UNIT 4 MEDICAL PATHOLOGIES OF UROGENITAL SYSTEM
Key Unit Competencies
To take an appropriate decision on management of different common medicalpathologies of urogenital system.
Introductory activity 4.0
Observe the image below and answer the questions that follow.
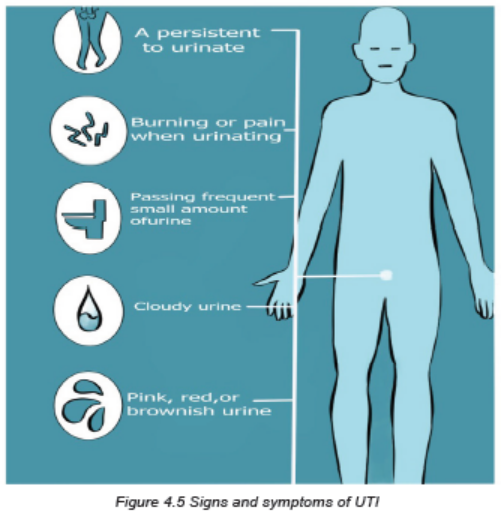
Figure 4.1 Urinary tract infection
1. What do you observe on the picture?
2. What do you think will happen if the microorganisms enter in the urinary
system?3. How do you think the microorganisms can enter in the urinary system?
4.1 URINARY TRACT INFECTION (UTI)
Learning Activity 4.1
Carefully read the case below and answer the following questions:
A.K., man of 45 years old was brought at Muhima Hospital in a private car with
his knees bent and drawn to his abdominal area. In the history, he reported to
have unprotected sex 3 days ago with a person whom he doesn’t know. He
appears restless and keeps moving from back to side in an effort to reduce his
discomfort. At arrival, the vital signs were blood pressure 156/70 mmHg, Pulse
108 beats per minute, respiratory rate 24 cycles per minute, temperature 37.4° C,
O2 saturation 96% on room air. He was awake, alert, and oriented. Lungs were
clear on auscultation. The abdomen not distended with positive bowel sounds in
all 4 quadrants and no rebound tenderness. He had costovertebral tenderness
and mild pain when palpating the hypogastric pain (lower parts of the abdomen).
He was voiding small amounts (pollakyuria) of chocolate urine with aromatic odor
and had burning during urination (dysuria). From the investigations done, the
patient had elevated white blood cells of 13000, and the abdominal ultrasound
and urine culture were pending. The health care provider prescribed opioids forpain management, IV fluids and admitted A.K for further management.
1. Basing on case described, what are the abnormal signs and symptoms the
patient was presenting?
2. What are the investigations that have been requested to that patient? What
were their rationales?
3. What was the medical problem that the patient was presenting?
4. From the case study and what you know, what are all possible causes or
risk factors to develop that medical condition?
5. What must be included into the management plan of that medical condition?
6. If not treated, what might be the consequences?
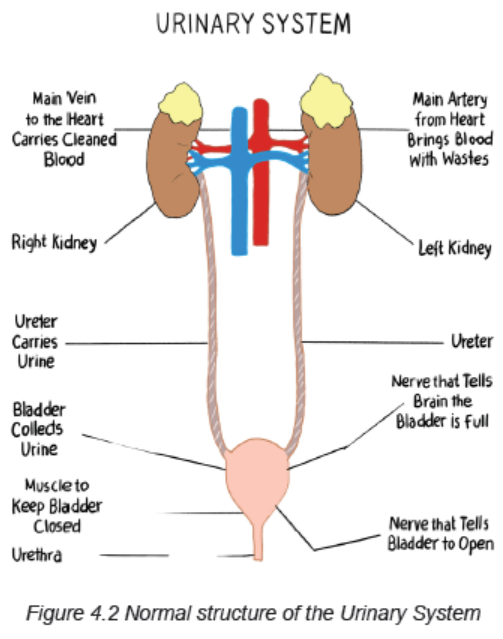
Adequate kidney function is essential to the maintenance of a healthy body. The
upper urinary system consists of two kidneys and two ureters. The lower urinary
system consists of a urinary bladder and a urethra. Urine is formed in the kidneys,
drains through the ureters to be stored in the bladder, and then passes from the
body through the urethra.
The kidneys have also many other functions including excreting excess water andnitrogenous waste products of protein metabolism, assisting in maintenance of acid
base and electrolyte balance, producing the enzyme renin, which helps regulate
blood pressure, and producing the hormone erythropoietin, which stimulates
red blood cell production. The remainder of the urinary system is involved in thetransport (ureters), storage (bladder), and excretion (urethra) of urine.
Renal and urologic disorders encompass a wide spectrum of problems. The
diverse causes of these disorders may involve infectious, immunologic, obstructive,
metabolic, collagen, vascular, traumatic, congenital, neoplastic, and neurologicmechanisms.
Urinary tract infection (UTI) is an inflammation of the urinary epithelium in response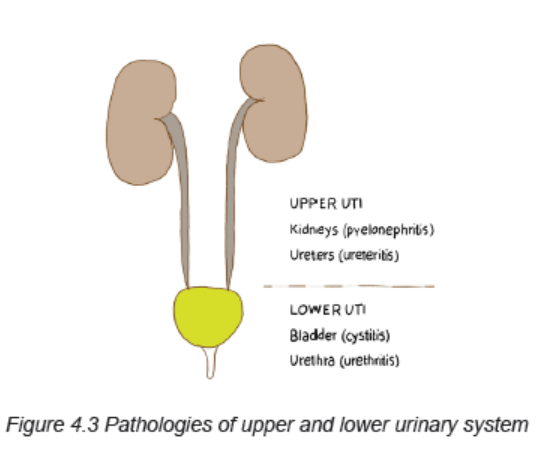
to colonization from a pathogen. The urinary tract infections can be classified as
complicated or uncomplicated. Uncomplicated UTI occur in a normal urinary tract
and usually involve only the bladder. Complicated UTI include those infections with
coexisting obstruction, stones, or catheters, diabetes or neurologic diseases, or
pregnancy-induced changes. The term Complicated UTI also applies to a recurrent
infection. The individual with a complicated infection is at risk for pyelonephritis,
uro-sepsis, and renal damage.
The most common urologic disorders are infectious and inflammatory conditions.
Those that affect the kidneys are extremely dangerous because damage to the
nephrons can result in permanent renal dysfunction.
The bladder is usually free from bacteria and the urinary tract above the urethra is
normally sterile. Several mechanical and physiologic defense mechanisms assist
in maintaining sterility and preventing urinary tract infection (UTI). These defenses
include normal voiding with complete emptying of the bladder, ureterovesical
junction competence, and ureteral peristaltic activity that propels urine toward the
bladder. Antibacterial characteristics of urine are maintained by an acidic pH (less
than 6.0), high urea concentration, and abundant glycoproteins that interfere with
the growth of bacteria. An alteration in any of these defense mechanisms increasesthe risk for a UTI.
Types of UTI
– Uncomplicated (isolated) UTI is either a 1st infection or an infection that
occurs at least 1 year after any prior UTI.
– Recurring UTI is diagnosed when the person experiences an initial infection
that is successfully treated, followed by reappearance of the infection no
sooner than 5 to 10 days after resolution of the original episode.
– Persistent UTI is persistence of infection despite at least 3 days of treatment
with an antibiotic.
Causes and risk factors
Inflammation of the urinary tract may be caused by a variety of disorders, but
bacterial infection is the most common.
The organisms that usually cause UTI are introduced via the ascending route from
the urethra and originate in the perineum.
The commonest causes of UTI are:
– Bacteria which are the most common cause of UTI (Escherichia coli, Neisseria
gonorrhea, Chlamydia trachomatis, Klebsiella, Proteus, Staphylococcus,
mycoplasma, Pseudomonas)
– Fungi (Candida albicans)
– Viruses
– Parasites (e.g. Trichomonas Vaginalis)
Another common factor contributing to ascending infection is urologic instrumentation
(e.g., catheterization, cystoscopic examinations). This instrumentation allows
bacteria that are normally present at the opening of the urethra to enter into the
urethra or bladder.
Sexual intercourse promotes “milking” of bacteria from the vagina and perineum
and may cause minor urethral trauma that predisposes women to UTI.
Rarely the UTI result from a hematogenous route, where blood-borne bacteria
secondarily invade the kidneys, ureters, or bladder from elsewhere in the body.
There must be prior injury to the urinary tract, such as obstruction of the ureter,
damage caused by stones, or renal scars, for a kidney infection to occur from
hematogenous transmission.
Other risk factors of UTI are premature infants, sexually active women, women using
a diaphragm and spermicide, individuals with diabetes mellitus, individuals with
advanced HIV or immunosuppressive disorders, people with recent instrumentation
of urinary system or indwelling catheterization, people with obstruction of the lower
urinary tract.
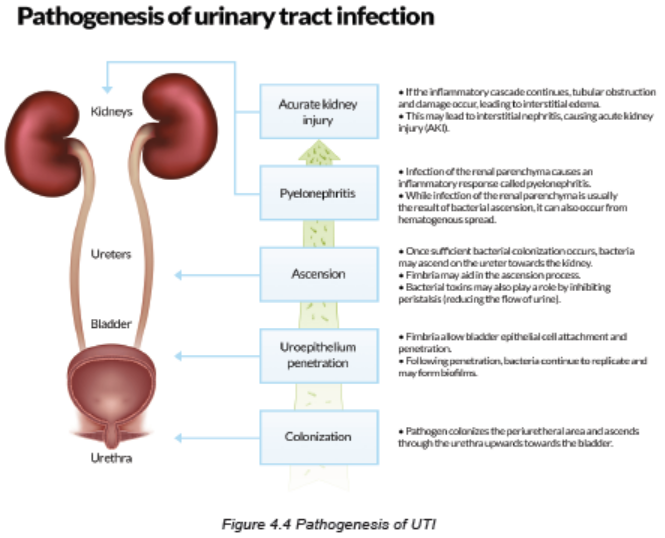
Pathophysiology overview
A UTI occurs when a pathogen overwhelms the host’s defense mechanisms and
colonizes the urinary system with proliferation of bacteria, fungi, or parasite and
the person raises a response to this invasion. The ability of the bacteria to adhere
(attach) to the uro-epithelium influences its virulence. Adherence enhances bacterial
persistence despite micturition that increase the risk for recurring UTI.
Causes of bacterial persistence include bacterial resistance to the antibiotic,
emergence of resistant secondary bacterial strain after the primary microorganism
is eradicated, renal insufficiency causing poor excretion of the antibiotic in the urine,a foreign body such as stone acting as a harbor for bacteria, and papillary necrosis.
Signs and Symptoms
Lower urinary tract symptoms are experienced in patients who have UTI of the
upper urinary tract, as well as those confined to the lower tract. Symptoms are
related to either bladder storage or bladder emptying. These symptoms include
dysuria, frequent urination (more than every 2 hours), urgency, and suprapubic
discomfort or pressure. The urine may contain grossly visible blood (hematuria) or
sediment, giving it a cloudy appearance. Flank pain, chills, and fever indicate an
infection involving the upper urinary tract (pyelonephritis). People with significant
bacteriuria may have no symptoms or may have nonspecific symptoms such as
fatigue or anorexia.
The UTI symptoms are often absent in older adults as they tend to experience
non localized abdominal discomfort rather than dysuria and suprapubic pain. In
addition, they may have cognitive impairment or generalized clinical deterioration.
The older adults are less likely to experience a fever with a UTI, the value of body
temperature as an indicator of a UTI is unreliable.
Investigations
In a patient suspected of having a UTI:
• Initially obtain a dipstick urinalysis to identify the presence of nitrites
(indicating bacteriuria), white blood cells (WBCs), and leukocyte esterase (an
enzyme present in WBCs indicating pyuria). These findings can be confirmed
by microscopic urinalysis.
• After confirmation of bacteriuria and pyuria, a urine culture may be obtained.
A urine culture is indicated in complicated UTI, persistent bacteriuria, or
frequently recurring UTI (more than two or three episodes per year). Urine
may also be cultured when the infection is unresponsive to empiric therapy
or the diagnosis is questionable. A urine culture is accompanied by sensitivity
testing to determine the bacteria’s susceptibility to a variety of antibiotic drugs.
• Imaging studies of the urinary tract like intravenous pyelogram (IVP),
cystoscopy, ultrasound can be performed. A computed tomography (CT)
urogram or ultrasound may be obtained when obstruction of the urinary
system is suspected or UTI occurs.
Adequate medical diagnosis
Most patients with urinary tract infection (UTI) can be managed as outpatients.
Indications for hospitalization include clinical uro-sepsis, immunocompromised
patient, vomiting or inability to tolerate oral medication, lack of outpatient followup,
and failure to respond to outpatient therapy. Empiric antimicrobial therapy
immediately after appropriate urine collection is warranted from patients with a high
probability of UTI based on the clinical and laboratory data available. Definitive
therapy is based upon the results of urine culture and sensitivities. There are other
investigations that must be performed like imaging.

Treatment plan
The goals of treatment of UTI include:
• Elimination of infection and prevention of uro-sepsis
• Relief of acute symptoms (eg, fever, dysuria, frequency)
• Prevention of recurrence and long-term complications including hypertension,
renal scarring, and impaired renal growth and function.
• Treatment to be effective should be oriented to both people if it is a couple
Interventions that must be carried out to meet those goals are:
• Ensuring adequate fluid intake if it is not contraindicated. Maintaining
adequate fluid intake may be difficult because of the patient’s perception that
fluid intake will worsen the discomfort and urinary frequency associated with
a UTI. Tell patients that fluids will increase frequency of urination at first but
will also dilute the urine, making the bladder less irritable. Fluids will help flush
out bacteria before they have a chance to colonize in the bladder. Caffeine,
alcohol, citrus juices, chocolate, and highly spiced foods or beverages should
be avoided because they are potential bladder irritants.
• Application of local heat to the suprapubic area or lower back may relieve the
discomfort associated with a UTI. Advise the patient to apply a heating pad
(turned to its lowest setting) against the back or suprapubic area. A warm
shower or sitting in a tub of warm water filled above the waist can also provide
temporary relief.
• Instruct the patient about the prescribed drug therapy, including side effects.
Emphasize the importance of taking the full course of antibiotics. Often
patients stop antibiotic therapy once symptoms disappear. This can lead to
inadequate treatment and recurrence of infection or bacterial resistance to
antibiotics.
• Instruct the patient to monitor for signs of improvement (e.g., cloudy urine
becomes clear) and a decrease in or cessation of symptoms. Teach patients
to promptly report any of the following to their health care provider: (1)
persistence of bothersome UTI beyond the antibiotic treatment course, (2)
onset of flank pain, or (3) fever.
• Antibiotic medications are necessary for the UTI. For treatment of uncomplicated
UTI, oral (by mouth) antibiotics are usually adequate. However, for major
complications such as sepsis or pyelonephritis, intravenous (IV) antibiotics
may be typically necessary. The antibiotics usually used are Nitrofurantoin
(Macrobid), Fosfomycin (Monurol), Trimethoprim-Sulfamethoxazole (Bactrim
and others), Cefixime, Cefuroxime, Cefotaxime or Ceftriaxone, Gentamicin,
Ciprofloxacin (Cipro) or Levofloxacin (Levaquin). Doxycicline or Erythromycin
can also be provided. Metronidazole will be needed in case of Trichomonas
infection or Nystatine in case of candida infection. The choice of regimen
depends on Antimicrobial spectrum and susceptibility, where the ultimate
choice of antimicrobial therapy is based upon the susceptibilities of the
organism isolated. Cephalosporins are the first-line oral agent in the treatment
of UTI among patients without genitourinary abnormalities. Amoxicillin and
ampicillin are not routinely recommended for empiric therapy because of the
high rate of resistance of E. coli.
• Inpatient parenteral therapy: this will require hospitalisation and the parenteral
therapy generally is indicated for the following cases: <2 months, clinical
urosepsis (eg, toxic appearance, hypotension, poor capillary refill), immune
compromise, vomiting or inability to tolerate oral medication, lack of adequate
outpatient follow-up (eg, no telephone, live far from hospital, etc), failure to
respond to outpatient therapy.
• Adjunctive therapies might be used to reduce the renal parenchymal
inflammation which if not treated leads to renal scarring. The therapies used
are anti-inflammatory drugs like Dexamethasone, Prednisolone, etc.
Evolution and complications
If all prescribed regimen are respected, the outcome is very good. Without treatment,
UTI can cause major health problems. Severe effects of a UTI that can develop
include:
• Pyelonephritis (acute or chronic): An infection involving the kidneys
• Sepsis: A dangerous, systemic, whole-body infection
• Renal scarring: due to chronic inflammation of renal parenchyma
• Hypertension: related to ineffective Angiotensin-Renin-Aldosteron
Self-assessment 4.1
1. What are all possible causes or risk factors to develop the urinary tract
infections?
2. What are the signs and symptoms of urinary tract infections?
3. What are the investigations that should be requested to make the diagnosis
of urinary tract infections?
4. What are their rationales?
5. What must be included into the management plan of that medical condition?
6. If not treated, what are the complications of UTIs?
4.1.1 URETHRITIS
Learning Activity 4.1.1
Carefully read the case below and answer the following questions:
A male patient aged around 25 years came to our hospital with the complaints
of discharge per urethra since 2 days. He also had burning micturition since
10 days which was followed 12 hours later by foul smelling white discharge
from urethra which continued to be present till the day he visited the hospital.
