UNIT 5 MEDICAL PATHOLOGIES OF ENDOCRINE SYSTEM
Key Unit Competences
To take an appropriate decision on management of common pathologies of
Endocrine system.
Introductory activity 5.0
Carefully observe the picture below and answer the following questions:
Figure 5.1 Glycemia measurement
1. How do you call the instrument shown at the picture below?
2. Can you interpret the readings/results from the instrument above?
3. Can you list some conditions that a person might present that will enablethe use of this equipment?
Endocrine glands include the hypothalamus, pituitary, thyroid, parathyroids,
adrenals, pancreas, ovaries, testes, and pineal gland. Exocrine glands are not part
of the endocrine system. They secrete their substances into ducts that then empty
into a body cavity or onto a surface. Hormones are chemical substances produced
in the body that control and regulate the activity of certain target cells or organs.
Many are produced in one part of the body and control and regulate the activity of
certain cells or organs in another part of the body. Endocrine glands produce andsecrete hormones that travel to affect their specific target tissues.
5.1 DIABETES MELLITUS
Learning Activity 5.1
Carefully read this below situation and answer the following questions:
A 54 year old female visited NCD clinic with the complaints of excessive urination,
sudden weight loss, blurred vision, increased thirst, fatigue and excessive
sweating. She was experiencing these conditions from last one month. From the
past medical history, she was also suffering from hypertension from last 3 years
under treatment (Atenolol 50mg OD per day and Lasix 40mg BID per day from
last 3 years. From the general examination, weight: 70kg and height: 152cm
BMI: 30.5kg/m2. She also had limited physical activities as she always stayed
at home.
From all observations, the NCD Medical Doctor recommended to monitor the
patient’s blood glucose level. At that time patient’s random blood glucose level
was 245mg/dl which was beyond the normal range of the random blood glucose
level (70-110mg/dl). The NCD Medical Doctor recommended also to patient
to monitor the patient fasting glucose level and then to check HbA1C Level
after about every 3rd month in the following visits. The NCD Medical Doctor
prescribed the drug (metformin 500mg BID per day) that should be taken about
5 -10 minutes before the meal and in combination with other drugs she has been
taking.
The patient was also advised that instead of eating a lot at 3 meals, divide total
intake in 5 meals. She was also suggested to avoid sugar intake, do exercise
and walk to reduce body weight, take high fiber diet and less intake of fats and
carbohydrates. The patient was given the appointments to visit the NCD clinic
on monthly basis to monitor the trends of blood sugar levels and also the other
symptoms that might arise from existing condition.
1. What are the abnormal signs and symptoms that the patient was presenting?
2. What do you think is the medical condition was she presenting in addition
to hypertension?
3. What are the investigations requested to diagnose that medical condition?
4. What was included into her plan of the management?5. If this condition is not well managed, what are the possible complications?
The pancreas is a long, tapered, lobular, soft gland located behind the stomach and
anterior to the first and second lumbar vertebrae. The pancreas has both exocrine
and endocrine functions. The hormone-secreting portion of the pancreas is referred
to as the islets of Langerhans. The islets account for less than 2% of the gland
and consist of four types of hormone-secreting cells: α, β, delta, and F cells. α
Cells produce and secrete the hormone glucagon. Insulin and amylin are produced
and secreted by β cells. Somatostatin is produced and secreted by the delta cells.
Pancreatic polypeptide (PP) is secreted by the F
(or PP) cells.
Glucagon is synthesized and released from pancreatic α cells and the gut in response
to low levels of blood glucose, protein ingestion, and exercise. Glucagon increases
blood glucose by stimulating glycogenolysis, gluconeogenesis, and ketogenesis.
Glucagon and insulin function in a reciprocal manner to maintain normal blood
glucose levels. In the fasting state, hormones such as catecholamines, cortisol,
and glucagon break down stored complex fuels (catabolism) to provide glucose as
fuel for energy.
Insulin is the principal regulator of metabolism and storage of ingested
carbohydrates, fats, and proteins. Insulin facilitates glucose transport across
cell membranes in most tissues. However, the brain, nerves, lens of the eye,
hepatocytes, erythrocytes, and cells in the intestinal mucosa and kidney tubules
are not dependent on insulin for glucose uptake. An increased blood glucose level
is the major stimulus for insulin synthesis and secretion. Other stimuli to insulin
secretion are increased amino acid levels and vagal stimulation. Insulin secretion is
usually inhibited by low blood glucose levels, glucagon, somatostatin, hypokalemia,
and catecholamines. A major effect of insulin on glucose metabolism occurs in
the liver, where the hormone enhances glucose incorporation into glycogen and
triglycerides by altering enzymatic activity and inhibiting gluconeogenesis. After a
meal, insulin is responsible for the storage of nutrients (anabolism). Another major
effect occurs in peripheral tissues, where insulin facilitates glucose transport into
cells, transport of amino acids across muscle membranes and their synthesis into
protein, and transport of triglycerides into adipose tissue.
The term diabetes mellitus describes diseases of abnormal carbohydrate metabolism
that are characterized by hyperglycemia. It is associated with a relative or absolute
impairment in insulin secretion, along with varying degrees of peripheral resistance
to the action of insulin.
