes of death related to epilepsy are potentially preventable, such as falls,drowning, burns and prolonged seizures.
Evolution and complications
People with epilepsy tend to have more physical problems (such as fractures and
bruising from injuries related to seizures), as well as higher rates of psychological
conditions, including anxiety and depression. Similarly, the risk of premature death
in people with epilepsy is up to three times higher than in the general population.
The other complications related to epilepsy are drowning, car accidents,
pregnancy complications, emotional and psychological health issues problems,
especially depression, anxiety, and suicidal thoughts and behaviors. Other lifethreatening
complications of epilepsy that might occur are:
• Status epilepticus: this condition occurs if a patient is in a state of continuous
seizure activity lasting more than five minutes or if there is frequent recurrent
seizures without regaining full consciousness in between them. People with
status epilepticus have an increased risk of permanent brain damage anddeath.
• Sudden unexpected death in epilepsy (SUDEP): people with epilepsy
also have a small risk of sudden unexpected death. The cause is unknown
but may occur due to heart or respiratory conditions mainly to patients with
frequent tonic-clonic seizures or people whose seizures aren’t controlled ornot responding to medications.
Self-assessment 6.3
1. Differentiate the epilepsy to seizures
2. Basing on signs and symptoms, differentiate two major types of epilepsy
3. What are the mechanisms involved into pathophysiology of epilepsy
4. What are the examples of drugs used to treat different types of seizures?
6.4 END UNIT 6 ASSESSMENT
End unit assessment 6
SECTION A:SHORT ANSWER QUESTIONS
1. What are the elements of neurological diseases assessment?
2. Differentiate the headache to migraine.
3. What are the risk factors to develop the migraine?
4. Describe different treatment options of migraine.
5. Define epilepsy and differentiate epilepsy to seizures and convulsions.
6. Basing on signs and symptoms, differentiate two major types of epilepsy
7. List 5 different complications of epilepsy
8. What are the preventive strategies of epilepsy?
9. Describe the status epilepticus
SECTION B:MULTIPLE CHOICE QUESTIONS
1. Which type of headache is suspected when the headaches are unilateral
and throbbing, preceded by a prodrome of photophobia, and associated
with a family history of this type of headache?
a. Cluster
b. Migraine
c. Frontal-typed. Tension-type
2. A patient is diagnosed with cluster headaches. The nurse knows that
which characteristics are associated with this type of headache?
a. Family history
b. Alcohol is the only dietary trigger
c. Abrupt onset lasting 5 to 180 minutes
d. Severe, sharp, penetrating head pain
e. Bilateral pressure or tightness sensation
f. May be accompanied by unilateral ptosis or lacrimation
3. What is the most important method of diagnosing functional headaches?
a. CT scan
b. Electromyography (EMG)
c. Cerebral blood flow studies
d. Thorough history of the headache
4. The nurse is preparing to admit a newly diagnosed patient experiencing
tonic-clonic seizures. What could the registered nurse delegate to associate
nurse?
a. Complete the admission assessment.
b. Explain the call system to the patient.
c. Obtain the suction equipment from the supply cabinet.
d. Place a padded tongue blade on the wall above the patient’s bed.
5. How do generalized seizures differ from focal seizures?
a. Focal seizures are confined to one side of the brain and remain focal
in nature.
b. Generalized seizures result in loss of consciousness whereas focal
seizures do not.
c. Generalized seizures result in temporary residual deficits during the
postictal phase.
d. Generalized seizures have bilateral synchronous epileptic discharges
affecting the whole brain at onset of the seizure.
6. The patient is diagnosed with complex focal seizures. Which characteristics
are related to complex focal seizures?
a. Formerly known as grand mal seizure
b. Often accompanied by incontinence or tongue or cheek biting
c. Psychomotor seizures with repetitive behaviors and lip smacking
d. Altered memory, sexual sensations, and distortions of visual or auditorysensations
e. Loss of consciousness and stiffening of the body with subsequent
jerking of extremities
f. Often involves behavioral, emotional, and cognitive functions with
altered consciousness
7. Which type of seizure is most likely to cause death for the patient?
a. Subclinical seizures
b. Myoclonic seizures
c. Psychogenic seizures
d. Tonic-clonic status epilepticus
8. A patient admitted to the hospital following a generalized tonic-clonic
seizure asks the nurse what caused the seizure. What is the best response
by the nurse?
a. “So many factors can cause epilepsy that it is impossible to say what
caused your seizure.”
b. “Epilepsy is an inherited disorder. Does anyone else in your family have
a seizure disorder?”
c. “In seizures, some type of trigger causes sudden, abnormal bursts of
electrical brain activity.”
d. “Scar tissue in the brain alters the chemical balance, creating
uncontrolled electrical discharges.”