He also gave history of unprotected sexual intercourse with a commercial sex
worker 2 days prior to the onset of all symptoms. On examination, there was
mucopurulent discharge from urethra.
The meatus was cleaned using gauze soaked in saline. The discharge was
collected using a sterile swab under aseptic precautions. It was processed
for Gram staining and showed many pus cells and intracellular gram negative
diplococci, with adjacent sides concave (Kidney shaped). On chocholate agar
colonies were small, round, slightly raised and greyish white. Gram staining was
done from the colonies which showed gram negative diplococci. He was treated
with ciprofloxacin 500mg two times a day for 10 days, metronidazole 2gr single
dose and doxycycline 100mg two times a day and ibuprofen 400mg three times
a day for 3 days.
1. What are the possible medical conditions of this patient?
2. What are the signs and symptoms of this medical condition?
3. What are the causes of this above medical condition?
4. What are the investigations that should be used to diagnose that medical
condition?
5. Propose the treatment plan regarding this medical condition
6. If the patient is not well treated what are possible complications?
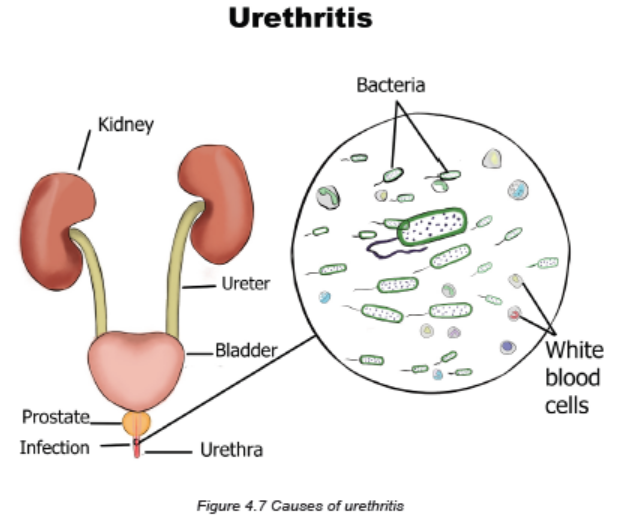
Urethritis is an inflammation of urethra that is the tube that carries urine from the
bladder to outside the body.
Causes and risk factors
Urethritis is an inflammatory condition that can be infectious or posttraumatic
in nature. Infectious causes of urethritis are typically sexually transmitted and
categorized as either gonorrhoea urethritis (ie, due to infections with Neisseria
gonorrhoeae) or non-gonorrhoea urethritis (eg, due to infections with Chlamydia
trachomatis, Ureaplasma urealyticum, Mycoplasma hominis, Mycoplasma
genitalium, or Trichomonas vaginalis). Bacteria that normally are present cause
no difficulty unless these tissues are traumatized, usually after instrumentation
such as catheterization or cystoscopic examination. Other causes of nonspecific
urethritis in men include irritation during vigorous intercourse, rectal intercourse, or
intercourse with a woman who has a vaginal infection.
Urethritis is seen more commonly in men than in women. In women, urethritis may
accompany cystitis but also may be secondary to vaginal infections. Soaps, bubble
baths, sanitary napkins, or scented toilet paper also may cause urethritis. In men, a
common cause of urethritis is infection with Chlamydia trachomatis or Ureaplasma
urealyticum, which causes an STI. The distal portion of the normal male urethra is
not totally sterile.
Pathophysiology
The pathogenesis of urethritis depends on the causative pathogen. N.
gonorrhea is usually transmitted via the genital tract to the human host. Following
attachment to host cell, which is mediated by pili, gonococci become engulfed
in a process known as parasite-directed endocytosis. This organism will survive
inside the vacuoles and replicate. Among non-gonorrheal causes, Chlamydia
trachomatis is the most common. The infectious process begins with cell surface
attachment and phagocytosis by the host cell. The pathogen survives inside
the cell by debilitating the cellular lysosomes and replicating as elementary bodies
which is considered as the infective form of the pathogen.
Signs and symptoms
Infection of the urethra results in discomfort on urination varying from a slight
tickling sensation to burning or severe discomfort and urinary frequency. Fever is
not common, but fever in the male client may be due to further extension of the
infection to areas such as the prostate, testes, and epididymis.
Urethritis can cause itching, pain, or discomfort when a person is not urinating, pain
during sexual intercourse, discharge from the urethral opening or vagina, in men
there can be blood in the semen or urine.
Investigations
The diagnosis of urethritis relies on:
• Physical examination that includes the genitals, abdomen, and rectum.
• Urine tests and culture for gonorrhea, chlamydia, or other bacteria.
• Examination of any discharge under a microscope
• Blood tests may be done in certain situations.
Adequate medical diagnosis
The client’s history and symptoms often provide a tentative diagnosis. In men,
a urethral smear is obtained for culture and sensitivity to identify the causative
microorganism. In women, a urinalysis (clean-catch midstream specimen) may
identify the causative microorganism.
Treatment plan
Treatment includes appropriate antibiotic therapy (doxycycline, azithromycin,
ceftriaxone, etc), liberal fluid intake, analgesics, warm sitz baths, and improvement
of the client’s resistance to infection by a good diet and plenty of rest. If urethritis is
due to an STI, it is treated with appropriate antibiotic therapy. Oral Antibiotic treatment
for 1-2 weeks (Men 2 weeks recommended). Urethritis due to trichomonas infection
(called trichomoniasis) is usually treated with an antibiotic called metronidazole
(Flagyl). Tinidazole (Tindamax) is another antibiotic that can treat trichomoniasis.
The nurse reinforces the need to complete antibiotic therapy, drink plenty of fluids,
and take warm sitz baths and analgesics for pain. Urethritis may be seen in clients
with indwelling urethral catheters. To prevent or decrease urethritis, the nurse needs
to be vigilant with sterile technique, as well as to exercise gentleness when changing
catheters. It also is essential to provide frequent perineal care, especially if the
client is incontinent of faeces. In addition to washing around the anus and buttocks,
the nurse also cleans the meatus and labia of the female client. When cleaning the
anal area, wiping away from the urethra ensures that there is no contamination. If
cotton pledgets are used, the nurse wipes from the urethral meatus to the anus in a
single stroke and discards the pledget. Client teaching information about prevention
include: avoid having intercourse with multiple partners, use condoms every time
you have unsafe sex, get tested regularly, protect others if you find out you have an
STI, inform others who are also at risk of an infection.
Evolution and complications
Failure to seek treatment for gonococcal urethritis may result in a urethral stricture
in men. Medication can often treat urethritis quickly. If the infection goes untreated,
however, the effects can be lasting and quite serious. For example, the infection
may spread to other parts of the urinary tract, including the ureters, kidneys, and
bladder. These infections can be painful on their own. While they can be treated
with more intensive rounds of antibiotics, they can cause damage to the organs if
left untreated for too long. These untreated infections can also spread to the blood
and result in sepsis, which can be deadly.
In addition, the STIs that frequently cause urethritis can damage the reproductive
system. Women may develop pelvic inflammatory disease (PID), which is painful
and can result in infertility, ongoing pelvic pain, or pain during sex. Women with
untreated STIs are also at a higher risk for ectopic pregnancies, which can be lifethreatening.
Men may develop painful inflammation or infection of the prostate
gland, or the narrowing of a section of the urethra due to scarring, leading to painful
urination. Major complications of urethritis are: pyelonephritis, pre-term delivery,
urinary retention, recurrent UTI, prostatitis, sepsis, renal abscess.
Self-assessment 4.1.1
1. What are all possible causes or risk factors to develop the urethritis?
2. What are the signs and symptoms of urethritis?
3. What are the investigations that should be requested to make the diagnosis
of urethritis?
4. What are their rationales?
5. What must be included into the management plan of the urethritis?
6. If not treated, what are the complications of urethritis?
4.1.2 CYSTITIS
Learning Activity 4.1.2
Carefully read the case below and answer the following questions:
A 27-year-old woman presents to her primary care physician with a report of
urinating more frequently and pain with urination. She denies blood in her urine,
fevers, chills, flank pain, and vaginal discharge. The nurse reports the cloudy
urine with a strong bad odor, after some days of hospitalization patient complains
the fever, pain or burning sensation while urinating, cramps or pressure in lower
middle abdomen and back, the results of laboratory test show red blood cells in
urine and E.coli. The physician prescribed for her the antibiotics (ciprofloxacin
500mg two times a day during 7 days) and painkillers (ibuprofen 400mg three
times a days for 5 days and buscopan 20mg two times a day for 5 days) and
nurse continued to monitor vital signs and drugs administration.
She reports having experienced similar symptoms a few years ago and that they
went away after a course of antibiotics. The patient has no other past medical
problems. Pertinent history reveals that she has been sexually active without
using condoms.
1. What are the abnormal signs and symptom that the patient was presenting?
2. What is the medical condition was the patient having?
3. What are the possible causes and risk factors of that medical condition as
stipulated in this case?
4. What are the investigations for diagnosing that medical condition?
5. Propose the treatment plan for this patient.6. What are possible complications if the patient is not well treated?
Cystitis is an inflammation of the urinary bladder usually caused by the bladder
infection. Although it is usually able to be treated on an outpatient basis, it is
common type of UTIs that are potential source of ore complex problems requiring
invasive treatment.
Causes of cystitis
Cystitis can be either acute or interstitial:
Bacterial cystitis:
UTIs typically occur when bacteria outside the body enter the urinary tract through
the urethra and begin to multiply. Most cases of cystitis are caused by a type of
Escherichia coli (E. coli) bacteria. Bacterial bladder infections may occur in women
as a result of sexual intercourse. But even sexually inactive girls and women are
susceptible to lower urinary tract infections because the female genital area often
harbors bacteria that can cause cystitis.
Non-infectious cystitis:
Although bacterial infections are the most common cause of cystitis, a number
of noninfectious factors also may cause the bladder to become inflamed. The
causes include urologic instrumentation (e.g., cystoscopy, catheterization), faecal
contamination, prostatitis, or benign prostatic hyperplasia, indwelling catheters,
pregnancy, and sexual intercourse. Some examples include:
• Interstitial cystitis: The cause of this chronic bladder inflammation, also
called painful bladder syndrome, is unclear. Most cases are diagnosed in
women. The condition can be difficult to diagnose and treat.
• Drug-induced cystitis: Certain medications, particularly the chemotherapy
drugs cyclophosphamide and ifosfamide, can cause inflammation of your
bladder as the broken-down components of the drugs exit your body.
• Radiation cystitis: Radiation treatment of the pelvic area can cause
inflammatory changes in bladder tissue.
• Foreign-body cystitis: Long-term use of a catheter can predispose you
to bacterial infections and to tissue damage, both of which can cause
inflammation.
• Chemical cystitis: Some people may be hypersensitive to chemicals
contained in certain products, such as bubble bath, feminine hygiene sprays
or spermicidal jellies, and may develop an allergic-type reaction within the
bladder, causing inflammation.
• Cystitis associated with other conditions: Cystitis may sometimes occur
as a complication of other disorders, such as diabetes, pregnancy, kidney
stones, an enlarged prostate or spinal cord injuries.
Pathophysiology
The inflammation usually is caused by a bacterial infection. Bacteria can invade
the bladder from an infection in the kidneys, lymphatics, and urethra. Because the
urethra is short in women, ascending infections, or microorganisms from the vagina
or rectum are more common.
The lining of the bladder provides a natural resistance to most bacterial invasions
by preventing an inflammatory reaction from occurring. If bacteria do survive in the
bladder, however, they adhere to the mucosal lining of the bladder and multiply. The
surface of the bladder becomes edematous and reddened, and ulcerations may
develop. When urine contacts these irritated areas, the client experiences pain and
urgency, which is magnified in the presence of even slight bladder distention.
Signs and Symptoms
The symptoms of cystitis include urgency (feeling a pressing need to void although
the bladder is not full), frequency, low back pain, dysuria, perineal and suprapubic
pain, and hematuria, especially at the termination of the stream (terminal hematuria).
If bacteremia is present, the client also may have chills, fever, dark urine, cloudy
or strong smelling. When the disease/infection becomes severe, the patient will
experience some systemic signs and symptoms: nausea, vomiting, loss appetite,
weakness, etc. Chronic cystitis causes similar symptoms, but usually they are less
severe.
Investigations
Microscopic examination of the urine reveals an increase in the number of red
and white blood cells.
Culture and sensitivity studies are used to identify the causative microorganism
and appropriate antimicrobial therapy.
If repeated episodes occur, intravenous pyelogram (IVP) or cystoscopy with or
without retrograde pyelograms may be needed to identify the possible cause, such
as chronic prostatitis or a bladder diverticulum (weakening and outpouching of the
bladder wall), which encourages urinary stasis and infection.
Adequate medical diagnosis
The client’s history and symptoms often provide a tentative diagnosis. Culture and
sensitivity studies are used to identify the causative microorganism. Intravenous
pyelogram or cystoscopy may identify the possible cause of cystitis.
Treatment Plan
Medical management includes antimicrobial therapy and correction of contributing
factors. Examples of drugs that may be used include trimethoprim-sulfamethoxazole
(Bactrim) and nitrofurantoin macrocrystals (Macrodantin). Antibiotics like
sulfonamides are drugs commonly used to treat urinary tract infections (UTIs).
Other drugs used are nitrofurantoin macrocrystals (Macrodantin) and nitrofurantoin
(Furadantin), and the acids methenamine mandelate (Mandelamine) and nalidixic
acid (NegGram). An azo dye, phenazopyridine (Pyridium), may be ordered for its
soothing effect on bladder mucosa and often is used in conjunction with urinary
antimicrobial drugs.
Cranberry juice or vitamin C may be recommended to keep the bacteria from
adhering to the wall of the bladder and thus promoting their excretion and enhancing
the effectiveness of drug therapy.
When there is a partial urethral obstruction, no treatment of cystitis is fully effective
until adequate drainage of urine is restored by the removal of the obstruction (see
discussion of urethral strictures).
In some instances, treatment may be prolonged and may need to be repeated.
Advise clients to follow their physicians’ instructions about the medication, such as
drinking extra fluids.
Evolution and complications
When treated promptly and properly, bladder infections rarely lead to complications.
But left untreated, they can become something more serious. Complications may
include:
• Kidney infection: an untreated bladder infection can lead to kidney infection,
also called pyelonephritis. Kidney infections may permanently damage the
kidneys.
• Young children and older adults are at the greatest risk of kidney damage
from bladder infections because their symptoms are often overlooked or
mistaken for other conditions.
• Blood in the urine: with cystitis, the patient may have blood cells in the
urine that can be seen only with a microscope (microscopic hematuria) and
that usually resolves with treatment. If blood cells remain after treatment, the
doctor may recommend a specialist to determine the cause.
• Blood in the urine that the patient can see (gross hematuria) is rare with
typical, bacterial cystitis, but this sign is more common with chemotherapy- or
radiation-induced cystitis
Self-assessment 4.1.2
1. What are all possible causes or risk factors to develop the cystitis?
2. What are the signs and symptoms of cystitis?
3. What are the investigations that should be requested to make the diagnosis
of cystitis?
4. What are their rationales?
5. What must be included into the management plan of the cystitis?
6. If not treated, what are the complications of cystitis?
4.1.3 ACUTE AND CHRONIC PYELONEPHRITIS
Learning Activity 4.1.3
Carefully read the case below and answer the following questions:
S.U. a 38-yr-old woman came at the accident and emergency of Kibungo DH
for a history of painful, frequent urination with passage of small volumes of urine
for 3 days. Had intermittent fever, chills, and back pain during 3 days. She was
frightened when she saw blood in her urine and reports this is her third attack of
painful urination and back pain in 4 months. She is anxious because her father
died of kidney cancer and remembers having many UTIs as a child. She has
had four pregnancies with difficult vaginal deliveries. She complains of bilateral
flank pain and abdominal tenderness to palpation, and severe pain (pain score
of 9/10) while palpating the costovertebral area. Her vital signs are BP: 134/67
mmHg, Pulse: 78 beats/min, respiratory rate of 24 cycles/min, temperature of
38° C. The urinalysis revealed pyuria, hematuria and the presence of white blood
cells in the urine. Urine and blood cultures were still pending and treating team
decided to hospitalize her, gave her the IV fluids (Normal saline 2liters/24hours),
ciprofloxacin tablets 500mg BID for 7 days, and IV paracetamol 100mg as
needed.
1. What are the abnormal signs and symptoms the patient was presenting?
2. What are the risk factors that predispose S.U to develop her medical
condition?
3. What is the medical condition that S.U is presenting?
4. List all investigations that have been ordered to the patient, and all other
helpful investigations based on her medical condition.
5. What was included into her treatment plan?
6. What do you think could be the complications if her medical condition is
poorly managed?
The most common urologic disorders are infectious and inflammatory conditions.
Those that affect the kidneys are extremely dangerous because damage to the
nephrons can result in permanent renal dysfunction and the consequences can
lead to acute or chronic renal failure.
Pyelonephritis is an acute or chronic bacterial infection of the kidney (which
involves one or both kidneys) and the lining of the collecting system (kidney pelvis).
Acute pyelonephritis presents with moderate to severe symptoms that usually
last 1 to 2 weeks. If the treatment of acute pyelonephritis is unsuccessful and the
infection recurs, the chronic pyelonephritis occurs.