Types of diabetes mellitus and their causes: the underlying cause of diabetesvaries by type:
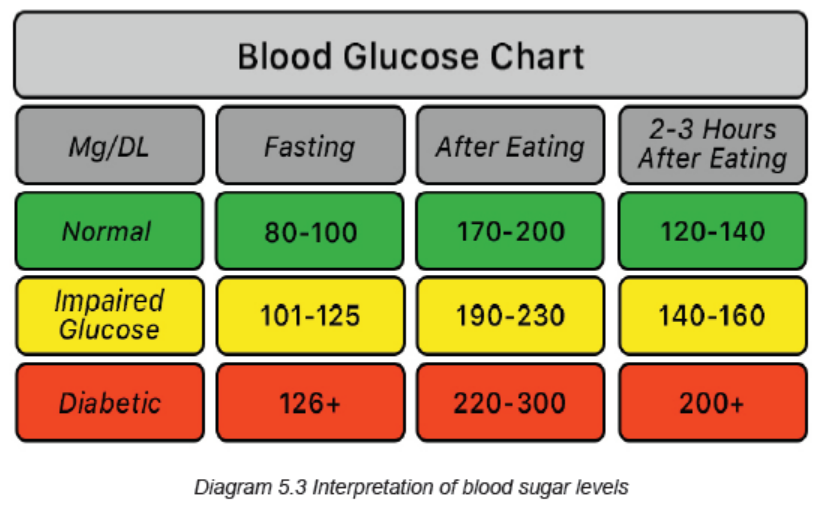
A. Prediabetes:
Prediabetes is a condition in which blood glucose levels are too high to be considered
normal but not high enough to be labeled diabetes. People have prediabetes if their
fasting blood glucose level is between 100 mg/dL (5.6 mmol/L) and 125 mg/dL
(6.9 mmol/L) or if their blood glucose level 2 hours after a glucose tolerance test
is between 140 mg/dL (7.8 mmol/L) and 199 mg/dL (11.0 mmol/L). Prediabetes
carries a higher risk of future diabetes as well as heart disease. Decreasing body
weight by 5 to 10% through diet and exercise can significantly reduce the risk of
developing future diabetes.
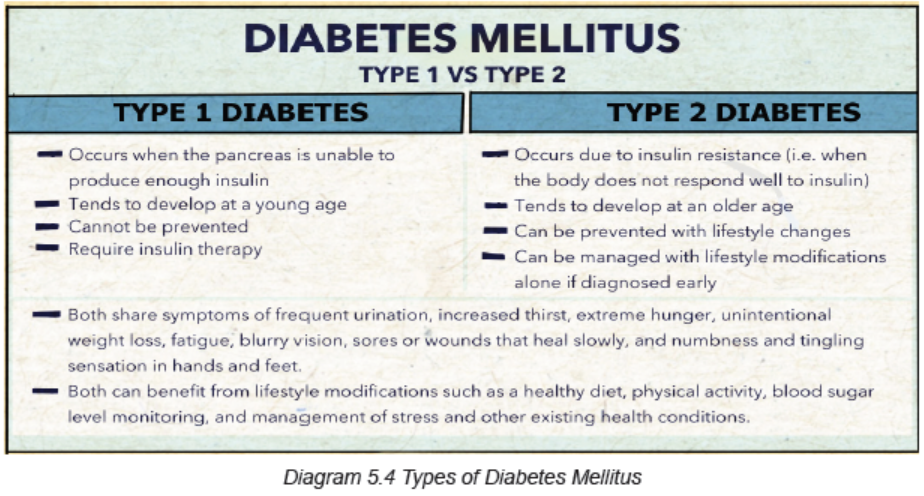
B. Type 1 diabetes mellitus:
In type 1 diabetes mellitus (formerly called insulin-dependent diabetes or
juvenile-onset diabetes), the body’s immune system attacks the insulin-producing
cells of the pancreas, and more than 90% of them are permanently destroyed. The
pancreas, therefore, produces little or no insulin. Most people who have type 1
diabetes develop the disease before age 30, although it can develop later in life.
Some environmental factors like viral infection or nutritional factor during childhood
or early adulthood cause the immune system to destroy the insulin-producing cells
of the pancreas. A genetic predisposition makes some people more susceptible to
an environmental factor.
C. Type 2 diabetes mellitus:
In type 2 diabetes mellitus (formerly called non–insulin-dependent diabetes or
adult-onset diabetes), the pancreas often continues to produce insulin, sometimes
even at higher than normal levels, especially early in the disease. However, the
body develops resistance to the effects of insulin, so there is not enough insulin to
meet the body’s needs. As type 2 diabetes progresses, the insulin producing ability
of the pancreas decreases.
Obesity is the chief risk factor for developing type 2 diabetes, and 80 to
90% of people with this disorder are overweight or obese. Because obesity
causes insulin resistance, obese people need very large amounts of insulin to
maintain normal blood glucose levels.
Certain disorders and drugs can affect the way the body uses insulin and can lead
to type 2 diabetes mellitus.