9. Following a generalized tonic-clonic seizure, the patient is tired and sleepy.
What care should the nurse provide?
a. Suction the patient before allowing him to rest.
b. Allow the patient to sleep as long as he feels sleepy.
c. Stimulate the patient to increase his level of consciousness.
d. Check the patient’s level of consciousness every 15 minutes for an
hour.
10. During the diagnosis and long-term management of a seizure disorder,
what should the nurse recognize as one of the major needs of the patient?
a. Managing the complicated drug regimen of seizure control
b. Coping with the effects of negative social attitudes toward epilepsy
c. Adjusting to the very restricted lifestyle required by a diagnosis of
epilepsy
d. Learning to minimize the effect of the condition in order to obtainemployment
REFERENCES
1. Barbara K. Timby; Nancy E. Smith. (2010). Introductory medical-surgical
nursing 10th Edition.
2. Daniel J Bonthius, Andrew D Hershey. (2022). Headache in children: Approach
to evaluation and general management strategies
3. Deborah J Wexler. (2022). Initial management of hyperglycemia in adults with
type 2 diabetes mellitus.
4. Deborah J Wexler. (2022). Overview of general medical care in nonpregnant
adults with diabetes mellitus
5. Diabetes mellitus, cases management, retrieved from
6. Epilepsy case management, retrieved from https://www.healthline.com/health/
epilepsy
7. Epilepsy case management, retrieved from https://www.mayoclinic.org/
diseases-conditions/epilepsy/symptoms-causes/syc-20350093
8. Epilepsy factsheets, retrieved from https://www.who.int/news-room/fact-sheets/
detail/epilepsy
9. Michael Cutrer. (2022). Pathophysiology, clinical manifestations, and diagnosis
of migraine in adults. Retrieved from https://www.uptodate.com/contents/
pathophysiology-clinical-manifestations-and-diagnosis-of-migraine-in-adul
ts?search=migraine&source=search_result&selectedTitle=2~150&usage_
type=default&display_rank=2
10. John Service, MD, (2000). Diabetes mellitus: Management and complications.
DOI: https://doi.org/10.1016/S0025-6196(12)61411-6
11. Frederick R Taylor. (2022). Tension-type headache in adults: Pathophysiology,
clinical features, and diagnosis. Retrived from https://www.uptodate.
com/contents/tension-type-headache-in-adults-pathophysiologyclinical-
features-and-diagnosis?search=headache&source=search_
result&selectedTitle=5~150&usage_type=default&display_rank=4
12. https://www.mayoclinic.org/diseases-conditions/diabetes/symptoms-causes/
syc-20371444
13. Introductory medical-surgical nursing by Barbara K. Timby and Nancy E. Smith
10th edition
14. Irl B Hirsch, Michael Emmett. (2020). Diabetic ketoacidosis and hyperosmolar
hyperglycemic state in adults: Clinical features, evaluation, and diagnosis
15. Irl B Hirsch, Michael Emmett. (2020). Diabetic ketoacidosis and hyperosmolar
hyperglycemic state in adults: Epidemiology and pathogenesis
16. Irl B Hirsch, Michael Emmett. (2022). Diabetic ketoacidosis and hyperosmolarhyperglycemic state in adults: Treatment
17. Lynne L Levitsky, Madhusmita Misra. (2022).Epidemiology, presentation, and
diagnosis of type 1 diabetes mellitus in children and adolescents
18. R Joshua Wootton, Franz J Wippold II, Mark A Whealy. (2021). Evaluation of
headache in adults.
19. Sharon L. Lewis, Shannon Ruff Dirken, Margaret McLean Heitkemper, L. B.
(2014). Medical-surgical nursing. Assessment and management of clinical
conditions.
20. Silvio E Inzucchi, Beatrice Lupsa. (2022). Clinical presentation, diagnosis, and
initial evaluation of diabetes mellitus in adults. Retrieved from From https://www.
uptodate.com/contents/clinical-presentation-diagnosis-and-initial-evaluationof-
diabetes-mellitus-in-adults?search=diabetes%20mellitus&source=search_
result&selectedTitle=1~150&usage_type=default&display_rank=1
21. Silvio E Inzucchi, Beatrice Lupsa. (2022). Clinical presentation, diagnosis, and
initial evaluation of diabetes mellitus in adults
22. Tina Shih. (2021). Seizures and epilepsy in older adults: Etiology, clinical
presentation, and diagnosis. Retrieved from https://www.uptodate.com/contents/
seizures-and-epilepsy-in-older-adults-etiology-clinical-presentation-and-diag
nosis?search=epilepsy&source=search_result&selectedTitle=9~150&usage_
type=default&display_rank=9
23. Todd J Schwedt, Ivan Garza. (2022). Acute treatment of migraine in adults. Retrived
rom https://www.uptodate.com/contents/acute-treatment-of-migraine-in-adu
lts?search=migraine&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
24. Todd J Schwedt, Ivan Garza. (2022). Preventive treatment of episodic migraine
in adults. Retrieved from https://www.uptodate.com/contents/preventivetreatment-
of-episodic-migraine-in-adults?search=migraine&source=search_
result&selectedTitle=3~150&usage_type=default&display_rank=3
25. Barbara K. Timby; Nancy E. Smith. (2010). Introductory medical-surgical
nursing 10th Edition.