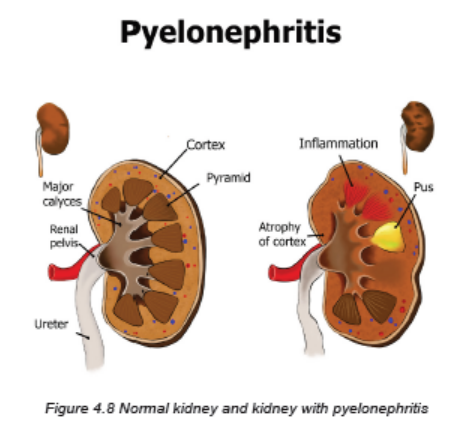
A. ACUTE PYELONEPHRITIS
In acute pyelonephritis, the inflammation causes the kidneys to grossly enlarge.
The cortex and medulla develop multiple abscesses. The renal calyces and pelves
also can become involved. Resolution of the inflammation results in fibrosis and
scarring.
Causes and Risk Factors
Pyelonephritis usually begins with colonization and infection of the lower urinary
tract via the ascending urethral route. Acute pyelonephritis commonly starts in the
renal medulla and spreads to the adjacent cortex. The common causes are:
• Bacteria normally found in the intestinal tract, such as E. coli or Proteus,
Klebsiella, or Enterobacter species, frequently cause pyelonephritis.
• A preexisting condition like vesicoureteral reflux (retrograde, or backward,
movement of urine from lower to upper urinary tract)
• Dysfunction of the lower urinary tract causing the urinary stasis or urinary
obstruction (e.g., obstruction from benign prostatic hyperplasia, tumors, a
stricture, a urinary calculi or stone).
• Instrumentation of urethra and bladder (Urinary tract catheterization,
cystoscopy, urologic surgery) is also a common cause of pyelonephritis and
urosepsis.
• Another important risk factor for acute pyelonephritis is pregnancy-induced
physiologic changes in the urinary system.
• Women with increased sexual activity, who use the diaphragm or spermicide,
who fails to void after intercourse, history of recent urinary infection.
• Men who perform anal intercourse, who has infection with HIV
• Inability to empty the bladder
• Other existing conditions/comorbidities like diabetes mellitus, other renal
disease (polycystic kidney disease), neurogenic bladder (post stroke, multiple
sclerosis, or spinal cord injury)
Pathophysiology
Infection spread by ascending microorganisms along the ureters, and may be also by
bloodstream. The infection causes the inflammation, and the inflammatory process
affects the pelvis, calyces, medulla and tubules. There is medullary infiltration of
white blood cells with renal inflammation, renal edema and purulent urine. In severe
infection, the abscess may be formed in the medulla and extend into the cortex.
The necrosis of renal papillae may develop.
Signs and Symptoms
The clinical manifestations of acute pyelonephritis are acute onset and vary from
mild fatigue to the sudden onset of chills, fever, vomiting, malaise, flank or groin pain,
and the lower UTIs characteristics that include dysuria, urgency, and frequency.
The patient might also have the cloudy or purulent urine.
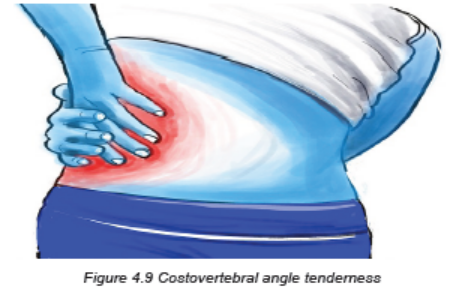
Costovertebral tenderness to percussion (costovertebral angle pain) is typically
present on the affected side. Although the clinical manifestations may subside within
a few days, even without specific therapy, bacteriuria and pyuria usually persist.
Investigations
For investigating the pyelonephritis, the complete history taking and comprehensive
physical examination must be performed first. The most useful investigations are:
• Urinalysis that will indicate pyuria, bacteriuria, and varying degrees of
hematuria. White blood cells casts may be found in the urine indicating
involvement of the renal parenchyma.
• A full blood count ( FBC) shows leucocytosis (increased levels of leukocytes
in the blood)
• Urine cultures must be obtained when pyelonephritis is suspected to detect
the causative agents.
• In patients with more severe illness who are hospitalized, blood cultures
are usually obtained as well.
• Ultrasonography of the urinary system may be performed to identify anatomic
abnormalities, hydronephrosis, renal abscesses, or an obstructing stone.
• Other Imaging investigations include CT scan alone or combined with
Intravenous pyelography, VCUG (a voiding cystourethrogram is a study
used to look at bladder and urethral abnormalities and to determine if you
have ureteral reflux), CT urograms are also used to assess for signs of
infection in the kidney and complications of pyelonephritis such as impaired
renal function, scarring, chronic pyelonephritis, or abscesses.
Adequate Medical diagnosis
The client’s history and symptoms often provide a tentative diagnosis. The physical
examination and most useful investigations such as urinalysis, a full blood count ,
urine culture may contribute to confirm the diagnosis

Treatment Plan
The treatment plan is made basing of severity of signs and symptoms that the
patient is presenting.
Mild Symptoms (Uncomplicated Infection):
• Outpatient management or short hospitalization
• Antibiotics therapy should be for 2 – 3 weeks
• Empirically selected broad-spectrum antibiotics: ampicillin, vancomycin
combined with an aminoglycoside (e.g., tobramycin, gentamicin)
• Switch to sensitivity-guided therapy: trimethoprim/sulfamethoxazole (Bactrim)
when results of urine and blood culture are available
• Fluoroquinolones are helpful too like ciprofloxacin, ofloxacin, norfloxacin,
gatifloxacin
• Adequate fluid intake (oral preferably)
• Nonsteroidal antiinflammatory drugs (NSAIDs) or antipyretic drugs
• Follow-up urine, blood cultures and imaging studies
Severe Symptoms:
• Require Hospitalization
• Antibiotics therapy should be for 2 – 3 weeks
• Parenteral (Intravenous) Antibiotics
• Oral antibiotics (broad spectrum antibiotics, fluoroquinolones, etc) when
patient tolerates oral intake
• Adequate fluid intake (parenteral initially and switch to oral fluids as nausea,
vomiting, and dehydration subside)
• NSAIDs as antipyretic or analgesic drugs to reverse fever and relieve
discomfort
• Follow-up urine, blood culture and imaging studies
Evolution and complications
After the acute phase, healing occurs with deposition of scar tissue and
atrophy of affected tubules. Acute pyelonephritis rarely causes renal failure.
The most common complications of acute pyelonephritis are:
1. Transformation to Chronic pyelonephritis
2. Papillary necrosis due to inflammatory thrombosis of the blood vessels
supplying the renal papilla.
3. Pyonephrosis (filling of the dilated calyces and pelvis by pus due to obstruction
at pelviureteric junction.
4. Perinephric abscess due to spread of the inflammation to the perinephric fat
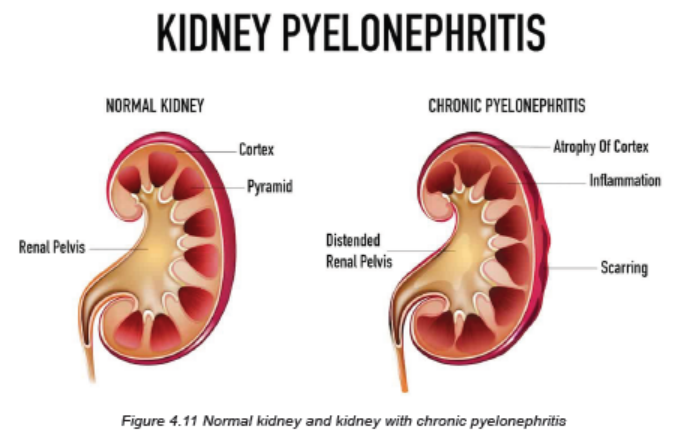
B. CHRONIC PYELONEPHRITIS
This is a persistent or recurrent infection of the kidney, leading to scarring of the
kidney. One or both kidneys may be involved. In chronic pyelonephritis, the kidneys
become small, atrophic, and shrunken and lose function due to fibrosis (scarring).
Chronic pyelonephritis is usually the result of recurring infections involving the upper
urinary tract. However, it may also occur in the absence of an existing infection,
recent infection, or history of UTIs.
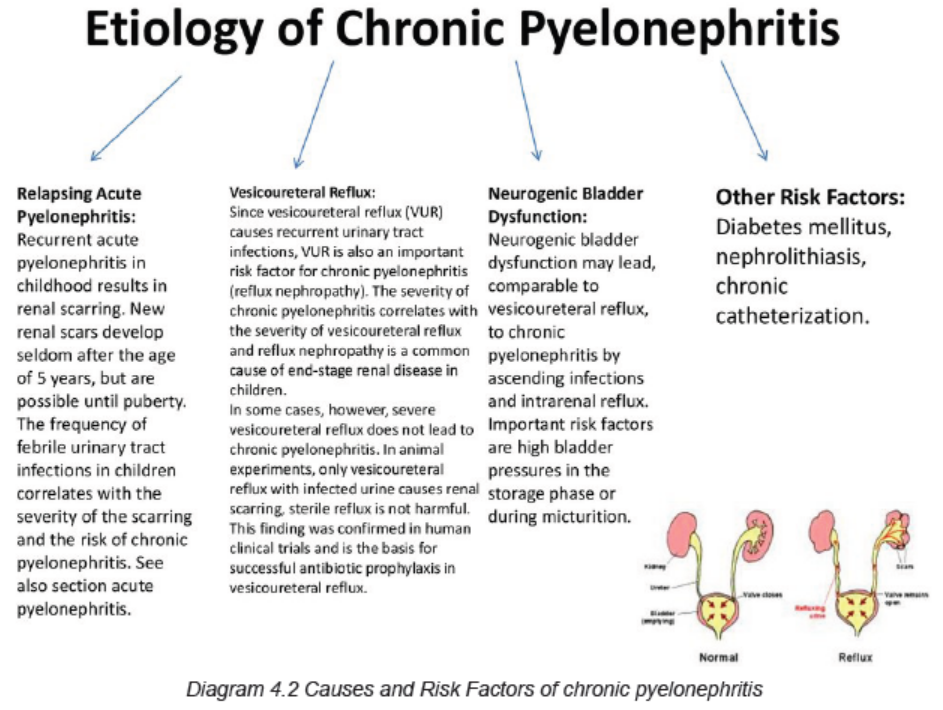
Causes and Risk factors
The most common causes of chronic pyelonephritis are:
• Recurrent episodes of acute pyelonephritis
• Chronic obstruction (e.g., strictures and stones)
• Reflux disorders that allow urine to flow backward up the ureters
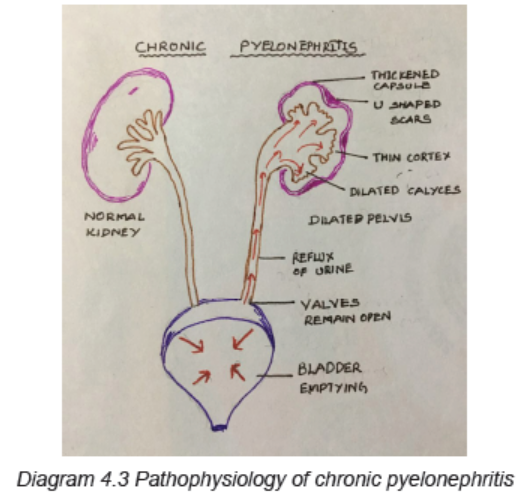
Pathophysiology
There is a process of progressive inflammation, altered renal pelvis and calyces,
destruction of the tubules, atrophy or dilation, and diffuse scarring; and finally
impaired urine- concentrating ability, leading to chronic renal failure.
Signs and Symptoms
Repeated acute pyelonephritis leads to chronic pyelonephritis. In exacerbation,
the symptoms are similar to acute pyelonephritis. The general clinical signs and
symptoms are:
– General body weakness, fatigability, headache
– Anorexia/poor appetite
– Polyuria and frequency urine
– Excessive thirst
– Weight loss
– Pain and/or unpleasant sensation at costovertebral region
– Flank pain
– Cloudy urine
– Progressive scarring leads to Renal failure
– Systemic signs: elevated BP (Hypertension), vomiting, diarrhea.
Investigations
Investigations of chronic pyelonephritis are similar to the ones of acute pyelonephritis.
The complete history taking and comprehensive physical examination must be
performed first. Radiologic imaging and a biopsy, rather than clinical features are
used to confirm the diagnosis of chronic pyelonephritis.
The level of renal function in chronic pyelonephritis depends on whether one or
both kidneys are affected, the extent of scarring, and the presence of coexisting
infection.
The most useful investigations are:
• Urinalysis that will indicate pyuria, bacteriuria, and varying degrees of
hematuria. White blood cells casts may be found in the urine indicating
involvement of the renal parenchyma.
• A full blood count ( FBC) shows leucocytosis (increased levels of leukocytes
in the blood)
• Urine cultures must be obtained when pyelonephritis is suspected to detect
the causative agents.
• In patients with more severe illness who are hospitalized, blood cultures
are usually obtained as well.
• Ultrasonography of the urinary system may be performed to identify anatomic
abnormalities, hydronephrosis, renal abscesses, or an obstructing stone.
• Other Imaging investigations include CT scan alone or combined with
Intravenous pyelography, VCUG (a voiding cystourethrogram is a study
used to look at bladder and urethral abnormalities and to determine if you
have ureteral reflux), CT urograms are also used to assess for signs of
infection in the kidney and complications of pyelonephritis such as impaired
renal function, scarring, chronic pyelonephritis, or abscesses.
• Imaging studies reveal a small, fibrotic kidney. The collecting system may be
small or hydronephrotic.
• Renal Biopsy results indicate the loss of functioning nephrons, infiltration of
the parenchyma with inflammatory cells, and fibrosis.
Adequate medical diagnosis
The client` history and symptoms often provide a tentative diagnosis. A comprehensive
physical examination must be performed . The most useful investigations such as
urinalysis, a full blood count, urine culture and ultrasonography may contribute to
confirm the diagnosis.
Treatment plan
The treatment should focus on treating the causes (Obstruction must be relieved)
and treat all risk factors (vesicoureteral reflux, neurogenic bladder dysfunction,
arterial hypertension) and should also include the prolonged Antibiotics for 4-6
weeks.
The patient will require hospitalization, Parenteral (Intravenous) Antibiotics but Oral
antibiotics (broad spectrum antibiotics, fluoroquinolones, etc.) can be preferred
when patient tolerates oral intake. Patient must also receive the adequate fluid intake
(parenteral initially and switch to oral fluids as nausea, vomiting, and dehydration
subside) and NSAIDs as antipyretic or analgesic drugs to reverse fever and relieve
discomfort.
Surgical management (Nephrectomy) is indicated when there is unilateral
manifestation of chronic pyelonephritis with organ dysfunction to control current
UTI or arterial hypertension.
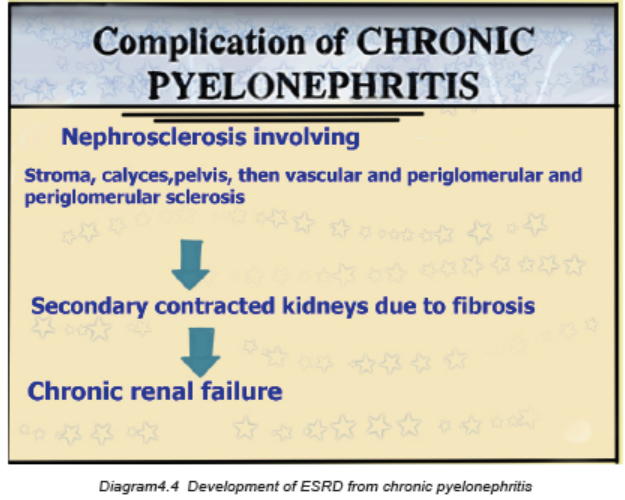
Evolution and Complications
Chronic pyelonephritis often progresses to end-stage kidney (renal) disease
(ESRD) even if the underlying infection is successfully treated.
The most common complications of chronic pyelonephritis are:
• Anemia
• Fluid overload
• Bacteremia
• Hypertension
• Renal stones
• End stage renal disease
Self-assessment 4.1.3
1. What is the most common cause of acute pyelonephritis resulting from an
ascending infection from the lower urinary tract?
a) The kidney is scarred and fibrotic.
b) The organism is resistant to antibiotics.
c) There is a preexisting abnormality of the urinary tract.
d) The patient does not take all of the antibiotics for treatment of a UTI.
2. Which characteristic is more likely with acute pyelonephritis than with a
lower UTI?
a) Fever
b) Dysuria
c) Urgency
d) Frequency
3. Which test is required for a diagnosis of pyelonephritis?
a) Renal biopsy
b) Blood culture
c) Intravenous pyelogram (IVP)
d) Urine for culture and sensitivity
4. Referring to their causes, differentiate the acute and chronic pyelonephritis
5. What are the investigations and their rationale requested for pyelonephritis?
6. What are the treatment modalities are available for severe form of acute
pyelonephritis?
7. What are the most clinical signs and symptoms that determine the
pyelonephritis?