Examples of common states (conditions) that result in impaired insulin use are
high levels of corticosteroids (most commonly due to use of corticosteroid drugs or
Cushing syndrome (a disorder that occurs when your body makes too much of the
hormone cortisol over a long period of time), Pregnancy. Diabetes also may occur
in people with excess production of growth hormone (acromegaly) and in people
with certain hormone-secreting tumors. Severe or recurring pancreatitis and otherdisorders that directly damage the pancreas can lead to diabetes
D. Gestational diabetes:
Gestational diabetes is diabetes diagnosed for the first time during pregnancy
(gestation). Like other types of diabetes, gestational diabetes affects how your cells
use sugar (glucose). Gestational diabetes causes high blood sugar that can affect
your pregnancy and your baby’s health. For a person who has gestational diabetes
during pregnancy, generally the blood sugar returns to its usual level soon after
delivery. But the person has a higher risk of getting type 2 diabetes mellitus.
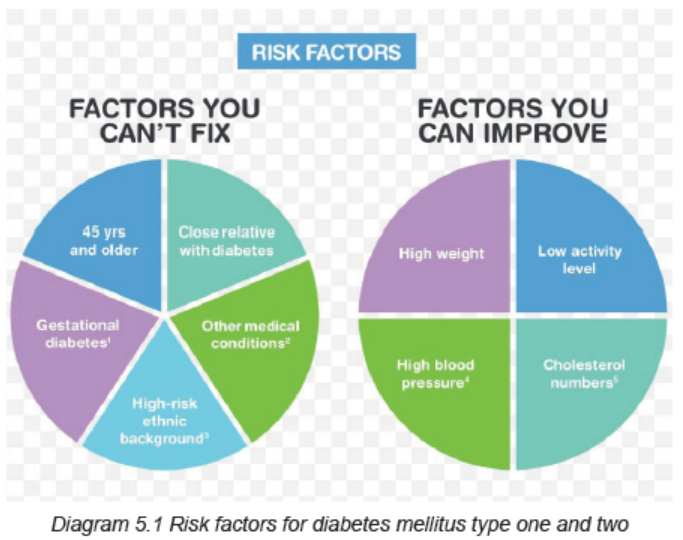
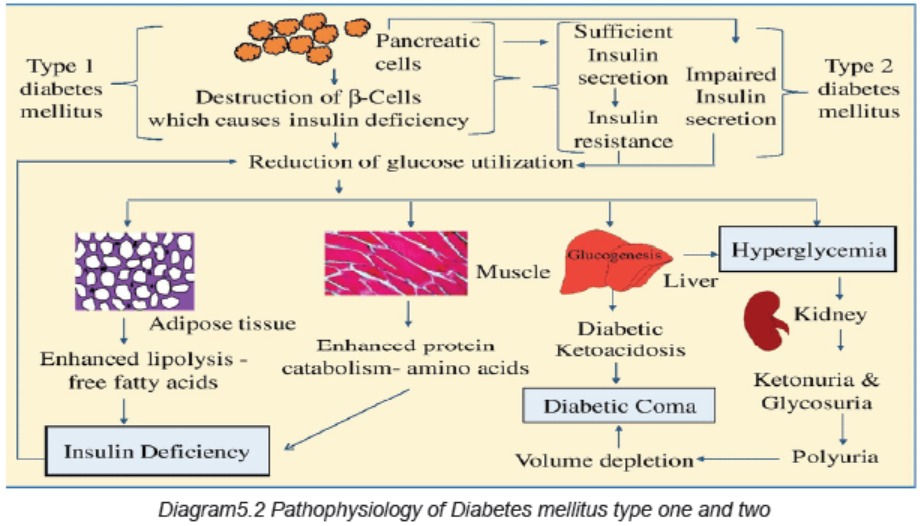
Risk factors and Pathophysiology
The factors that increase the risk of developing diabetes mellitus differ dependingon the type of diabetes.
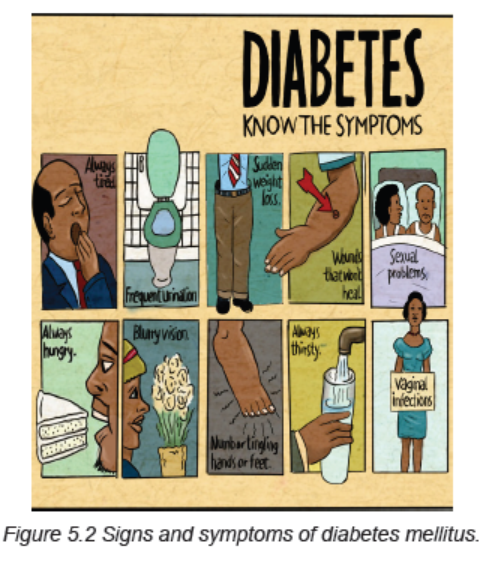
Signs and symptoms:
Diabetes signs and symptoms vary depending on how much the blood sugar iselevated.
Some people, especially those with prediabetes or type 2 diabetes, may sometimes
not experience symptoms. In type 1 diabetes, symptoms tend to come on quickly
and be more severe.