26. CDC. (2021). Stroke. Retrieved from https://www.cdc.gov/stroke/facts.htm,
27. Christopher H Fanta, M. (2021). An overview of asthma management. Retrieved
from https://www.uptodate.com/contents/an-overview-of-asthma-managem
ent?search=asthma&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
28. Frederick E Barr, MD, M., & Barney S Graham, MD, P. (2011). Respiratory
syncytial virus infection: Treatment. Retrieved September 19, 2021, from
Respiratory syncytial virus infection: Treatment website: https://www.
uptodate.com/contents/respiratory-syncytial-virus-infection-treatment?se
arch=bronchiolitis&source=search_result&selectedTitle=8~150&usage_type=default&display_rank=8
29. Jamary Oliveira-Filho, M. T. M. (2021). Initial assessment and management
of acute stroke. Retrieved from https://www.uptodate.com/contents/initialassessment-
and-management-of-acute-stroke?search=stroke&source=sear
ch_result&selectedTitle=1~150&usage_type=default&display_rank=1
30. Jan Basile, M. J. B. (2021). Overview of hypertension in adults. Retrieved
from https://www.uptodate.com/contents/overview-of-hypertension-in-adults
?search=hypertension&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1,
31. Jose-Alberto Palma, H. K. (2021). Mechanisms, causes, and evaluation
of orthostatic hypotension. Retrieved from https://www.uptodate.com/
contents/mechanisms-causes-and-evaluation-of-orthostatic-hypotension?
search=hypotension&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
32. Julio A Ramirez, MD, F. (2021). Overview of community-acquired pneumonia
in adults. Retrieved from https://www.uptodate.com/contents/overview-ofcommunity-
acquired-pneumonia-in-adults?search=pneumonia&source=sear
ch_result&selectedTitle=3~150&usage_type=default&display_rank=3 on 22nd
September 2021
33. Louis R Caplan. (2020). Etiology, classification, and epidemiology of
stroke. Retrieved from https://www.uptodate.com/contents/etiologyclassification-
and-epidemiology-of-stroke?search=stroke&source=search_
result&selectedTitle=3~150&usage_type=default&display_rank=3,
34. Louis R Caplan. (2021). Clinical diagnosis of stroke subtypes. Retrieved
from https://www.uptodate.com/contents/clinical-diagnosis-of-stroke-subty
pes?search=stroke&source=search_result&selectedTitle=5~150&usage_
type=default&display_rank=5,
35. Mayo Clinic. (2021). Low Blood pressure/Hypotension. Retrieved from https://
www.mayoclinic.org/diseases-conditions/low-blood-pressure/symptomscauses/
syc-20355465#:~:text=What’s considered low blood pressure,pressure
is lower than normal.,
36. Michael Klompas, MD, M. (2021). Clinical evaluation and diagnostic testing
for community-acquired pneumonia in adults. Retrieved from https://www.
uptodate.com/contents/clinical-evaluation-and-diagnostic-testing-forcommunity-
acquired-pneumonia-in-adults?search=pneumonia&source=sear
ch_result&selectedTitle=1~150&usage_type=default&display_rank=1
37. Pedro A Piedra, M., & Ann R Stark, M. (2021). Bronchiolitis in infants and children:
Treatment, outcome, and prevention. Retrieved from https://www.uptodate.com/
contents/bronchiolitis-in-infants-and-children-treatment-outcome-and-preventi
on?search=bronchiolitis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 on 23rd September 2021
38. Sharon L. Lewis, Shannon Ruff Dirken, Margaret McLean Heitkemper, L. B.
(2014). Medical-surgical nursing. Assessment and management of clinical
conditions.