8. What are the treatment options for chronic pyelonephritis?
9. Referring to RAA system, describe how the pyelonephritis can cause the
hypertension
10. What are the complications of chronic pyelonephritis?
11. Describe how the pyelonephritis can lead to renal failure.
4.1.4 ACUTE AND CHRONIC PROSTATITIS
Learning Activity 4.1.4
Carefully read the case below and answer the following questions:
A 54-year-old man experiences a brief period of dysuria accompanied by some
frequency and urgency. These symptoms occurred after a couple of days where
he didn’t seek medical treatment. Three days later, he suddenly developed fever
(39oC), chills, and worsening, irritating dysuria. Because the fever persisted, he
went to see his physician. Except for the fever, his vital signs were normal. Upon
physical examination, he is found to have extreme tenderness in his prostate
by digital rectal examination. The prostate is palpably tense. He does not have
any noticeable costovertebral angle tenderness and no other notable physical
abnormalities. He says that he has not had any previous incidents that producedsymptoms like the ones he has been experiencing over the past few days.
He was advised to drink plenty of much water, prescribed ciprofloxacine 500mg
BID for 7 days, paracetamol 500mg TDS for 5 days, requested the abdominal
ultrasound and the urine culture that results were still pending.
1. What are abnormal signs and symptoms was the patient having?
2. What is the medical diagnosis is the patient presenting?
3. What are different risk factors to the development of that medical condition?
4. What are all relevant investigations are helpful in confirming that diagnosis?
5. What is the treatment plan of that medical condition?
6. What might be the complications if poorly treated?
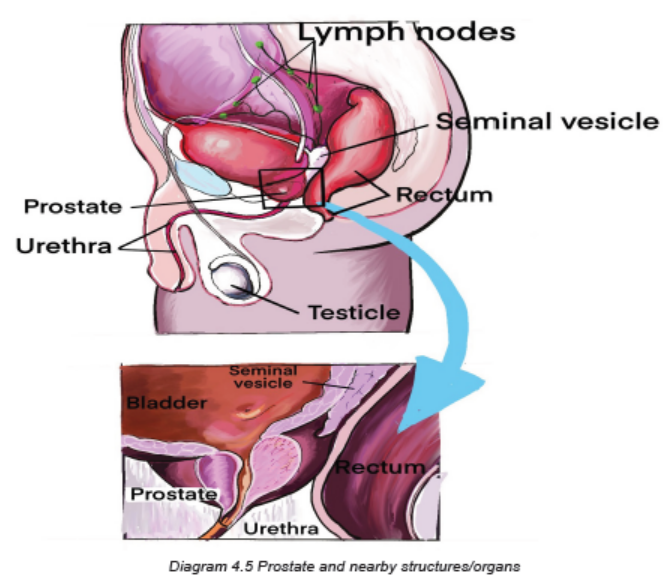
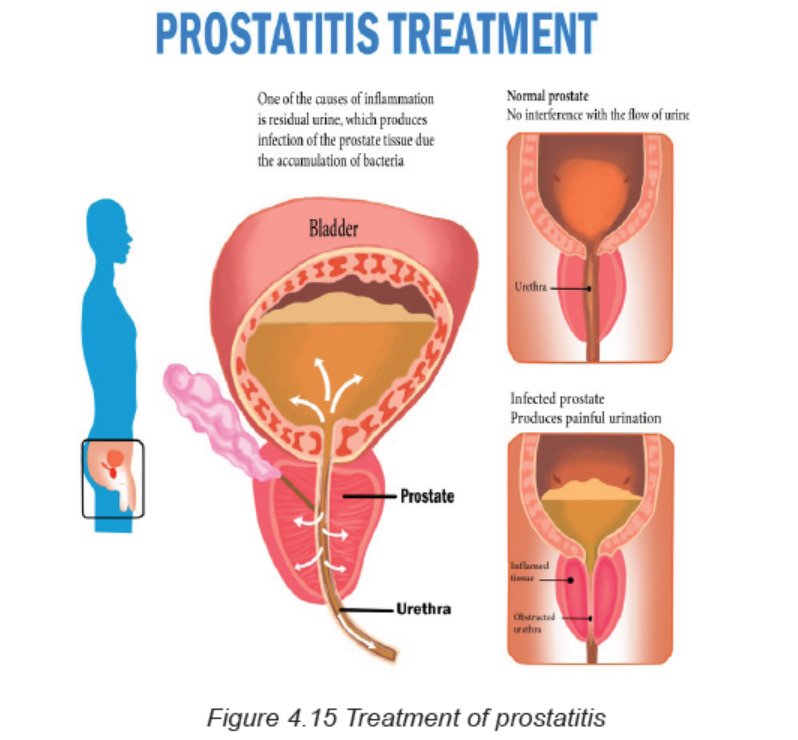
The term prostatitis has been used for various inflammatory conditions affecting
the prostate, including acute and chronic infections with specific bacteria and, more
commonly, instances in which signs and symptoms of prostatic inflammation are
present but no specific organisms can be detected.
Classification of prostatitis
Prostatitis is classified as:
– Acute bacterial prostatitis
– Chronic bacterial prostatitis
– Nonbacterial prostatitis (Chronic pelvic pain syndrome).
A. ACUTE PROSTATITIS
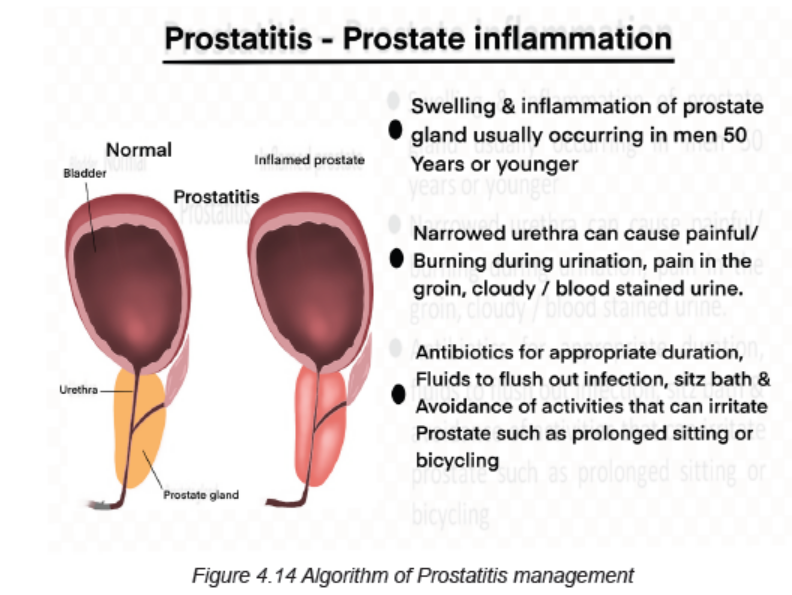
Acute prostatitis is a sudden inflammation of the prostate gland. It is a rare type of
prostatitis, which is a common prostate problem. When the prostate gland becomes
inflamed, symptoms may be similar to those of an acute UTI. Acute prostatitis
is often caused by a type of bacteria that causes UTIs and sexually transmitted
infections.
Causes and Risk factors
Inflammation can result from bacteria entering the prostate via the blood or an
infection in the area. It can also be caused by urethral stricture and prostatic
hyperplasia. A medical procedure may also lead to bacteria entering the prostate.
Underlying causes of acute prostatitis might also be a blocked urethra or suppressed
immune system. The most common causes of prostatitis are bacteria, fungi or
mycoplasma:
– Escherichia coli
– Enterobacter
– Klebsiella
– Pseudomonas
– Chlamydia trachomatis
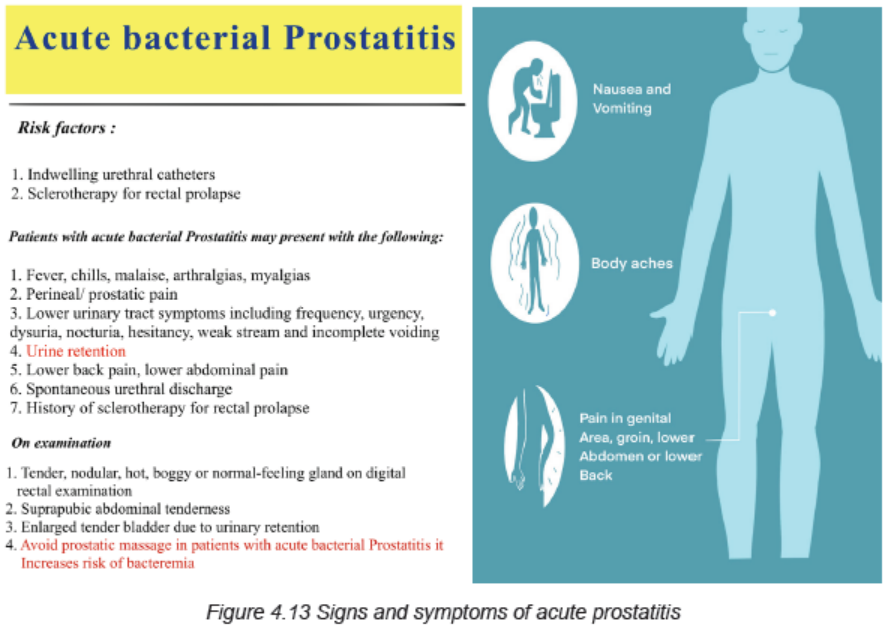
The risk factors for acute bacterial prostatitis (all allow bacterial colonization) are
intra-prostatic ductal reflux, phimosis and redundant foreskin, unprotected anal
intercourse, urinary tract infections, acute epididymitis, indwelling foley catheter,
transurethral surgery, altered prostatic secretions, recent transrectal ultrasoundguided
prostate needle biopsy, immunosuppression (patients with underlying
immunosuppression, may be more likely to have prostatic involvement with
organisms other than the usual bacteria that tend to cause urinary tract infection),
etc.
Pathophysiology
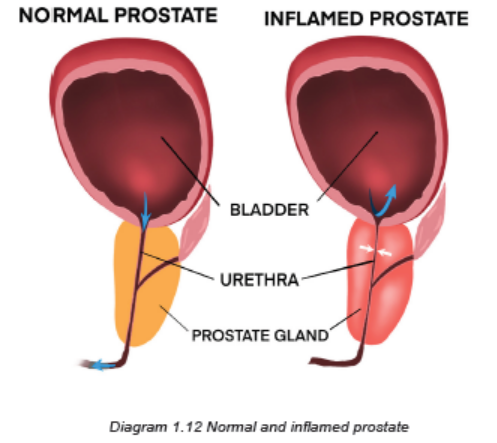
The infection stimulates an inflammatory response in which the prostate becomes
enlarged, tender, firm, or boggy (too wet). Acute inflammatory prostatic edema may
cause urinary obstruction with dysuria. The onset of the illness may be acute, or
follow catheterization or cystoscopy.
An inflammation of the prostate gland and surrounding tissue due to an infection
can be acute or chronic. Some physiological factors that contribute to development
of prostatitis are altered prostate secretory functions, decreased zinc, decreased
prostatic antibacterial factor and altered prostatic PH. The prostatitis can also be
due to catheters, urethral instrumentation and transurethral prostatectomy.
Signs and symptoms
Patient with acute prostatitis present with low back pain, perineal pain, high fever
up to 40o C, chills, dysuria, inability to empty the bladder, nocturia, urinary retention,
systemic signs and symptoms of infection (myalgia, arthralgia, fatigue/malaise),
prostatic pain especially when an individual is in upright position, symptoms can
include pain (in the perineum, lower abdomen, testicles, penis, and with ejaculation),
bladder irritation, bladder outlet obstruction, and sometimes blood in the semen,
sexual dysfunction may accompany chronic bacterial prostatitis.
Investigations
The ways of diagnosing the acute prostatitis include:
• Complete history taking
• Complete physical exam that include the Digital rectal examination: there
may be prostatic hypertrophy, tenderness, edema, and nodularity. However,
the prostate exam is frequently normal.
• FBC, Urea and creatinine, PSA (prostatic specific antigen): Laboratory
findings that suggest inflammation or infection like elevated serum
leukocytes or inflammatory markers may be absent. Usually there is an
elevated prostatic specific antigen (>4 ng/mL).
• Urinalysis: Gram stain, culture, bacteriuria (WBC >105 )
• The diagnostic standard for bacterial prostatitis is the finding of bacteria at
higher levels in prostatic fluid compared with urethral and bladder specimens.
It is better to obtaining prostatic specimens for analysis and culture to
confirm the prostate as the site of infection.
• Abdominal ultrasound can also be helpful (demonstrated the prostate
increased in size).
Adequate medical diagnosis
Treatment plan
The treatment plan for acute prostatitis includes:
Antibiotics: prolonged antibiotic therapy (for at least six weeks) with an agent that
has good penetration into the prostatic tissue is generally necessary for treatment
of bacterial prostatitis. A fluoroquinolone is generally the drug of choice for both
initial and recurrent episodes. Trimethoprim-sulfamethoxazole is an adequate
alternative regimen. Other agents with good penetration into prostatic fluid and
tissue include tetracyclines and macrolides. In mild case: Oral antibiotics up to 6
weeks, in severe cases: IV Ampicilline+ Gentamycine for 7 days, then 4-6 weeks
oral antibiotics.
Analgesics and Antipyretics
Bed rest and adequate hydration
Addressing urinary obstruction — Symptoms of difficulty urination, a sensation of
incomplete emptying, or post-void dribbling should trigger further investigations.
Alpha-blockers (prazocin, terazocin, etc) may be used to relax the bladder muscles
and reduce discomfort
Most cases of acute prostatitis will clear up with antibiotic treatment. Some
severe cases of infection may require a hospitalisation, and mainly due to failed
outpatients management, inability to tolerate oral intake, evidence of resistance risk
factors (recent fluoroquinolones use, recent transurethral or transrectal prostatic
manipulation), systemically ill patient or septicaemia, urinary retention, etc
In addition to medical interventions, a patient may try to alleviate symptoms with
home remedies like taking warm showers or baths, avoiding activities that put
pressure on the prostate such as bicycling, sitting on a cushion, avoiding alcohol,
reducing or avoiding consumption of spicy foods, drinking plenty of fluids that do
not contain caffeine. There are a variety of lifestyle changes that may reduce the
risks of developing chronic or recurring prostatitis: reducing stress, using protection
during sexual activity, ejaculating at least once a week, avoiding processed foods,
eating a healthful diet, protecting against pelvic trauma, maintaining a healthy
weight.
Evolution and Complications
Most cases of acute prostatitis will clear up with antibiotic treatment. Acute prostatitis
may cause a blockage of the urethra. When this occurs, a person will experience
pain and discomfort in the bladder. If left untreated, a blocked bladder can lead
to permanent kidney damage. Other complications may include residual chronic
prostatitis, inflammation of the epididymis or epididymoorchitis (a coiled tube at
the back of the testicles), bacteremia (a bacterial infection of the blood), prostatic
abscess (a pus-filled pocket in the prostate), semen abnormalities, seminal
vesiculitis, infertility.
B. CHRONIC BACTERIAL PROSTATITIS
The chronic bacterial Prostatitis is characterized by recurrent urinary tract symptoms
and persistence of pathologic bacteria (usually Gram negative) in urine or prostatic
fluid. It is similar to chronic pelvic pain syndrome (CPPS). Chronic prostatitis is the
inflammation or infection of the prostate that lasts at least 3 months.
Causes and risk factors
Chronic bacterial prostatitis is caused by bacteria getting to the prostate through the
urethra. This infection can be caused by an infection originating from the bladder or
contaminated urinary catheter. Some bacterial infections contribute to the formation
of prostate stones that are not expelled during urination. Prostate stones are about
the size of a poppy seed and are not always detectable during physical exam.
Infected prostate stones are a common cause of recurring UTIs and make curing
chronic bacterial prostatitis very difficult.
Pathophysiology
The infection stimulates an inflammatory response in which the prostate becomes
enlarged, tender, firm, or boggy (too wet). Acute inflammatory prostatic edema may
cause urinary obstruction with dysuria.
Signs and symptoms
The signs and symptoms of chronic prostatitis and CPPS are very similar. They
usually start out mild and build in intensity over time. Those signs and symptoms
include: a constant urge to urinate, burning pain when urinating, difficulty starting
urination followed by uneven flow, blood in urine, feeling as if the bladder isn’t fully
emptied after urination, painful ejaculation, pain in following locations: lower back,
lower abdomen, above pubic area, between the testicles and anus, etc. It may also
be accompanied by fever and chills.
Symptoms may be similar to those of prostatic cancer, urinary retention, bladder
stones and those from an acute bladder infection: urgency, frequency, dysuria,
perineal discomfort, low back pain, myalgia, arthralgia and sexual dysfunction.
The prostate may only slightly enlarged or wet, but yet fibrosis because with
repeated infections can cause it to be rigid and irregular in shape.
Investigations
– Complete history taking
– Complete physical exam that include the Digital rectal examination: there
may be prostatic hypertrophy, tenderness, edema, and nodularity. However,
the prostate exam is frequently normal.
– FBC, Urea and creatinine, PSA (prostatic specific antigen): Laboratory
findings that suggest inflammation or infection like elevated serum leukocytes
or inflammatory markers may be absent. Usually there is an elevated prostatic
specific antigen (>4 ng/mL).
– Urinalysis: Gram stain, culture, bacteriuria (WBC >105 )
– The diagnostic standard for bacterial prostatitis is the finding of bacteria at
higher levels in prostatic fluid compared with urethral and bladder specimens.
It is better to obtaining prostatic specimens for analysis and culture to confirm
the prostate as the site of infection.