The signs and symptoms of type 1 diabetes and type 2 diabetes are: increased
thirst (polydipsia), frequent urination (polyuria), extreme hunger (polyphagia),
unexplained weight loss, presence of ketones (are a byproduct of the breakdown
of muscle and fat that happens when there’s not enough available insulin) in the
urine, fatigue, irritability, blurred vision, numbness or tingling into the hands or feet,
slow-healing sores, frequent infections such as gums or skin infections and vaginal
infections. Patient with type 1 diabetes might also present nausea, vomiting andstomach pains.
Investigations
Symptomatic hyperglycemia: The diagnosis of diabetes mellitus is easily
established when a patient presents with classic symptoms of hyperglycemia (thirst,
polyuria, weight loss, blurry vision) and has a random blood glucose value of 200
mg/dL (11.1 mmol/L) or higher.
Most patients with type 1 diabetes are symptomatic and have plasma glucose
concentrations/random blood glucose of ≥200 mg/dL. Some patients with type 2
diabetes also present with symptomatic hyperglycemia and blood glucose ≥200
mg/dL.
Asymptomatic hyperglycemia: The diagnosis of diabetes in an asymptomatic
individual (generally type 2 diabetes) can be established with any of the followingcriteria:
• Fasting plasma glucose (FPG) values ≥126 mg/dL (7.0 mmol/L). Fasting is
defined as no caloric intake for at least eight hours.
• Two-hour plasma glucose values of ≥200 mg/dL (11.1 mmol/L)
• A1C (hemoglobin A1C, HbA1C, glycated hemoglobin, and glycosylatedhemoglobin test) values ≥6.5 percent (48 mmol/mol).
In the absence of symptomatic hyperglycemia, the diagnosis of diabetes must be
confirmed by repeated measurement, repeating the same test for confirmation.
However, if two different tests (eg, FPG and A1C) are available and are concordant
for the diagnosis of diabetes, additional testing is not needed.
Urine analysis must also be done for glucosuria, ketonuria. Other investigations
include: full blood count, proteins into urine, blood urea and electrolytes, liverbiochemistry, lipidemia and cholesterol levels, etc.
Adequate medical diagnosis
Plan of management of each type of diabetes mellitus
The goal of diabetes management is to keep blood glucose levels as close to normal
as safely possible. Since diabetes may greatly increase risk for heart disease and
peripheral artery disease, measures to control blood pressure and cholesterol
levels are an essential part of diabetes treatment as well.
People with diabetes must take responsibility for their day-to-day care. This includes
monitoring blood glucose levels, dietary management, maintaining physical
activity, keeping weight and stress under control, monitoring and adhering to oral
medications or insulin use via injections. To help patients achieve this, the health
care facility must offer self-management educational programs that emphasize
individualized diabetes care.
The plan of management of diabetes mellitus includes:A. Dietary management and physical activity
Modifying eating habits and increasing physical activity are typically the first steps
toward reducing blood sugar levels. The benefits of exercises include to improve
insulin sensitivity, to lower blood glucose during and after exercise, to improve lipid
profile, may improve some hypertension, to assist with weight loss, to promotecardiovascular fitness, to increase strength and flexibility, to improve sense of wellbeing.
The patient must also know some risks of exercises: precipitation or exacerbation
of cardiovascular disease, angina, dysrrhythmias, sudden death, hypoglycemia if
taking insulin or oral agents, late onset post-exercise hypoglycemia, hypoglycemia
after very strenuous exercise, worsening of long-term complications such as
proliferative retinopathy, peripheral neuropathy. The patient must also know that
taking some glucose before an exercise may be necessary to minimize the risk forhypoglycemia. Blood glucose check up before and after exercise is necessary.
B. Insulin Therapy
People with type 1 diabetes require multiple insulin injections each day to maintain
safe insulin levels. Insulin is often required to treat type 2 diabetes too. The pump
is about the size of a pager and is usually worn on your belt. Insulin is delivered
through a small syringe that contains the small and thin needle that is placed under
the skin (usually in the abdomen) during injection. There are four major types ofinsulin: rapid-acting, short-acting, intermediate-acting and long-acting.
C. Oral Medications/Hypoglycemia
Sometimes blood sugar levels remain high in people with type 2 diabetes even
though they eat in a healthy manner and exercise. When this happens, medications
taken in pill form may be prescribed. The medications work in several different ways.
These include improve the effectiveness of the body’s natural insulin, reduce blood
sugar production, increase insulin production and inhibit blood sugar absorption.Oral diabetes medications are sometimes taken in combination with insulin.
Oral hypoglycemia agents in type 2 diabetes in early stages are e.g biguanides such
as Metformin reduces hepatic glucose production, Thiazolidinediones/glitazones
reduce insulin resistance, alpha-Glucosidase inhibitors such as miglitol reducepostprandial hyperglycemia by delaying glucose absorption.
D. Monitor glycemia before meal and before bedtime
C. Education to diabetic patients: Education about signs and symptoms of
hypoglycemia, During any journey, the patient should carry the drugs on him/her.