39. Sterns, R. H. (2020). Etiology, clinical manifestations, and diagnosis
of volume depletion in adults. Retrieved from https://www.uptodate.
com/contents/etiology-clinical-manifestations-and-diagnosis-of-volumedepletion-
in-adults?search=hypotension in adults&source=search_
result&selectedTitle=5~150&usage_type=default&display_rank=5
40. Talmadge E King, Jr, M. (2021a). Overview of bronchiolar disorders in
adults. Retrieved from https://www.uptodate.com/contents/overview-ofbronchiolar-
disorders-in-adults?search=bronchiolitis&source=search_
result&selectedTitle=3~150&usage_type=default&display_rank=3
41. Talmadge E King, Jr, M. (2021b). Respiratory bronchiolitis-associated interstitial
lung disease. Retrieved from https://www.uptodate.com/contents/respiratorybronchiolitis-
associated-interstitial-lung-disease?search=bronchiolitis&source
=search_result&selectedTitle=4~150&usage_type=default&display_rank=4 on
20th September 2021
42. WHO. (2021a). Hypertension. Retrieved from https://www.who.int/news-room/
fact-sheets/detail/hypertension
43. WHO. (2021b). Stroke/Cerebrovascular accident. Retrieved from http://www.
emro.who.int/health-topics/stroke-cerebrovascular-accident/index.html,
44. William J Barson, M. (2021). Pneumonia in children: Epidemiology, pathogenesis,
and etiology. Retrieved from https://www.uptodate.com/contents/pneumonia-inchildren-
epidemiology-pathogenesis-and-etiology?search=pneumonia&sourc
e=search_result&selectedTitle=10~150&usage_type=default&display_rank=6
on 22nd September 2021
45. Nader Shaikh, M., & Alejandro Hoberman, M. (2021). Urinary tract infections
in infants older than one month and young children: Acute management,
imaging, and prognosis. Retrieved from https://www.uptodate.com/contents/
urinary-tract-infections-in-infants-older-than-one-month-and-young-childrenacute-
management-imaging-and-prognosis?search=UTI&source=search_
result&selectedTitle=2~150&usage_type=default&display_rank=2
46. Thomas M Hooton, M. (2021). Acute simple cystitis in men. Retrieved from https://
www.uptodate.com/contents/acute-simple-cystitis-in-men?search=acute
simple cystitis&source=search_result&selectedTitle=2~150&usage_
type=default&display_rank=2
47. Alain Meyrier, M., & Thomas Fekete, M. (2021). Acute and chronic bacterial
prostatitis. Retrieved from https://www.uptodate.com/contents/acute-bacterialprostatitis?
search=acute and chronic bacterial prostatitis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
48. J Dennis Fortenberry, MD, M. (2021). Sexually transmitted infections:
Issues specific to adolescents. Retrieved from https://www.uptodate.
com/contents/sexually-transmitted-infections-issues-specific-toadolescents?
search=Sexually transmitted infections: Issues specific
to adolescents&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
49. Michel Pontari, M. (2021). Chronic prostatitis and chronic pelvic pain syndrome.
Retrieved from https://www.uptodate.com/contents/chronic-prostatitis-andchronic-
pelvic-pain-syndrome?search=chronic prostatitis&source=search_
result&selectedTitle=1~37&usage_type=default&display_rank=1
50. Thomas M Hooton, M., & Kalpana Gupta, MD, M. (2021). Acute complicated
urinary tract infection (including pyelonephritis) in adults. Retrieved from
https://www.uptodate.com/contents/acute-complicated-urinary-tractinfection-
including-pyelonephritis-in-adults?search=Acute complicated
urinary tract infection (including pyelonephritis) in adults&source=search_
result&selectedTitle=1~150&usage_type=default&display_rank=1
51. Barbara K. Timby; Nancy E. Smith. (2010). Introductory medical-surgical
nursing 10th Edition.
52. Sharon L. Lewis, Shannon Ruff Dirken, Margaret McLean Heitkemper, L. B.
(2014). Medical-surgical nursing. Assessment and management of clinical
conditions.
53. Charles B. Hicks, Meredith Clement. (2021). Syphilis: Epidemiology,
pathophysiology, clinical manifestations, treatment and monitoring.
54. Source: https://www.cdc.gov/std/gonorrhea/stdfact-gonorrhea.htm accessed
on 04th Novemebr,2021
55. Introductory medical-surgical nursing by Barbara K. Timby and Nancy E. Smith
10th edition P.889-892.
56. https://www.mayoclinic.org/diseases-conditions/hpv-infection/symptomscauses/
syc-20351596 accessed on 20th November,2021
57. https://en.wikipedia.org/wiki/Human_papillomavirus_infection#/media/
File:HPV_causing_cervical_cancer.jpg accessed on 19th November,2021
58. https://www.mayoclinic.org/diseases-conditions/chlamydia/diagnosistreatment/
drc-20
59. https://www.karger.com/Article/Abstract/348751
60. https://www.wikidoc.org/index.php/Chlamydia_infection_pathophysiology
61. https://my.clevelandclinic.org/health/diseases/4108-diarrhea visitedon17thOctober,2021.