– Abdominal/pelvic imaging (CT scan, MRI, ultrasound)
– Prostatic massage to express secretions: culture, Gram-stain
– Pelvic X-ray may show prostatic calculi
– Biopsy guided by transurethral or transrectal ultrasonography
Adequate medical diagnosis
Chronic prostatitis is a pelvic condition that needs to be distinguished from other
forms of prostatitis, such as acute and chronic bacterial prostatitis. It is characterized
by pelvic or perineal pain lasting longer than 3 months without evidence of urinary
tract infection. Symptoms include pain that may radiate to the back and perineum
causing discomfort while sitting, dysuria, frequency, urgency, arthralgia, myalgia,
unexplained fatigue, abdominal pain, and burning sensation in the penis may be
present. Post-ejaculatory pain mediated by nerves and muscles is a hallmark of
the condition. Some patients report low libido, sexual dysfunction, and erectile
difficulties. The symptoms of chronic prostatitis appear to result from interplay
between psychological factors and dysfunction in the immune, neurological,
and endocrine systems. The prognosis is good with use of multimodal treatment
including antibiotics use, psychotherapy, pelvic nerve trigger point release, anxiety
control, and chronic pain therapy
Treatment plan
Antibiotics: prolonged antibiotic therapy (for 12 weeks) with an agent that has good
penetration into the prostatic tissue is generally necessary for treatment of bacterial
prostatitis. A fluoroquinolone is generally the drug of choice for both initial and
recurrent episodes. Trimethoprim-sulfamethoxazole is an adequate alternative
regimen. Other agents with good penetration into prostatic fluid and tissue include
tetracyclines and macrolides. In mild case: Oral antibiotics, In severe cases: IV
antibiotics.
Analgesics and Antipyretics (Nonsteroidal anti-inflammatory drugs or corticosteroids)
Bed rest, adequate hydration.
Addressing urinary obstruction — Symptoms of difficulty urination, a sensation of
incomplete emptying, or post-void dribbling should trigger further investigations.
Alpha-blockers may be used to relax the bladder muscles and reduce discomfort
Patients may require the hospitalisation
Treat the underlying cause (e.g.: surgical removal of prostatic stone through
transurethral prostatectomy, surgery to remove scar tissue in the urethra, which
can help urination difficulties)
Muscle relaxants to relieve spasm of the pelvic muscles
Therapy to help with psychological stress and anxiety
Evolution and complications
The prongosis is good with use of multimodal treatment including antibiotics use,
psychotherapy, pelvic nerve trigger point release, anxiety control, and chronic pain
therapy. When chronic prostatitis is caused by a bacterial infection, it can be treated
with antibiotics. When the cause is unknown, treatment of the symptoms may be
the best course of action. If left untreated, a blocked bladder can lead to permanent
kidney damage, inflammation of the epididymis or epididymoorchitis, bacteremia,
prostatic abscess, semen abnormalities, seminal vesiculitis, infertility.
Self-assessment 4.1.4
1. Differentiate the acute and chronic prostatitis
2. Describe briefly the pathogenesis of bacterial prostatitis.
3. What are the signs and symptoms of acute prostatitis?
4. What are the causes of prostatitis?
5. List the risk factors of acute prostatitis
6. Enumerate all investigations needed to diagnose prostatitis and their
rationale.
7. What are the treatment modalities of acute prostatitis?
8. Explain when is surgical interventions needed during the management of
chronic prostatitis.
9. List some complications of acute prostatitis.
10. What is the standard investigation of prostatitis?
11. What are the indications of hospitalisation to a patient with acute prostatitis?
4.2. SEXUAL TRANSMISSIBLE DISEASES (STDs)
Introductory activity 4.2
Observe the picture below and answer the questions that follow.

Figure 4.2.1Relationship between girl and boy
1. What do you see on the picture?
2. What do you think could be the consequences of their act?
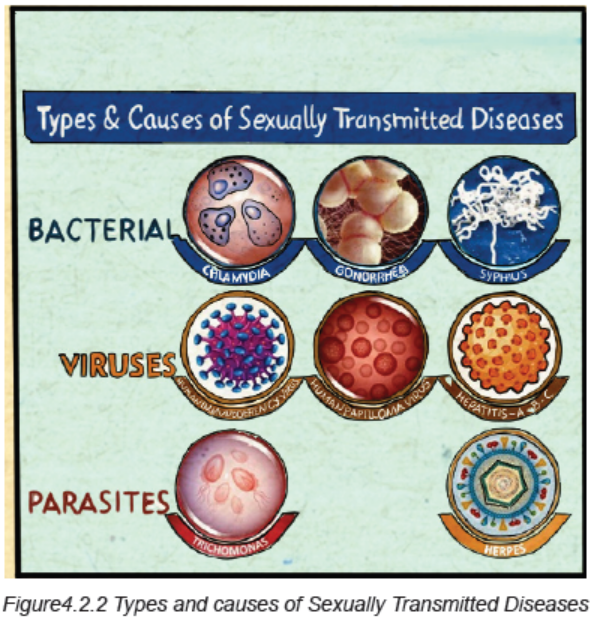
Sexually transmitted infections (STIs), also known as Sexually Transmitted Diseases
(STDs), are caused by bacteria, viruses or parasites that are transmitted through
unprotected sex (vaginal, anal, or oral) and skin to skin genital contact. The most
common bacterial infections include chlamydia, gonorrhoea, and syphilis. The viral
infections include genital herpes, Hepatitis B, Human Papillomavirus (HPV) and
Human Immunodeficiency Virus (HIV). Parasites are responsible for trichomoniasis.
4.2.1 CHLAMYDIA
Learning Activity 4.2.1
Ms A.E, a 20 year old female was worried because she had vaginal discharge
and irritation for three days. The discharge was slight, clear, watery, and nonoffensive,
and she had no abnormal vaginal bleeding. Ms A.E had changed
her sexual partner two months previously. Soon after this she had contracted
genital thrush, which responded to topical clotrimazole. She uses a combined
contraceptive pill and does not use condoms. Ms A.E has no other sexual
partners, and thinks it unlikely her partner has. During the physical examination,
the abnormal finding at vaginal examination was that Ms A.E’s cervix bled
easily when swabbed. A vaginal swab was taken for laboratory examination.
Ms A.E was prescribed doxycycline 200 mg two times a day for seven days and
metronidazole 400 mg three times daily for seven days and sent back home and
waited for results.
A few days later the laboratory reported that chlamydia had been detected. Ms
A.E was called to come back at health facility to be communicated the results.
She was upset to be told that she might have had a sexually transmitted disease
and was unpleasant to go together with her partner.
1. What were the abnormal signs and symptoms was the patient presenting?
2. Basing on those signs and symptoms, what do you think was the medical
diagnosis?
3. What were the risk factors that predisposed her to develop that condition?
4. What were the investigations requested to guide in the confirmation of that
diagnosis?
5. What were the treatment options were available towards that diagnosis?
6. If not well managed, what will be the complications?
Chlamydia is a sexually transmitted disease caused by a bacterium named
Chlamydia trachomatis.
Risk factors
A person is at risk of getting infected of STIs if he/she drinks alcohol (it may be difficult
to convince a drunken partner to use a condom or use one condom correctly). If the
partner uses drugs, it may also make it easier for them to pressure a person into
engaging in unsafe sexual behaviours. Having one STI frequently is a risk to getting
more infections. If the skin is swollen, or scorched, it is easy for another pathogen
to cause infection.
Pathophysiology
Disease pathogenesis due to Chlamydia trachomatis is a complicated process that
involves: (1) exposure to the organism and infectivity; (2) survival within the host
cell; (3) virulence associated with specific strain types; (4) innate and acquired
immunity, and (5) host genetic susceptibility to infection and disease.
Most female and male infections are asymptomatic, which provides an ongoing
opportunity for silent transmission and the development of disease. In addition,
repeat and persistent infections are common among at risk adolescent and young
adult populations. Even with appropriate detection, there is increasing evidence
for antibiotic resistance to the common drugs used to treat Chlamydia trachomatis.
Consequently, the inability to adequately prevent, diagnose, treat, and eradicate
infection provides the opportunity for pathogenicity and disease.
Chlamydia are intracellular bacterial pathogens, which means they are unable to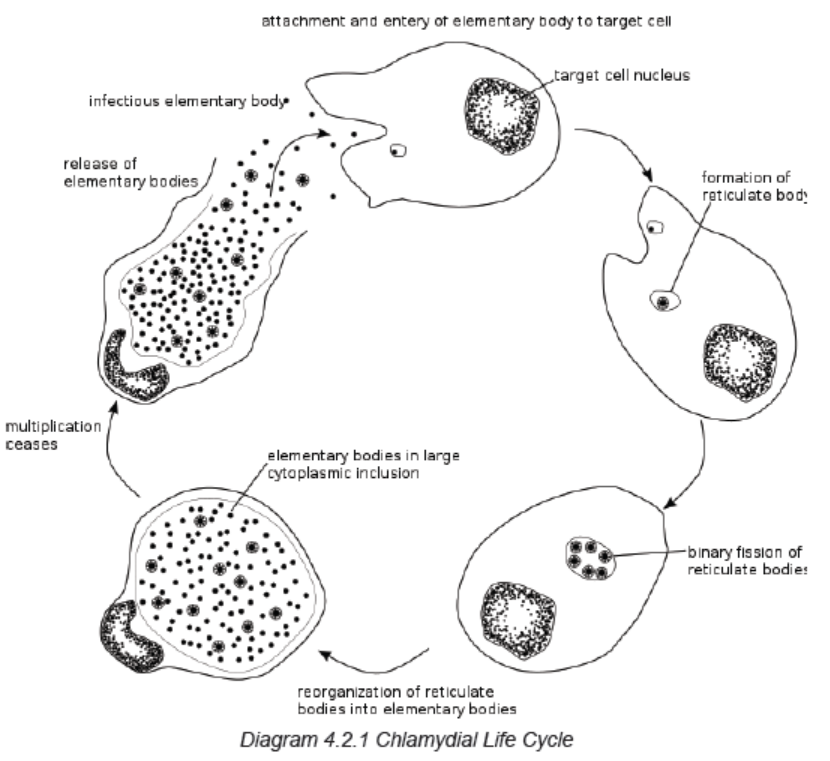
replicate outside of a host cell. However, to disseminate effectively, these pathogens
have evolved a distinct biphasic life cycle wherein they alternate between twofunctionally and morphologically distinct forms.
The elementary body (EB) is infectious, but metabolically inert (much like a spore),
and can survive for limited amounts of time in the extracellular milieu. Once the
EB attaches to a susceptible host cell, it mediates its own internalization through
pathogen-specified mechanisms (via type III secretion system) that allow for therecruitment of actin with subsequent engulfment of the bacterium.
The internalized EB, within a membrane-bound compartment, immediately
begins differentiation into the reticulate body (RB). RBs are metabolically active
but non-infectious; in many regards, they resemble normal replicating bacteria.
The intracellular bacteria rapidly modify its membrane-bound compartment into
the so-called chlamydial inclusion so as to prevent phagosome-lysosome fusion.
The inclusion is thought to have no interactions with the endocytic pathway
and apparently inserts itself into the exocytic pathway as it retains the ability tointercept sphingomyelin-containing vesicles.
The mechanism by which the host cell protein is trafficked to the inclusion through
the exocytic pathway is not fully understood. As the RBs replicate, the inclusion
grows as well to accommodate the increasing numbers of organisms. Through
unknown mechanisms, RBs begin a differentiation program back to the infectious
EBs, which are released from the host cell to initiate a new round of infection.
Because of their obligate intracellular nature, Chlamydiae have no tractable genetic
system, unlike E. coli, which makes Chlamydiae and related organisms difficult to
investigate.
Signs and symptoms
Chlamydia is the most common curable bacterial STD. The symptoms may not be
noticed, or they may be vague and nonspecific. Some people experience no health
effects at all. Chlamydia Symptoms are burning or itching of the genitals, discharge
from the penis or vagina, and pain during sex or urination. Those symptoms can
appear within days or weeks. It infects the cervix in women which is the opening to
the uterus or womb and the penile urethra in men. Chlamydia infections can also
develop in the rectum and throat.
Investigations
Screening and diagnosis of chlamydia is relatively simple. Tests include:
A urine tests: a sample of the urine is analyzed in the laboratory for presence of
this infection.
A swab: for women, your doctor takes a swab of the discharge from your cervix
for culture or antigen testing for chlamydia. This can be done during a routine Pap
test/smear. Some women prefer to swab their vaginas themselves, which has been
shown to be as diagnostic as doctor-obtained swabs. For men, the doctor inserts a
slim swab into the end of the penis to get a sample from the urethra. In some cases,
the doctor will swab the anus
Adequate medical diagnosis
In females, Chlamydia trachomatis most commonly affects the cervix. The majority
of infected females are asymptomatic, although some may present with the typical
findings of cervicitis, including vaginal discharge, abnormal vaginal bleeding, and
purulent endocervical discharge on exam.
The most concerning complication of untreated cervical chlamydial infection is
pelvic inflammatory disease, which in turn can lead to infertility, ectopic pregnancy,
or chronic pelvic pain.
In males, C. trachomatis is a common cause of nongonococcal urethritis. The
majority of infected males are asymptomatic. When present, symptoms include
a mucoid or watery urethral discharge and dysuria. C. trachomatis is a frequent
cause of acute epididymitis in males younger than 35 years of age and may be an
etiology in some cases of chronic prostatitis.
The diagnostic test of choice for chlamydial infection of the genitourinary tract is
nucleic acid amplification testing (NAAT) of vaginal swabs for females or urine for
males. NAAT should also be used on rectal swabs to diagnose chlamydial infection.
If non-NAAT-based testing is used for diagnosis or if adequate follow-up cannot be
insured, patients with signs and symptoms consistent with chlamydia should be
treated empirically before diagnostic test results return.
Treatment plan
Chlamydia can be easily cured with antibiotics. HIV-positive persons with chlamydia
should receive the same treatment as those who are HIV-negative.
Persons with chlamydia should abstain from sexual activity for 7 days after single
dose antibiotics (metronidazole, doxycycline, etc) or until completion of a 7-day
course of antibiotics, to prevent spreading the infection to partners. It is important
to take all the medications prescribed to cure chlamydia. Chlamydial infection in
infants can be treated with antibiotics.
Preventive strategies
It is important to practice proper self-hygiene, for instance, shower regularly, clean
the toilet and bathroom with disinfectants, detergent, and clean water, because one
can easily get an infection from a dirty toilet.
To ensure protection during sexual intercourse, when the client thinks he/she is at
risk of STIs, he/she should go for instant check-up and seek treatment when the
infection is suspected. However, both partners should be treated.
Also, it is urgent to see a doctor immediately if the person is sexually active and may
have been exposed to an STI, or when signs and symptoms of an STI are present.
Evolution and complications
If left untreated, chlamydia can cause permanent damage to the reproductive system
in both males and females. It can cause infertility by blocking the reproductive tract
in men and women. Chlamydia can do a lot of damage to the body in the long run.
Repeated infection with chlamydia is common. Women whose sex partners have
not been appropriately treated are at high risk for re-infection. Having multiple
chlamydial infections increases a woman’s risk of serious reproductive health
complications, including pelvic inflammatory disease and ectopic pregnancy.
Women and men with chlamydia should be retested about three months after
treatment of an initial infection, regardless of whether they believe that their sex
partners were successfully treated. In addition, the infants infected with chlamydia
may develop ophthalmia neonatorum (conjunctivitis) and/or pneumonia.
Self-assessment 4.2.1
1. Name the bacteria that is responsible of chlamydia.
2. What are the signs and symptoms of chlamydia?
3. What are the necessary tests performed to diagnose the infection of
chlamydia?
4. Explain the treatment plan of chlamydia
5. What are the preventive measures?
6. What are the complications of chlamydia in women and men?
4.2.2 SYPHILIS
Learning Activity 4.2.2
Carefully read the case below and answer the following questions:
A 39-year-old woman presented to the emergency department reporting several
weeks of generalized weakness, headache, nausea, and arthralgia. The patient
had unprotected sexual intercourse with a man whom the past 6 months physical
examination revealed a painful ulcerated plaque on the upper lip, a macular rash
with painless lesions (considered to be healing chancres) on the glans, a nonpruritic
hyperkeratotic palmar rash and bilateral submandibular lymphadenopathy.
Results of laboratory testing included a positive reactive syphilis immunoglobulin
G (IgG) enzyme immunoassay and a positive rapid plasma reagin (RPR) test.
The human immunodeficiency virus (HIV) testing was negative, and serologic
testing demonstrated prior immunization to hepatitis B virus. Given the clinical
presentation and laboratory findings, she was treated with benzathine penicillin
G 2.4 million units intramuscularly.
1. Basing on the scenario above, what are the signs and symptoms the
patient was presenting.
2. What is the medical diagnosis is the patient presenting?
3. What are different risk factors and causes of that medical condition?
4. What are different investigations used to diagnose that medical condition?
5. What are different treatment modalities for that medical condition?
6. If not properly treated, what might be some complications?
Syphilis is a chronic bacterial disease that is contracted mainly by infection during
sexual intercourse, but also congenitally by infection of a developing foetus.
Causes and Risk Factors
Syphilis is mainly caused by the bacteria called Treponema pallidum. It is a common
and dangerous infection that is spread from person to person through sexual contact.
It is an infection that is transmitted by direct contact with a syphilitic sore via skin
and mucous membranes such as the vagina, anus, rectum, lips and mouth, most
commonly during oral, anal or vaginal sexual activity. In rare occasions syphilis
spread during kissing.