The diabetic card is also necessary, and the patient should not forget to carry some
foods or fluid containing sugar to take in case of hypoglycemia,
Education on self-injection: number of injections per day, way of administration (S/C
route) and site of injection, General hygiene specifically feet hygiene, Educate the
patient and the family the importance of insulin therapy and some complications
of diabetes if insulin is not taken carefully, Don’t forget the importance of diabetic
regimen, Advise the patient to join diabetic associations (it will help her or him
to have medication on low cost, and he/she will learn more about the diabetes
mellitus). FOOT CARE is also very important due to these three major factors that
interact in foot problems in diabetes: neuropathy, ischemia, and sepsis. Therefore
patient must also be educated to never soak feet, wash feet daily and dry them well,
playing attention to the area between the toes, inspect the feet daily (color changes,
swelling, cuts, cracks in the skin, redness, blisters, temperature changes), never
walk barefoot. Always wear shoes or slippers, wear well-fitting shoes, after bathing,
when toenails are soft, cut nails straight across and don’t cut into the corners, if feet
are dry, apply lotion or cream; don’t put lotion between the toes, consult a podiatristfor any problem of the feet.
Evolution and complications of type 1 and 2 diabetes mellitus
Diabetes mellitus is a chronic disease and does not have a cure, except for the case
of gestational diabetes which usually disappears after childbirth. Among diabetes
mellitus complications, there are Acute that develop suddenly and Long-term
complications of diabetes that develop gradually. The longer you have diabetes and
the less controlled your blood sugar the higher the risk of complications. Eventually,diabetes complications may be disabling or even life-threatening.
Acute complications include diabetic ketoacidosis (DKA), Hperglycemic
Hyperosmolar nonketonic coma (HHNC/HHS), Hypoglycemia, the somogyi effect
(happens when patient takes insulin before bed and wake up with high blood
sugar levels; according to the theory of the Somogyi effect, when insulin lowers the
blood sugar too much, it can trigger a release of hormones that send the blood sugar
levels into a rebound high), the dawn phenomenon (early morning hyperglycemiadue to the liberation of growth hormone during nighttime).
Possible long-term complications include:
• Cardiovascular disease: diabetes dramatically increases the risk of various
cardiovascular problems, including coronary artery disease with chest pain
(angina), heart attack, stroke and narrowing of arteries (atherosclerosis).
• Nerve damage (neuropathy): excess sugar can injure the walls of the tiny
blood vessels (capillaries) that nourish the nerves, especially in the legs. This
can cause tingling, numbness, burning or pain that usually begins at the tips
of the toes or fingers and gradually spreads upward. Left untreated, it can
lead to loss of all sense of feeling in the affected limbs. Damage to the nerves
related to digestion can cause problems with nausea, vomiting, diarrhea orconstipation. For men, it may lead to erectile dysfunction
• Kidney damage (nephropathy): the kidneys contain millions of tiny blood
vessel clusters (glomeruli) that filter waste from the blood. Diabetes can
damage this delicate filtering system. Severe damage can lead to kidney
failure or irreversible end-stage kidney disease, which may require dialysis
or a kidney transplant.
• Eye damage (retinopathy): diabetes can damage the blood vessels of the
retina (diabetic retinopathy), potentially leading to blindness. Diabetes also
increases the risk of other serious vision conditions, such as cataracts and
glaucoma.
• Foot damage: nerve damage in the feet or poor blood flow to the feet increases
the risk of various foot complications. Left untreated, cuts and blisters can
develop serious infections, which often heal poorly. These infections may
ultimately require toe, foot or leg amputation.
• Skin conditions: diabetes may leave a person to more susceptible to skin
problems, including bacterial and fungal infections.
• Hearing impairment: hearing problems are more common in people with
diabetes.
• Alzheimer›s disease: type 2 diabetes may increase the risk of dementia,
such as Alzheimer›s disease. The poorer the blood sugar control, the greater
the risk appears to be.
• Depression: depression symptoms are common in people with type 1 and
type 2 diabetes. Depression can affect diabetes self-management leading topoor outcomes.
Complications of gestational diabetes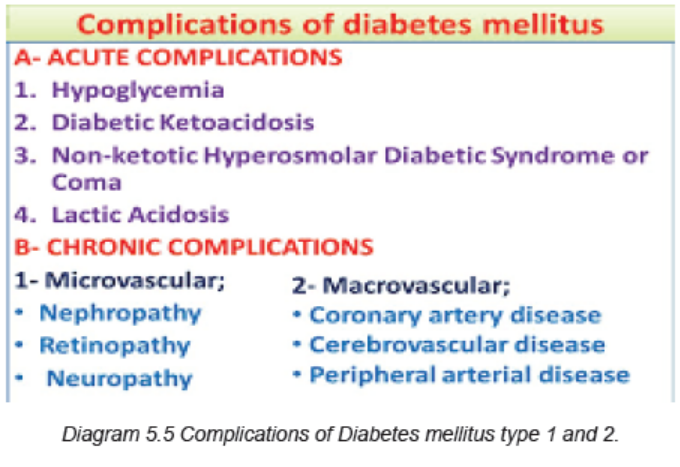
Most women who have gestational diabetes deliver healthy babies. However,
untreated or uncontrolled blood sugar levels can cause problems for the mother
and/or the baby.
Complications to the baby can occur as a result of gestational diabetes, including:
– Excess growth: Extra glucose can cross the placenta, which triggers the
baby›s pancreas to make extra insulin. This can cause the baby to grow too
large (macrosomia). Very large babies are more likely to require a C-section
birth.
– Low blood sugar: Sometimes babies of mothers with gestational diabetes
develop low blood sugar (hypoglycemia) shortly after birth because their own
insulin production is high. Prompt feedings and sometimes an intravenous
glucose solution can return the baby›s blood sugar level to normal.
– Type 2 diabetes later in life: Babies of mothers who have gestational
diabetes have a higher risk of developing obesity and type 2 diabetes later
in life.
– Death: Untreated gestational diabetes can result in a baby›s death either
before or shortly after birth.
– Complications to the mother also can occur as a result of gestational
diabetes, including:
– Preeclampsia: This condition is characterized by high blood pressure, excess
protein in the urine, and swelling in the legs and feet. Preeclampsia can lead
to serious or even life-threatening complications for both mother and baby.
– Subsequent gestational diabetes. Once a pregnant women had gestational
diabetes in one pregnancy, she will be more likely to have it again with the
next pregnancy. She is also more likely to develop diabetes typically type 2
diabetes — as she gets older.
Very serious and Acute Complications of Diabetes Mellitus (DKA and HHS)
A. DIABETIC KETOACIDOSIS (DKA)
DKA results from relative or absolute insulin deficiency (lack of insulin, insulin
omission). The decreased ratio of insulin to glucagon promotes gluconeogenesis,
glycogenolysis, and ketone body formation in the liver. Ketosis results from a
marked increase in free fatty acid release from adipocytes, with a resulting shift
toward ketone body synthesis in the liver. Reduced insulin levels, in combination
with elevations in catecholamines and growth hormone, increase lipolysis and therelease of free fatty acids. DKA is more present in type 1 diabetes mellitus.
Causes of DKA
• DKA is the initial manifestation of diabetes in 20% of adults and 30–40% of
children with type 1 diabetes.
• In patients with established diabetes, causes of DKA include:
• Infection (30%-50%)
Most common infections urinary tract infection and pneumonia
• Noncompliance with insulin• Psychological stress
Clinical manifestations include: Hyperglycemia, Ketosis: ketonuria, serum ketone
(ketonemia), ketone smelling (fruity odor), Metabolic acidosis, Hyperlipoproteinemia,
Nausea, Signs of acidosis (Kussmaul respiration, acetone breath), Signs of volume
depletion/ dehydration, Polyuria, polydipsia, polyphagia, weight loss, Fever due to
underlying infection is common(if present), Gastrointestinal signs (abdominal pain,
vomiting), Neurological signs (hemiparesis and seizures) related to metabolicacidosis.
Diagnosis of DKA
• Serum glucose level > 250 mg/dL
• Serum bicarbonate < 18 mg/dL
• Serum pH < 7.30
• Presence anion gap
• History and physical examination,
• Blood studies including immediate blood glucose, complete blood count, pH,
ketones, electrolytes, blood urea nitrogen, arterial or venous blood gases.• Urinalysis, including specific gravity, glucose, acetone
Management of DKA:
1. Confirm diagnosis (↑plasma glucose, positive serum ketones, metabolic
acidosis).
2. Admit to hospital (unconsciousness, PH < 7 )
3. Assess: serum electrolytes (K+, Na+, Mg2+, Cl-, bicarbonate, phosphate),
acid-base status (pH, HCO3-, PCO2), renal function (creatinine, urine output)
4. Replace fluids: 2–3 L of 0.9% saline over first 1–3 h (10–15 mL/kg per hour);
5. Administer short-acting insulin: IV (0.1 unit/kg/hour) or IM/ SC (0.3 units/
kg). Insulin increases peripheral glucose utilization and decreases hepatic
glucose production. If initial serum potassium is < 3.3 mmol/L (3.3 meq/L), donot administer insulin until the potassium is corrected to > 3.3 mmol/L.
6. Give medication to correct hyperkalemia (urgent treatment of hyperkalemia
includes stabilizing the myocardium to protect against arrhythmias and
shifting potassium from the vascular space into the cells. Intravenous calcium
(eg: calcium gluconate) is administered to stabilize the myocardium; it lowers
the threshold potential, thus counteracting the toxic effect of high potassium.
Other medications like sodium polystyrene sulfonate (Kaayexalate) works by
helping the body get rid of extra potassium through feces, etc.
7. Electrolyte replacement
8. Assessment of mental status, Assessment of blood glucose levels, Assessment
of blood and urine for ketones, Assessment of cardiovascular and respiratory
status and ECG monitoring, Assess patient: What precipitated the episode
(noncompliance, infection, trauma, alcohol?
9. Monitoring and recording of intake and output
10. Central venous pressure monitoring (if indicated)
11. Measure capillary glucose every 1–2 h; measure electrolytes (especially K+,
bicarbonate, phosphate) and anion gap every 4 h for first 24 h.