Treponema pallidum also crosses the placenta, thereby resulting in fetal infection
(Congenital syphilis). This congenital syphilis is generally acquired through
transplacental transmission of spirochetes in the maternal bloodstream or,
occasionally, through direct contact with an infectious lesion during birth
The acquisition of syphilis through transfused blood is very rare because all donors
are screened and T. pallidum cannot survive longer than 24 to 48 hours under blood
bank storage conditions.
While syphilis can affect anyone, there are a number of risk factors (related to
sexual behaviors, while others are associated with characteristics that can place an
entire population at risk) that can increase your likelihood of infection: inconsistent
condom use is the main cause of transmission in all groups, and Men who have sex
with men (due to physiological vulnerabilities such as the fragility of rectal tissues),
multiple sex partners place you at risk simply by providing you a greater opportunity
for exposure, injecting drug use that can impair judgment and increase the risk of
sexual violence or the exchange of sex for drugs, risk attitude and behaviors of
avoidance of STIs screening mainly among those people who have multiple sex
partners.
Pathophysiology
The pathogenesis of Syphilis is explained through different following stages:
• Early local infection: T. pallidum initiates infection when it gains access to
subcutaneous tissues via microscopic abrasions. The spirochete evades
early host immune responses and establishes the initial ulcerative lesion, the
chancre. During the period of early local replication, some organisms establish
infection in regional draining lymph nodes, with subsequent dissemination.
Early syphilis comprises primary and secondary syphilis, which typically occur
within weeks to months after initial infection, as well as early latent syphilis
(asymptomatic infection that was acquired within the previous 12 months).
• Late infection: The prolonged latent period that is characteristic of most
types of late syphilis suggests that immune mechanisms may be involved in
one of two ways. Waning immunity with aging may facilitate recrudescence
of a small number of treponemes that had survived in sequestered sites.
Alternatively, a partially immune hypersensitive host may react to the
presence of treponemes, engendering a chronic inflammatory response. Late
benign syphilis often involving the skin, viscera, or other tissues (eg, bone,
brain, abdominal viscera), are characterized pathologically by the presence
of granulomas, a finding that is consistent with a cellular hypersensitivity
reaction.
If left untreated, syphilis will go through five stages of infection: primary, secondary,
early latent, late latent, and tertiary. The risk and mode of transmission can vary by
the stage:
• During primary syphilis, the disease is passed by coming into contact with
a chancre.
• During secondary syphilis, the disease can be passed by coming into
contact with the secondary rash.
• During early latent syphilis, secondary symptoms can sometimes relapse
and increase the risk of transmission.
• During late latent or tertiary syphilis, the disease is considered noncontagious.
Syphilis cannot be passed via toilet seats, casual contact, or the shared use of
utensils or personal care items. This is because T. pallidum has a fragile shell that
lacks the lipoproteins needed to sustain life outside of the body for very long.
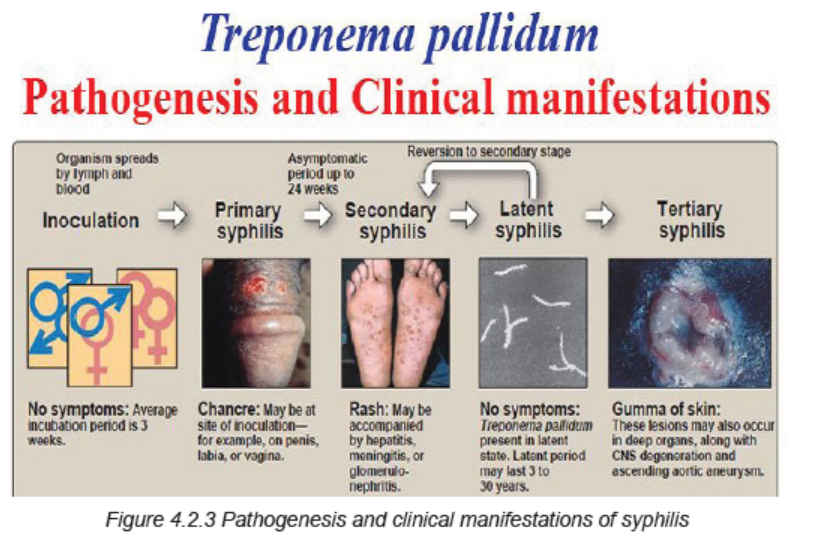
Signs and Symptoms
Patients with syphilis can present with a wide range of symptoms depending on
the stage of disease. Others will have serologic evidence of syphilis based upon
laboratory testing, but will not have symptoms (mainly in latent syphilis).
The clinical manifestations depend upon the stage of disease. The signs and
symptoms of syphilis are related to the stage of the infection. The first involves a
painless sore on the genitals, rectum, or mouth. After that heals, the second stage
will begin and usually produce a rash. After a long period with no symptoms (stage
three), the fourth stage can suddenly develop, causing extensive damage to the
brain, nerves, eyes, or heart.
Primary syphilis (Stage 1): is the first stage of infection. It will typically start with
the appearance of an ulcer called a chancre between 10 to 90 days after the initial
exposure; the average is 21 days. The sore will develop at the point of contact,
most commonly on the cervix, vagina, penis, anus, rectum, or mouth. There may
be one or more lesions. Because the sores are painless, they can be missed if they
are located internally.
Sometimes swollen lymph nodes can develop near the site of the infection. These
are small glands that, among other things, contain white blood cells that help fight
infection called lymphocytes. Without treatment, a chancre will heal in three to six
weeks.
Secondary Syphilis (Stage 2): If left untreated, a primary infection will progress
to secondary syphilis. Symptoms typically appear within two to eight weeks of the
appearance of the chancre. During this stage, a person may experience general
symptoms of illness such as fever, sore throat, fatigue, weight loss, headache,
muscle ache. They may also experience symptoms that may be a bit more telling:
unexplained hair loss (syphilitic alopecia), cracked lesions on the corner of the
mouth (fissure cheilitis), generalized swelling of the lymph nodes, widespread, nonitchy
rash on the palms and soles of the feet, the trunk, or the limbs.
Rarely, secondary syphilis affects the liver, kidneys, bones, and central nervous
system and may produce associated symptoms and complications. The symptoms
of secondary syphilis typically resolve without treatment within weeks or months.
Latent Syphilis (Stage 3): Latent syphilis is the third, so-called “hidden” stage of
infection. It is marked by the relative absence of symptoms and positive blood tests.
This stage is further divided into two stages:
• Early latent syphilis is the period within a year of the initial infection.
Secondary symptoms can sometimes relapse during the early latent phase.
• Late latent syphilis is the period a year after the initial infection. It can last
for years and even decades with no signs of disease.
Tertiary Syphilis (Stage 4): Tertiary syphilis is the most serious stage of this
infection and it is characterized by three major complications:
• Gummatous syphilis causes the formation of soft, tumor-like lesions called
gummas. These noncancerous lesions can cause large ulcerative sores on
the skin and mouth, and erode tissues of the heart, liver, muscles, bones, and
other vital organs. Symptoms typically develop between 3 and 10 years after
a person is first infected.
• Cardiovascular syphilis can cause severe inflammation of the aorta and
swelling and weakening of the aortic wall (aortic aneurysm). It generally
occurs 10 to 30 years after the initial infection.
• Neurosyphilis affects the central nervous system and usually develops
within four to 25 years after the initial infection. While some people will
not develop symptoms, others may experience severe issues such as
General signs and Symptoms of Syphilis include: fever, general ill feeling, joint
pain, loss of appetite, moist warty patches (called condylomata lata) in the genitals
or skin folds, muscle aches, skin rash usually on the palms of the hands and soles
of the feet, sores called mucous patches in or around the mouth, vagina or penis.
Investigations
The diagnosis of syphilis relies on:
Physical examination and clinical manifestations– a doctor or nurse will
ask to examine your genitals (and inside the vagina for women) or other parts
of your body to look for growths or rashes that may be caused by syphilis.
Blood test (Rapid plasma regain: RPR, Venereal Disease Research Laboratory:
VDRL, T. pallidum particle agglutination assay: TPPA, T. pallidum enzyme
immunoassay: TP-EIA, Polymerase chain reaction: PCR): can show whether you
have syphilis or have had it in the past; repeating the test a few weeks later may
be recommended if it’s negative, in case it was too early to give an accurate result.
Swab test – a swab is used to take a small sample of fluid from any sores, so it can
be checked for syphilis.
CSF (cerebro-spinal fluid) testing to detect neurosyphilis is strongly recommended
in patients with tertiary syphilis or with neurological signs or symptoms consistent
with neurosyphilis and in patients without symptoms whose serologic titers do not
decline appropriately after being treated with recommended therapy.
Adequate medical diagnosis
Syphilis is a sexually transmitted infection (STI) caused by a spiral-shaped
bacterium called Treponema pallidum. The infection is typically transmitted through
contact with a sore during a sexual encounter with an infected person, although a
mother can pass to her child during pregnancy. During the initial phase of infection,
the organism disseminates widely, setting the stage for subsequent manifestations.
If untreated, syphilis can have a number of significant late manifestations, including
cardiovascular, gummatous, and neurologic complications. The investigations
should be obtained just before initiating therapy (ideally, on the first day of treatment).
Penicillin is the treatment of choice for all stages of syphilis. Patients should be
monitored clinically and with serologic testing after treatment to ensure they are
responding appropriately to therapy.
Treatment plan
While syphilis infection can still be treated during the tertiary stage, any damage
caused to the heart, kidneys, and other organs may be permanent and can lead
to end-stage organ failure. Treatment is determined by the type and extent of the
damage.
A single intramuscular injection of long acting Benzathine penicillin G (2.4 million
units administered intramuscularly) will cure a person who has primary, secondary
or early latent syphilis.
Three doses of long acting Benzathine penicillin G (2.4 million units administered
intramuscularly) at weekly intervals is recommended for individuals with late
latent syphilis or latent syphilis of unknown duration. Treatment will kill the syphilis
bacterium and prevent further damage, but it will not repair damage already done.
In the treatment of late syphilis by weekly injections, missing a dose of penicillin for
a period of 10-14 days does not require restarting the entire course of injections.
The exception to this is in the case of pregnant women in whom there is no latitude
for missing a dose of penicillin.
Doxycycline is the best alternative for treating early and late latent syphilis. Syphilis
associated with HIV infection does not require any enhanced antimicrobial therapy.
For patients who are allergic to penicillin, alternative agents include tetracyclines,
cephalosporins (ceftriaxone, etc) and macrolides (azithromycin, etc). However, we
only use azithromycin if no other options are available due to concerns of treatment
failure associated with macrolide resistance
Prevention of syphilis: avoid having sex with multiple partners, avoid sharing
sex toys, get screened for sexually transmitted infections and talk to your partners
about their results, syphilis can also be transmitted through shared needles. Avoid
sharing needles if you’re going to use drugs.
Evolution and complications
Early diagnosis and initiation of treatment provides good outcome to patients with
syphilis. At its beginning stage, syphilis will cause sores called chancre in the body.
Chancres are seen mostly in genital areas of the body. Syphilis can also cause rash,
mild fever, fatigue, headache, sore throat, patchy hair loss, and swollen glands
through the body. If left untreated, syphilis can spread to all areas of the body.
If it is untreated, syphilis can cause serious long-term health
problems such as arthritis, brain damage, and blindness.
During the tertiary stage of syphilis, small, rubbery lesions may develop on the
bones, skin, nervous system tissue, and/or arteries of the heart or the brain. Due to
these lesions and other health complications, these individuals are susceptible to
heart attack, paralysis, blindness, stroke, numbness, dementia.
Complications in new-borns if the syphilis is left untreated, the symptoms may
include:
• Liver and spleen enlargement
• Purplish skin spots caused by ruptured capillaries (petechiae)
• Profuse nasal drip with highly infectious mucus discharge (known as syphilitic
“snuffles”)
• Neurosyphilis
• Lung inflammation
• Yellowing of the skin and eyes (jaundice)
• Seizures
By age 2, the child may have characteristic facial or physical deformities and
significant sensory impairment, including:
• Blunted upper front teeth (known as Hutchinson’s teeth)
• A collapse of the bony part of the nose (saddle nose)
• A protruding jawbone and foreshortened upper jaw
• A protruding frontal bone of the skull (frontal bossing)
• Swollen knees
• Bowing of the shin bones (saber shins)
• Inflammation and scarring of the cornea, the clear cover over the front of the
eye (interstitial keratitis)
• Glaucoma, a disease that damage’s the optic nerve and can cause bliness
• Deafness
• Developmental delays
Self-assessment 4.2.2
1. What is the cause of syphilis?
2. Can you list some risk factors to syphilis development?
3. Differentiate different phases/stages of syphilis.
4. Describe briefly the pathogenesis of congenital syphilis.
5. What are different investigations used to diagnose syphilis and their
rationale?
6. What are the preventive strategies for syphilis?
7. What are the treatment options are for a patient with syphilis?
8. What are the complications of syphilis?
4.2.3 GONORRHEA
Learning Activity 4.2.3
Read carefully this below situation and answer the following questions:
Mr. B.E is a 54-year-old male patient who visited RUHENGERI Hospital with
complaints of a purulent white discharge from the penis accompanied by
itching and burning sensation when urinating, painful and the physical examination
(palpation and inspection) revealed swollen testicles on palpation. The history
taking revealed that he is performed unprotected sexual intercourse with a sex
worker met in a hotel two days ago after missing condom. Body temperature
was 36.5 degree Celicius, blood pressure was 110/70 mmHg, pulse rate was
74beats per minute, respiratory rate was 19 breaths per minutes. Mr. B.E was
treated with Doxycycline tablet 100mg two times a day for 7 days associated
with a single dose of Ciprofloxacin 500mg and ibuprofen 400mg two times per
day for 3 days. After taking medication given from health center, the signs and
symptoms persisted despite the adherence of health care provider’s provided
instructions and decided to re-visit the hospital where the pus culture was
done and revealed Neisseria Gonorrhea bacterium, antibiogram showed that
the bacteria can respond to Azithromycin only among others. Other laboratory
investigations were performed and revealed white blood cells (WBC) of 150000.
1. What are abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
4. What was included in the management of this case at different levels of
health care settings he visited?
5. If not treated, what will be the consequences?
Gonorrhea is an infection caused by a sexually transmitted bacterium that
infects both males and females. It can cause infections in the genitals (the urethra,
rectum and throat). In females, gonorrhea can also infect the cervix. This sexually
transmitted disease (STD) or sexual transmission infection (STI) is a very common
infection, especially among young people ages 15-24 years.
Causes and risk factors
Gonorrhea is caused by Neisseria Gonorrhea, any sexually active person can get
gonorrhea through unprotected vaginal, anal, or oral sex. If a patient is sexually
active, must have an honest and open talk with the health care provider and ask
whether he/she should be tested for gonorrhea or other STDs. A sexually active
man who is gay, bisexual, or who has sex with men, should be tested for gonorrhea
every year. A sexually active woman younger than 25 years or an older woman
with risk factors such as new or multiple sex partners, or a sex partner, who has a
sexually transmitted infection, should be tested for gonorrhea every year.
A pregnant woman, who has gonorrhea, can give the infection to the baby during
delivery. This can cause serious health problems for the baby. If the patient is
pregnant, it is important that she talks to the health care provider so that she get
the correct examination, testing, and treatment, as necessary. Treating gonorrhea
as soon as possible will make health complications for your baby less likely.
Pathophysiology
The infection is caused by a bacterium, Neisseria gonorrhoea, which can be
transmitted heterosexually or homosexually. The microorganism invades the
urethra, vagina, rectum, or pharynx, depending on the nature of sexual contact;
it can spread throughout the body. In untreated men, the localized infection may
spread to the prostate, seminal vesicles, and epididymis. Urethral strictures may
develop, requiring periodic dilation of the urethra or, possibly, reconstructive urethral
surgery. In women, the infection may progress upward to the cervix, endometrium,
and fallopian tubes, and symptoms of pelvic inflammatory disease (PID) may
develop. Gonorrhoea also can be transmitted to an infant’s eyes at the time of birth.
Signs and symptoms of gonorrhea
In men, symptoms usually appear 2 to 6 days after infection. Urethritis with a purulent
discharge and pain on urination are the most common signs and symptoms. A small
proportion of men are asymptomatic.
More than half of infected women experience no symptoms. When symptoms do
occur, women have a white or yellow vaginal discharge, intermenstrual bleeding due
to cervicitis, and painful urination. Other symptoms may include burning or frequent
urination, yellowish vaginal discharge, redness and swelling of the genitals, and a
burning or itching of the vaginal area. If untreated, gonorrhea can lead to severe
pelvic infections and even sterility. Even when a woman has symptoms, they are
often mild and can be mistaken for a bladder or vaginal infection. Women with
gonorrhea are at risk of developing serious complications from the infection, even if
they don’t have any symptoms. Symptoms in women can include painful or burning
sensation when urinating; increased vaginal discharge; vaginal bleeding between
periods.
An anal infection is accompanied by painful bowel elimination and a purulent rectal
discharge; the throat is sore when the pharynx is infected. If the microorganism
disseminates (scatters) throughout the body, the client may manifest a skin rash,
fever, and painful joints. Men with gonorrhea may have a yellowish discharge from
the penis accompanied by itching and burning.
Complications in later life can include inflammation of the heart valves, arthritis, and
eye infections. Gonorrhea can also cause eye infections in babies born of infected
mothers.
Some men with gonorrhea may have no symptoms at all. However, men who do
have symptoms may have a burning sensation when urinating; a white, yellow, or
green discharge from the penis; painful or swollen testicles (although this is less
common).
Rectal infections may either cause no symptoms or cause symptoms in both men
and women that may include discharge; anal itching; soreness; bleeding; painful
bowel movements.
The client should be examined by the doctor if he/she notices any of these symptoms
or if his/her partner has an STD or symptoms of an STD, such as an unusual sore,
a smelly discharge, burning when urinating, or bleeding between periods.
Investigations
Swabs from pus or discharge must be sent for analysis and identify the germ
Specimens of drainage from infected tissue are examined microscopically
immediately after they are collected or are inoculated on a culture medium and
incubated to reveal the causative organism.
Other laboratory blood tests (FBC, electrolytes, Renal and liver function tests,
etc) might be helpful to look for other existing conditions.
Medical diagnosis
The medical diagnosis of gonorrhea is based on the clinical manifestation of the
clients as well as the history taking and laboratory findings where possible.
Most of the time, urine can be used to test for gonorrhea. However, if the client has
had oral and/or anal sex, swabs may be used to collect samples from the throat
and/or rectum. In some cases, a swab may be used to collect a sample from a
man’s urethra (urine canal) or a woman’s cervix (opening to the womb).
Treatment plan
The microorganism N. gonorrhoea has become increasingly resistant to penicillin,
tetracycline, and fluoroquinolones.
Therefore, currently CDC (2006) recommendation for treating gonorrhoea is a
single intramuscular dose of a broad-spectrum cephalosporin such as ceftriaxone
(rocephin) or oral dosing with cefixime (suprax). Coinfection with chlamydia
is common; therefore, clients also are given a single dose of oral azithromycin
(zithromax) or oral doxycycline (vibramycin) for 7 to 10 days. Clients with complicated
gonococcal infections, as in PID or disseminated infection, are hospitalized and
treated with IV multiple-drug therapy.
The nursing management and client teaching are similar for those clients other
STDs. However, when a culture is collected from a woman, the vaginal speculum
is moistened with water rather than lubricated, because lubricant may destroy the
gonococci and cause inaccurate test results.
Evolution and complications
Untreated gonorrhoea can cause serious and permanent health problems in both
men and women.
In women, untreated gonorrhoea can cause pelvic inflammatory disease (PID).
Some of the complications of PID are formation of scar tissue that blocks fallopian
tubes external icon, ectopic pregnancy (pregnancy outside the womb external
icon), infertility (inability to get pregnant); long-term pelvic/abdominal pain,
untreated gonorrhea may also increase your chance of getting HIV, the virus that
causes AIDS.
In men, gonorrhoea can cause a painful condition in the tubes attached to the
testicles. In rare cases, this may cause a man to be sterile. Rarely, untreated
gonorrhoea can also spread to your blood or joints. This condition can be life-threatening.
Self-assessment 4.2.3
1. What is gonorrhoea?
2. Describe the causes and triggering factors contributing to the gonorrhoea
development.
3. What are different treatment options for a patient with gonorrhoea?
4. State the preventive measures to be taken to prevent gonorrhoea
5. What are possible investigations to be performed to confirm gonorrhoea?
6. If acute gonorrhoea is not well treated effetely, what could be the
complications?
4.2.4 HIV Infection (Human Immunodeficiency Virus Infection)
Learning Activity 4.2.4
Carefully read the case study below and answer the following questions:
The patient M.V a 24-year-old female who had spent 6 months in Matimba/
Biryogo consulted Muhima hospital for repetitive flu like syndrome, episode
of fevers and generalized body weakness with fatigue. A few weeks ago she
became ill with general body weakness, lymphadenopathy and fever of 39.2 o
C. All laboratory investigations requested (blood smear negative, FBC normal)
were normal and was given paracetamol 1g TDS for 5 days. During the current
visit she was further examined and denied recent sexual contacts, her marital
status is single and lives alone in a house. She reported to be unemployed
and stated that it is very difficult to find living means. Laboratory tests as FBC,
Urea and creatinine, ASAT and ALAT, HIV test and blood culture were ordered
and the health care professionals decided to hospitalise her and put her on IV
paracetamol 100mg TDS for 3 days and IV ceftriaxone 1gr BID for 7 days while
waiting for all results. The results became as normal FBC and a positive ELISA
test for HIV.
As the counselling was not done for HIV prior testing, they proceeded on
counselling and retested for HIV using rapid test to be able to communicate
results. The HIV rapid test became positive too and counselling for possible
initiation of antiretroviral drugs started. During this counselling, she reported
that she get living means from selling her sex and this was also known by her
neighbours. As she was unstable, they waited until to be stable for CD4 control
to decide on initiation of ARV drugs.
1. What was the medical diagnosis the patient was presenting?
2. What were the risks factors that exposed her to develop that medical
condition?
3. What must be considered before initiating the treatment to that condition?
4. What are different investigations are useful to decide on the management
of that medical condition?
5. What are different drugs you know that are used to treat that medical
condition?
6. What are the possible complications related to that medical condition?
HIV (human immunodeficiency virus) is a virus that attacks the immune system,
the body’s natural defence system. Without a strong immune system, the body
has trouble fighting off disease. Both the virus and the infection are called HIV.
White blood cells are an important part of the immune system. HIV infects and
destroys certain white blood cells called CD4+ cells. If too many CD4+ cells are
destroyed, the body can no longer defend itself against infection. The last stage of
HIV infection is AIDS (Acquired Immunodeficiency Syndrome). People with AIDS
have a low number of CD4+ cells and get infections or cancers that rarely occur in
healthy people. These can be deadly. But having HIV doesn’t mean you have AIDS.
Causes and Risk Factors
HIV infection is caused by the human immunodeficiency virus. HIV doesn’t
survive well outside the body, therefore it can’t be spread by casual contact like
kissing or sharing drinking glasses with an infected person. The patient can’t
catch HIV or AIDS by hugging, kissing, dancing or shaking hands with someone
who has the infection. HIV isn’t spread through the air, water or insect bites.
The HIV can be contaminated/transmitted from contact with infected blood, semen,
or vaginal fluids. This can happen in several ways:
By having sex: Infection comes if there is unprotected sexual intercourse being
vaginal, anal or oral with an infected partner whose blood, semen or vaginal
secretions enter your body. The virus can enter the body through mouth sores or
small tears that sometimes develop in the rectum or vagina during sexual activity.
By sharing needles: Sharing contaminated used IV drug materials (needles and
syringes) puts a person at high risk of HIV and other infectious diseases, such
as hepatitis. Health care professionals can get the HIV infections when not being
careful while giving injections or through blood sample collection due to needle
stick injuries while caring for HIV patients.
From blood transfusions: In some cases, the virus may be transmitted through
blood transfusions.
During pregnancy or delivery or through breast-feeding: Infected mothers can
pass the virus on to their babies. Mothers who are HIV-positive and get treatment
for the infection during pregnancy can significantly lower the risk to their babies.
The virus can also be passed from a mother to her baby during pregnancy, birth, or
breastfeeding.
The other greatest risk of HIV/AIDS are:
Have unprotected sex: Anal sex is more risky than is vaginal sex; and the risk
of HIV increases if there are multiple sexual partners.
Have an STI: Many STIs produce open sores on the genitals, and those sores act
as doorways for HIV to enter your body.
Pathophysiology
HIV destroys CD4+ cells in 3 ways: Viral replication leaves the holes in the cell
membranes, Infected cells fuse with other cells, Antibodies against HIV bind to the
infected cells and activate the complement system, which destroy the infected cells.
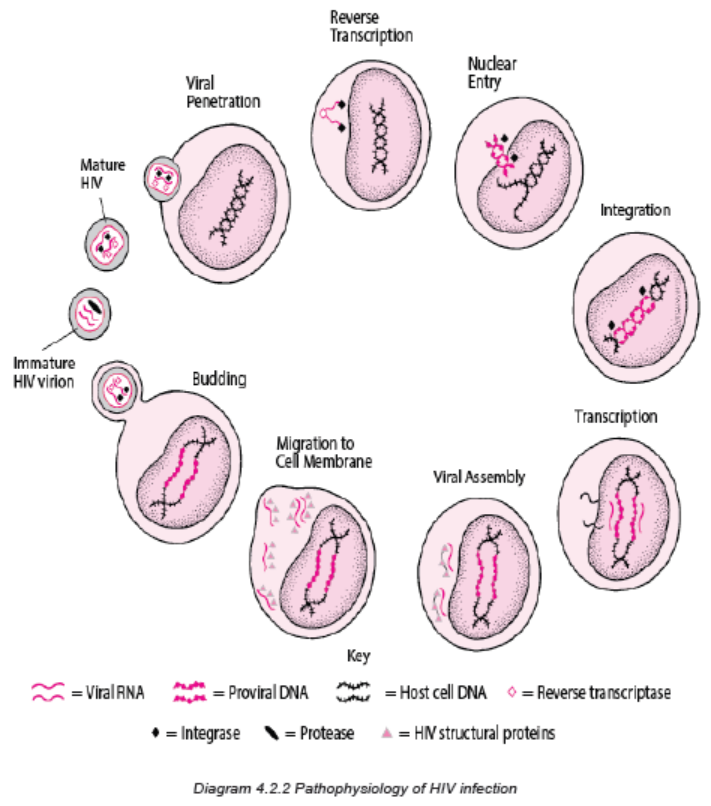
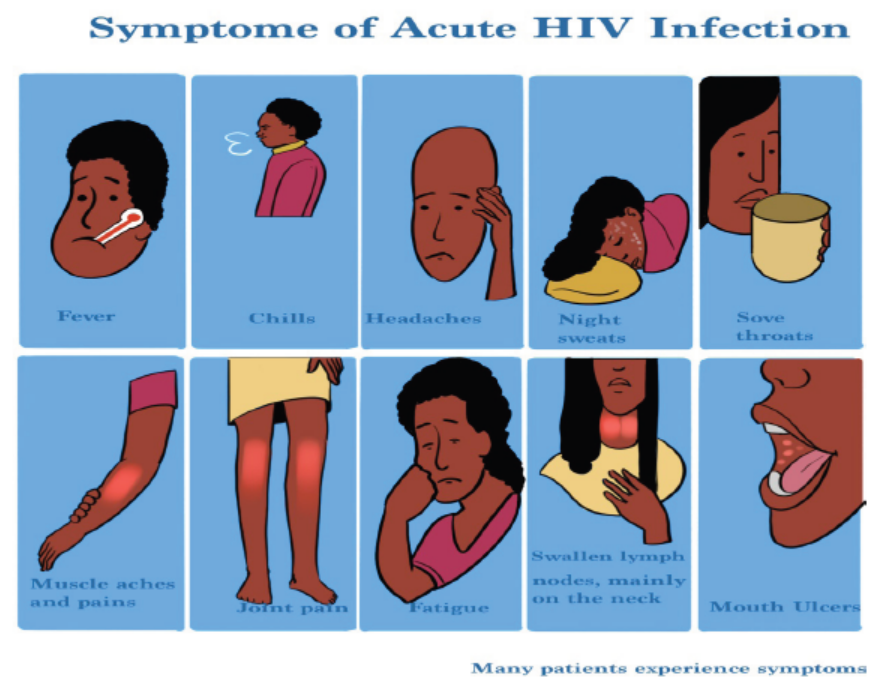
Figure4.2.4 Signs and symptoms of HIV infection
The symptoms of HIV and AIDS vary depending on the phase of infection:
Primary infection (Acute HIV): Some people infected by HIV develop a flu-like
illness within two to four weeks after the virus enters the body. This illness, known
as primary (acute) HIV infection, may last for a few weeks. Possible signs and
symptoms include fever, headache, muscle aches and joint pain, rash, sore throat
and painful mouth sores, swollen lymph glands, mainly on the neck, diarrhea,
weight loss, cough, night sweats.
These symptoms can be mild that the patient might not even notice them. However,
the amount of virus in your bloodstream (viral load) is quite high at this time. As a
result, the infection spreads more easily during primary infection than during the
next stage.
Clinical latent infection (Chronic HIV): In this stage of infection, HIV is still
present in the body and in white blood cells. However, many people may not have
any symptoms or infections during this time. This stage can last for many years if
the patient is not receiving antiretroviral therapy (ART). Some people develop more
severe disease much sooner.
Symptomatic HIV infection: As the virus continues to multiply and destroy the
immune cells (the cells in your body that help fight off germs) may develop mild
infections or chronic signs and symptoms such as fever, fatigue, swollen lymph
nodes often one of the first signs of HIV infection, diarrhea, weight loss, oral yeast
infection (thrush), shingles (herpes zoster), pneumonia.
Progression to AIDS: Untreated, HIV typically turns into AIDS. When AIDS occurs,
the immune system has been severely damaged. The patient is more likely to
develop opportunistic infections or opportunistic cancers or diseases that wouldn’t
usually cause illness in a person with a healthy immune system. The signs and
symptoms of some of these infections may include sweats, chills, recurring fever,
chronic diarrhea, swollen lymph glands, persistent white spots or unusual lesions
on your tongue or in your mouth, persistent or unexplained fatigue, weakness,
weight loss, skin rashes or bumps.
Investigations
Diagnosing HIV should be done basing on:
Clinical suspicion: due to the wide range of symptoms associated with acute
HIV infection, the possibility of HIV infection should be considered in patients who
present with the more typical signs and symptoms, including an ill-defined febrile
illness, heterophile-negative mononucleosis-like syndrome, heterophile positive
mononucleosis in an unusual host (for example, an older adult patient), and/or
aseptic meningitis. Certain clinical features, such as a rash, mucocutaneous ulcers,
diarrhea, or lymphadenopathy, should heighten the suspicion for HIV infection
HIV can be diagnosed through blood or saliva testing. During the use of blood
test to diagnose HIV infection, If the test is positive (meaning that HIV antibodies or
antigens are found), a test to detect HIV DNA or RNA will be done to be sure. HIV
antibodies may show up in the blood as early as 2 to 4 weeks after contact but can
also take as long as 3 to 6 months to show up in the blood.
When the possibility of acute or early HIV infection is being considered, we perform
the most sensitive screening immunoassay available (ideally, a combination
antigen/antibody immunoassay) in addition to an HIV virologic (viral load) test. We
favor using an RT-PCR based viral load test, if available. A positive HIV virologic
test is generally indicative of HIV infection
Available tests include:
• Antigen/antibody tests: These tests usually involve drawing blood from a
vein. Antigens are substances on the HIV virus itself and are usually detectable
— a positive test — in the blood within a few weeks after exposure to HIV.
• Antibodies are produced by the immune system when it’s exposed to HIV.
It can take weeks to months for antibodies to become detectable. The
combination antigen/antibody tests can take two to six weeks after exposure
to become positive.
• Antibody tests: These tests look for antibodies to HIV in blood or saliva.
Most rapid HIV tests, including self-tests done at home, are antibody tests.
Antibody tests can take three to 12 weeks after the patient is exposed to
become positive.
• Nucleic acid tests (NATs): These tests look for the actual virus in your
blood (viral load). They also involve blood drawn from a vein. If you might
have been exposed to HIV within the past few weeks, the doctor may
recommend NAT. NAT will be the first test to become positive after exposure
to HIV
• In addition to these tests, there is need of general screening to look for
hemodynamic and physiological status of a person suspected (FBC, Urea,
Creatinine, electrolytes, ASAT and ALAT and any other helpful investigation
depending on patient condition).
Once the patient thinks that he/she has been exposed to HIV but the test is negative,
should get tested again. A repeat test can be done after a few weeks to be sure he/
she is not infected.
After the confirmation of diagnosis of HIV/AIDS, several tests can help the clinician
to determine the stage of the disease and the best treatment:
CD4 T cell count: CD4 T cells are white blood cells that are specifically targeted
and destroyed by HIV. Even if the patient doesn’t have symptoms, HIV infection
progresses to AIDS when the CD4 T cells count below 200.
Viral load (HIV RNA): This test measures the amount of virus in your blood.
After starting HIV treatment the goal is to have an undetectable viral load. This
significantly reduces your chances of opportunistic infection and other HIV-related
complications.
Drug resistance: Some strains of HIV are resistant to medications. This test helps
the clinician to determine if the specific form of the virus has resistance and guides
treatment decisions.
Treatment plan
The standard treatment for HIV is a combination of medicines called antiretroviral
therapy or ART or ARV drugs. Antiretroviral medicines slow the rate at which the
virus multiplies. Taking these medicines can reduce the amount of virus in the body
and help to stay healthy.
Preventive strategies
There’s no vaccine to prevent HIV infection and no cure for AIDS. But you can
protect yourself and others from infection.
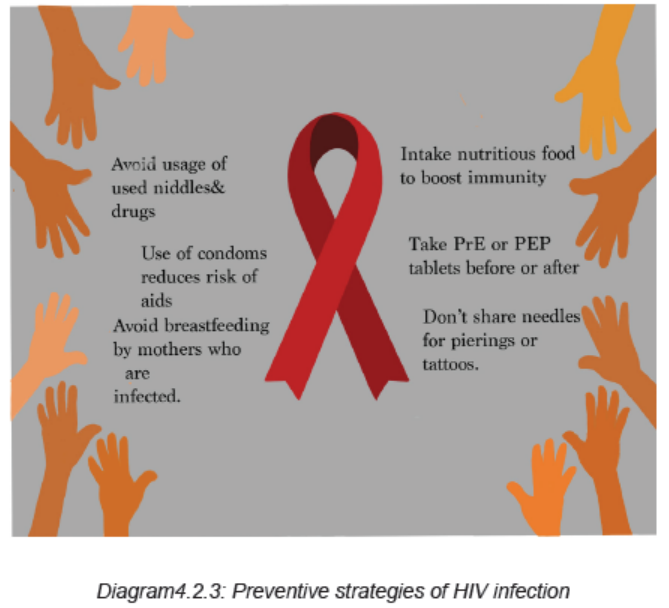
To help to prevent the spread of HIV:
Use treatment as prevention: If living with HIV, taking HIV medication can keep
the partner from becoming infected with the virus. If the viral load stays undetectable
(a blood test doesn’t show any virus) the patient will not transmit the virus to anyone
else. This requires taking the medication exactly as prescribed and getting regular
check-ups.