12. Initiate appropriate workup for precipitating event (cultures, Chest X-Ray,ECG).
The complications of diabetic ketoacidosis
DKA can cause complications such as low levels of potassium (hypokalemia) that
can cause severe problems like muscle weakness and heart rhythm problems
which can cause death), swelling inside the brain (cerebral edema), fluid inside the
lungs (pulmonary edema), damage to the kidney or other organs from the fluid loss.All these can lead to sudden death.
B. HYPERGLYCEMIC HYPEROSMOLAR NONKETONIC COMA/STATUS(HHCN/HHS)
This is a complication of type 2 diabetes mellitus especially for the elderly people.
Hyperglycemia induces an osmotic diuresis that leads to intravascular volume
depletion, which is exacerbated by inadequate fluid replacement (impaired patient’s
perception of thirst due to underlying cerebrovascular disease). The polyuriadisappears early because of the severe dehydration.
Clinical manifestations
• Severe dehydration (fluid deficit of 8-9 L)
• Severe hyperglycemia (plasma glucose may be >55.5 mmol/L (1000 mg/dL)• Hyperosmolarity (>350 mosmol/L)
Management
• IV replacement with hypotonic solutions (0.45% normal saline)
• IV insulin is not needed, give insulin subcutaneously
Possible complications of untreated HHS are shock, blood clot formation, brain
swelling (cerebral edema) or increased blood acid level (lactic acidosis).
C. HYPOGLYCEMIA
The hypoglycemia in diabetic person is due to insulin therapy or glucose lowering
agents:
• Insulin overdosage
• Glucose lowering agents overdosage
• Inconsistent carbohydrates intake (no glucose intake before insulin injection)
• Alcohol consumption
• Uncompensated exercise• Patient with end-stage renal or liver failure are at risk for hypoglycemia
Signs and symptoms
Adrenergic symptoms (hypoglycemia causes the liberation of chathecholamines
particulary adrenalin as compensatory mechanism): pallor, diaphoresis, tachycardia,
palpitation, nervousness, irritability, sensation of coldness, weakness, trembling,
hunger.
Neuroglycopenic symptoms: the low glucose in nervous system causes
headache, mental confusion, fatigue, incoherent speech, coma, diplopia, emotionallability, and convulsion.
Self-assessment 5.1
Read the clinical case scenario below and answer the followingquestions:
A 27year old man was brought to the emergency reception reporting severe
weakness, dizziness, and sleepiness all the time. Upon questioning, he reported
increased and not resolving thirst, and the repeated need to urinate. Although
he ate all of his rations as well as whatever he could get from his family, he had
lost 7 kgs during recent 9 months. On the previous day before his consult, he
complained of vague abdominal pain, which was worse on the morning and had
vomited once. During the physical examination, he was oriented but tachypneic
(pulse rate of 138 beats per minute) and his blood pressure was 90/60 mm
Hg. He appeared pale, dehydrated with dry mucous membranes, and poor
skin turgor. His respiratory rate was 36 cycles per minute with deep, laborious
breathing. After admission, the laboratory investigations showed blood glucose
levels of 560 mg/dl, sodium 154, potassium 6.5, pH 7.10, bicarbonate 10 mM/liter,
chloride 90, BUN 38 mg/dl, creatinine 2.5 mg/dl. (Normal values: glucose: 70-
110 mg/dl; Na = 135-145; K, 3.5-5.5; Cl, 98-108; CO2, 20-32 [all in mM/l]; BUN,
7-22mg/dl; creatinine, 0.7-1.5 mg/dl). A urine sample was 4+ for glucose and
had “large” acetone. Glycated hemoglobin (HbA1c) was 14% (normal=4-6.2%).
He was treated with insulin and normal saline I.V. initially and by the 4th hour
of treatment, potassium chloride was added to the IV at a rate of 15 mEq/hour.
Sixteen hours later, he was active, alert, well hydrated and cheerful, indicating
he felt extremely well. He requested that his IV be discontinued. His physician
decided to switch his insulin to subcutaneous injections and to start a liquid diet.
He was later put on a diabetes maintenance diet and treated with one injection of
Human Lente insulin in the morning. Although his blood sugars the next morning
were 100-140 mg/dl, he had frequent episodes of hypoglycemia during the day,
he was put on 3 injections of regular insulin/day, and a bedtime intermediate
duration (Lente) insulin.
1. Basing on the case presented above, what was the medical condition that
the patient was presenting?
2. What are the signs and symptoms that guided you in thinking about that
medical diagnosis?
3. What are different investigations requested to confirm that medical
condition?
4. What are all possible treatment options are available to that medical
condition?5. If it is not properly managed, what are the possible complications?
5.2 END UNIT 5 ASSESSMENT
End unit assessment
1. Explain how the pancreas serves both endocrine and exocrine functions.
2. By definition, differentiate diabetes mellitus type one and two
3. Give 5 risk factors of type one and two of diabetes mellitus.
4. What are the general signs and symptoms of diabetes mellitus?
5. What are the investigations that are relevant into the diagnosis of diabetes
mellitus?
6. Discuss different management principles of diabetes mellitus.
7. Discuss how the diabetes mellitus can lead to kidney, eye and foot
problems.
8. Basing on the causes and signs and symptoms, differentiate the DKA and
HHS.
9. What are different management principles of DKA?
10. In addition to promoting the transport of glucose from the blood into the
cell, what does insulin do?
a. Enhances the breakdown of adipose tissue for energy
b. Stimulates hepatic glycogenolysis and gluconeogenesis
c. Prevents the transport of triglycerides into adipose tissue
d. Accelerates the transport of amino acids into cells and their synthesisinto protein
11. Why are the hormones cortisol, glucagon, epinephrine, and growth
hormone referred to as counter regulatory hormones?
a. Decrease glucose production
b. Stimulate glucose output by the liver
c. Increase glucose transport into the cells
d. Independently regulate glucose level in the blood
12. What characterizes type 2 diabetes?
a. β-Cell exhaustion
b. Insulin resistance
c. Genetic predisposition
d. Altered production of adipokines
e. Inherited defect in insulin receptors
f. Inappropriate glucose production by the liver
13. Which laboratory results would indicate that the patient has prediabetes?
a. Glucose tolerance result of 132 mg/dL
b. Glucose tolerance result of 240 mg/dL
c. Fasting blood glucose result of 80 mg/dL
d. Fasting blood glucose result of 120 mg/dL
14. The nurse is teaching the patient with prediabetes ways to prevent or delay
the development of type 2 diabetes. What information should be included?
a. Maintain a healthy weight.
b. Exercise for 60 minutes each day.
c. Have blood pressure checked regularly.
d. Assess for visual changes on monthly basis
e. Monitor for polyuria, polyphagia, and polydipsia.
15. When teaching the patient with diabetes about insulin administration, the
nurse should include which instruction for the patient?
a. Pull back on the plunger after inserting the needle to check for blood.
b. Consistently use the same size of insulin syringe to avoid dosing errors.
c. Clean the skin at the injection site with an alcohol swab before each
injection.
d. Rotate injection sites from arms to thighs to abdomen with each injection
to prevent lipodystrophies.
16. A patient taking insulin has recorded fasting glucose levels above 200 mg/
dL (11.1 mmol/L) on awakening for the last five mornings. What should the
nurse advise the patient to do first?
a. Increase the evening insulin dose to prevent the dawn phenomenon.
b. Use a single-dose insulin regimen with an intermediate-acting insulin.
c. Monitor the glucose level at bedtime, between 2:00 am and 4:00 am,
and on arising.
d. Decrease the evening insulin dosage to prevent night hypoglycemia
and the Somogyi effect.
17. The nurse is assessing a newly admitted diabetic patient. Which observation
should be addressed as the priority by the nurse?
a. Bilateral numbness of both hands
b. Stage II pressure ulcer on the right heel
c. Rapid respirations with deep inspiration
d. Areas of lumps and dents on the abdomen
18. The nurse should observe the patient for symptoms of ketoacidosis when:
a. Illnesses causing nausea and vomiting lead to bicarbonate loss with
body fluids.
b. Glucose levels become so high that osmotic diuresis promotes fluid
and electrolyte loss.
c. An insulin deficit causes the body to metabolize large amounts of fatty
acids rather than glucose for energy.
d. The patient skips meals after taking insulin, leading to rapid metabolism
of glucose and breakdown of fats for energy.
19. What are manifestations of diabetic ketoacidosis (DKA)?
a. Thirst
b. Ketonuria
c. Dehydration
d. Metabolic acidosis
e. Kussmaul respirations
f. Sweet, fruity breath odor
20. What describes the primary difference in treatment for diabetic ketoacidosis
(DKA) and hyperosmolar hyperglycemic syndrome (HHS)?
a. DKA requires administration of bicarbonate to correct acidosis.
b. Potassium replacement is not necessary in management of HHS.
c. HHS requires greater fluid replacement to correct the dehydration.
d. Administration of glucose is withheld in HHS until the blood glucose
reaches a normal level.
21. A diabetic patient is found unconscious at home and a family member calls
the clinic. After determining that a glucometer is not available, what should
the nurse advise the family member to do?
a. Have the patient drink some orange juice.
b. Administer 10 U of regular insulin subcutaneously.
c. Call for an ambulance to transport the patient to a medical facility.
d. Administer glucagon 1 mg intramuscularly (IM) or subcutaneously.
22. The patient with diabetes is brought to the emergency department by his
family members, who say that he is not acting like himself and he is more
tired than usual. Number the nursing actions in the order of priority for this
patient.
a. Establish IV access.
b. Check blood glucose.
c. Ensure patent airway.
d. Begin continuous regular insulin drip.
e. Administer 0.9% NaCl solution at 1L/hr.
f. Establish time of last food and medication(s).
23. What disorders and diseases are related to macrovascular complications
of diabetes?
a. Chronic kidney disease
b. Coronary artery disease
c. Microaneurysms and destruction of retinal vessels
d. Ulceration and amputation of the lower extremitiese. Capillary and arteriole membrane thickening specific to diabetes