Use post-exposure prophylaxis (PEP) after being exposed to HIV: If exposed
through sex, needles or in the workplace, contact the doctor or go to the emergency
department or HIV clinic. Taking PEP as soon as possible within the first 72 hours
can greatly reduce the risk of becoming infected with HIV. Patient will need to take
medication for 28 days.
Use a new condom every time having sex: Use a new condom every time client
has anal or vaginal sex. Women can use a female condom. If using a lubricant,
make sure it’s water based. Oil based lubricants can weaken condoms and cause
them to break.
Consider Pre-exposure prophylaxis (PrEP): The combination drugs emtricitabine
plus tenofovir (Truvada) and emtricitabine plus tenofovir alafenamide (Descovy)
can reduce the risk of sexually transmitted HIV infection in people at very high
risk. PrEP can reduce the risk of getting HIV from sex by more than 90% and from
injection drug use by more than 70%, according to the Centers for Disease Control
and Prevention. Client will need an HIV test before start taking PrEP and then every
three months as long as he/she is taking it. The doctor will also test the kidney
function before prescribing Truvada and continue to test it every six months. These
PrEP drugs don’t prevent other STIs, so patient still need to practice safe sex. If
client has hepatitis B or C, he/she should be evaluated for any infectious disease or
liver disease before beginning therapy.
Tell the sexual partners if client has HIV: It›s important to tell all the current and
past sexual partners that client is HIV-positive. They›ll need to be tested.
Use a clean needle: If using a needle to inject drugs, make sure it›s sterile and
don›t share it. Take advantage of needle-exchange programs in the community.
Consider seeking help for the drug use.
If client is pregnant, get medical care right away: If client is HIV-positive, she
may pass the infection to the baby. But if she receives treatment during pregnancy,
she can significantly cut the baby›s risk.
Consider male circumcision: There›s evidence that male circumcision can help
reduce the risk of getting HIV infection.
Adequate medical diagnosis
A variety of symptoms and signs may be seen in association with acute HIV
infection, known as the acute retroviral syndrome. The most common findings are
fever, lymphadenopathy, sore throat, rash, myalgia/arthralgia, and headache.
The diagnosis of acute HIV infection requires a high level of clinical suspicion and
should be considered in patients who present with consistent signs and symptoms,
including an ill-defined febrile illness, heterophile-negative mononucleosis-like
syndrome, and/or aseptic meningitis. Early HIV infection should also be considered
in patients who have had a recent high-risk exposure or those who have had a
recent sexually transmitted infection regardless of the presence of symptoms or
signs. When the possibility of acute or early HIV infection is being considered, we
perform the most sensitive immunoassay available (ideally, a combination antigen/
antibody immunoassay) in addition to an HIV virologic (viral load) test. A positive
virologic test indicates HIV infection.
All patients with suspected or confirmed acute or early HIV infection should be
counseled to adopt behaviors that guard against HIV transmission, including
consistent and correct condom use and avoidance of sharing injection drug use
equipment and develop other positive behaviors towards other people.
There is no cure of HIV but the standard treatment for HIV is a combination of
medicines called antiretroviral therapy or ART or ARV drugs. Antiretroviral medicines
slow the rate at which the virus multiplies. Taking these medicines can reduce the
amount of virus in your body and help you stay healthy.
Evolution and Complications
There’s no vaccine to prevent HIV infection and no cure for it. Taking the ART
medicines can reduce the amount of virus in the body and help to stay healthy.
There is also need of protecting yourself and others from infection.
HIV infection weakens the immune system, making the person much more likely to
develop many infections and certain types of cancers:
Infections common to HIV/AIDS:
Pneumocystis pneumonia (PCP): This fungal infection can cause severe illness.
Although it›s declined significantly with current treatments for HIV/AIDS, the PCP is
still the most common cause of pneumonia in people infected with HIV.
Candidiasis (thrush): Candidiasis is a common HIV-related infection. It causes
inflammation and a thick, white coating on the mouth, tongue, esophagus or vagina.
Tuberculosis (TB): In resource-limited nations, TB is the most common
opportunistic infection associated with HIV. It›s a leading cause of death among
people with AIDS.
Cytomegalovirus: This common herpes virus is transmitted in body fluids such as
saliva, blood, urine, semen and breast milk. A healthy immune system inactivates
the virus, and it remains dormant in the body. If the immune system weakens, the
virus resurfaces causing damage to the eyes, digestive tract, lungs or other organs.
Cryptococcal meningitis: Meningitis is an inflammation of the membranes and
fluid surrounding the brain and spinal cord (meninges). Cryptococcal meningitis is a
common central nervous system infection associated with HIV, caused by a fungus
found in soil.
Toxoplasmosis: This potentially deadly infection is caused by Toxoplasma gondii,
a parasite spread primarily by cats. Infected cats pass the parasites in their stools,
which may then spread to other animals and humans. Toxoplasmosis can cause
heart disease, and seizures occur when it spreads to the brain.
Cancers common to HIV/AIDS:
Lymphoma: This cancer starts in the white blood cells. The most common early
sign is painless swelling of the lymph nodes in the neck, armpit or groin.
Kaposi›s sarcoma: A tumor of the blood vessel walls, Kaposi›s sarcoma usually
appears as pink, red or purple lesions on the skin and mouth. In people with darker
skin, the lesions may look dark brown or black. Kaposi›s sarcoma can also affect
the internal organs, including the digestive tract and lungs.
Other complications related to HIV infection:
Wasting syndrome: Untreated HIV/AIDS can cause significant weight loss, often
accompanied by diarrhea, chronic weakness and fever.
Neurological complications: HIV can cause neurological symptoms such as
confusion, forgetfulness, depression, anxiety and difficulty walking. HIV-associated
neurocognitive disorders can range from mild symptoms of behavioral changes and
reduced mental functioning to severe dementia causing weakness and inability to
function.
Kidney disease: HIV associated nephropathy is an inflammation of the tiny filters
in the kidneys that remove excess fluid and wastes from the blood and pass them
to the urine.
Liver disease: Liver disease is also a major complication, especially in people who
also have hepatitis B or hepatitis C.
Self-assessment 4.2.4
1. Describe briefly the steps of HIV infection pathogenesis
2. What are different classes of ART drugs and their site of actions?
3. Describe different coping skills needed towards HIV preventive strategies
4. Differentiate signs and symptoms depending on the different phases of
HIV
5. Discuss different complications of HIV
4.2.5 Human Papilloma Virus (HPV)
Learning Activity 4.2.5
Read carefully this below situation and answer the following questions:
Mrs. N, V is a 39-year-old female patient who visited MUHIMA Hospital with
complaints of itching, burning, and discomfort of the genital area and the physical
examination (palpation and inspection) revealed large, pink, flat shaped wart
on the vulva. The history taking revealed that she is HIV Positive and treated
on Highly Antiretroviral therapy (HAAT) initiated 2 years ago as she delayed to
get tested for HIV/AIDs. Her vital signs were body temperature of 36.5 degree
Celsius, blood pressure of 100/70 mmHg, pulse rate was 68 beats per minute,
respiratory rate was 19 breaths per minute. The pap smear and DNA tests were
performed from vulva and cervical tissues and revealed abnormal cell growth,
the physician encouraged her to adhere to the ARVs treatment and salicylic
acid was prescribed to be applied on the affected area.
1. What are abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
4. What was included in the management of this case at different levels of
health care settings he visited?
5. If not treated, what will be the consequences?
Human papillomavirus is an infection caused by human papillomavirus (HPV), a
DNA virus from the papillomaviridae family.
Causes and risk factors
HPV infection occurs when the virus (human papillomavirus: HPV, a DNA virus
from the papillomaviridae family) enters the human body, usually through a cut,
abrasion or small tear in the skin. The virus is transferred primarily by skin-to-skin
contact.
Genital HPV infections are contracted through sexual intercourse, anal sex and
other skin-to-skin contact in the genital region. Some HPV infections that result in
oral or upper respiratory lesions are contracted through oral sex.If a client is pregnant and has an HPV infection with genital warts, it’s possible her
baby may get the infection. Rarely, the infection may cause a noncancerous growth
in the baby’s voice box (larynx).
Warts are contagious. They can spread through direct contact with a wart. Warts
can also spread when someone touches something that already touched a wart.
The Risk factors for HPV infection include number of sexual partners (The
more sexual partners that the client has, the more likely he/she is to contract a
genital HPV infection. Having sex with a partner who has had multiple sex partners
also increases the risk), Age (Common warts occur mostly in children. Genital warts
occur most often in adolescents and young adults), Weakened immune systems
(People who have weakened immune systems are at greater risk of HPV infections.
Immune systems can be weakened by HIV/AIDS or by immune system-suppressing
drugs used after organ transplants).
Other risks are damaged skin (Areas of skin that have been punctured or
opened are more prone to develop common warts), Personal contact (Touching
someone’s warts or not wearing protection before contacting surfaces that have
been exposed to HPV such as public showers or swimming pool might increase the
risk of HPV infection unprotected intercourse, numerous sexual partners and age at
first intercourse), Teens that are sexually active and young adult females are at
a higher risk of contracting the virus, than women and men over 25, the people who
are immunocompromised, such as young adults with HIV, Smokers have higher
rates of HPV infection, Contracting herpes or chlamydia increases the risk of
HPV infection “due to inflammation of the epithelial cells and breaks in the epithelial
layer that allows a pathway for HPV introduction”.
HPV can pass from person to person regardless of whether symptoms are present.
The strains of HPV that cause warts are different from those that increase the risk
of cancer.
In children, HPV can transmit to an infant during birth. However, research suggests
that this risk is relatively low, as the immune system usually takes care of the
infection in this situation. Signs of an HPV infection in an infant include genital warts
or lesions in the mouth. If a young child develops HPV symptoms, it may indicate
child abuse.
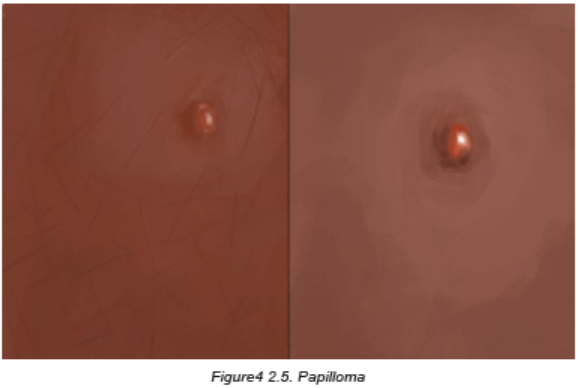
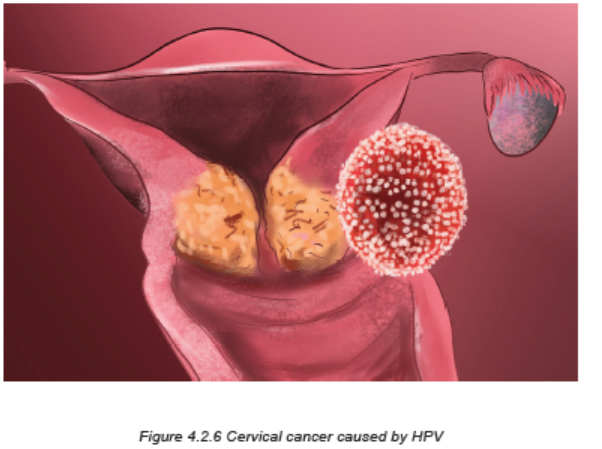
Pathophysiology overview
The HPV virus is a small, non-enveloped, double stranded DNA virus that infects
the mucosal or cutaneous epithelium. Since HPV affects epithelial cells and does
not enter the bloodstream, having an HPV infection in one part of the body should
not cause infection in another part. Once HPV gets into the epithelial cell, the virus
begins to make proteins that can interfere with normal functions in the cell, enabling
the cell to grow in an uncontrolled manner and to avoid apoptosis. HPV modifies
the DNA damage response (DDR) pathways by interacting with many proteins,
including ATM, ATR, MRN, y-H2AX, Chk1, Chk2, p53, BRCA1, BRCA2, RAD51,
etc. The HPV virus can activate and dysregulate DDR pathways throughout various
stages of their life cycles to replicate itself in host cells. Cell biology during a different
periods of a woman’s life can make her more susceptible to contracting the virus.
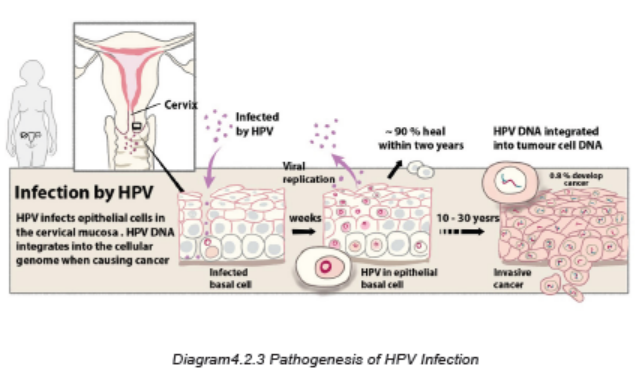
Signs and symptoms
Once infected, many patients remain asymptomatic and most cases resolve on
their own. The virus can remain dormant for years and then appear untriggered.
Appearance of ano-genital warts or abnormal pap smears are signs of likely HPV
infection.
In most cases, the body’s immune system defeats an HPV infection before it creates
warts. Symptoms of HPV may appear years after the initial infection. Some types of
the virus cause warts to form, while others can increase the risk of cancer. A person
may have one small skin bump, a cluster of bumps, or stem-like protrusions. These
warts can range in size and appearance, and they may be large or small, flat or
cauliflower-shaped, white, pink, red, purplish-brown, or skin-colored. The warts can
be formed on the vulva, cervix, penis or scrotum, anus, groin area, face or at any
part of the musculoskeletal system. These warts can cause itching, burning, and
other discomfort. When warts do appear, they vary in appearance depending on
which kind of HPV is involved:
Genital warts: These appear as flat lesions, small cauliflower-like bumps or tiny
stem like protrusions. In women, genital warts appear mostly on the vulva but can
also occur near the anus, on the cervix or in the vagina. In men, genital warts
appear on the penis and scrotum or around the anus. Genital warts rarely cause
discomfort or pain, though they may itch or feel tender.
Common warts: Common warts appear as rough, raised bumps and usually occur
on the hands and fingers. In most cases, common warts are simply unsightly, but
they can also be painful or susceptible to injury or bleeding
Plantar warts: Plantar warts are hard, grainy growths that usually appear on the
heels or balls of the feet. These warts might cause discomfort.
Flat warts: Flat warts are flat-topped, slightly raised lesions. They can appear
anywhere, but children usually get them on the face and men tend to get them in
the beard area. Women tend to get them on the legs. Flat warts are smaller and
smoother than other warts. They generally occur on the face or legs and are more
common in children and teens than in adults.
Female genital warts: Genital warts are a common sexually transmitted infection.
They can appear on the genitals, in the pubic area or in the anal canal. In women,
genital warts can also grow inside the vagina.
Male genital warts: Genital warts are a common sexually transmitted infection.
They can appear on the genitals, in the pubic area or in the anal canal.
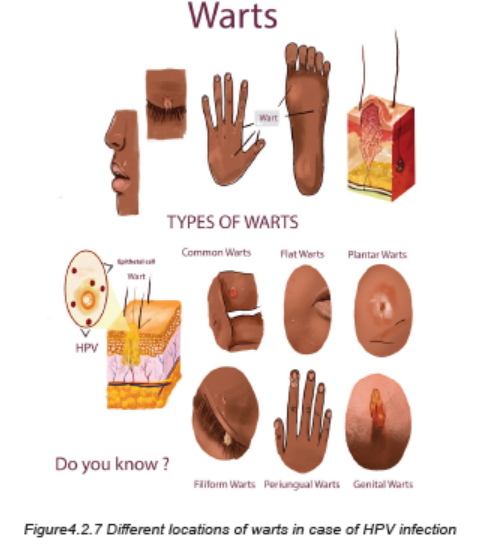
HPV and cervical cancer: nearly all cervical cancers are caused by HPV infections,
but cervical cancer may take 20 years or longer to develop after an HPV infection.
The HPV infection and early cervical cancer typically do not cause noticeable
symptoms. Being vaccinated against HPV infection is the best protection from
cervical cancer.
Because early cervical cancer does not cause symptoms, it is vital that women have
regular screening tests to detect any precancerous changes in the cervix that might
lead to cancer. Current guidelines recommend that women ages 21 to 29 have a
Pap test every three years. Women ages 30 to 65 are advised to continue having a
Pap test every three years, or every five years if they also get the HPV DNA test at
the same time. Women over 65 can stop testing if they have had three normal Pap
tests in a row, or two HPV DNA and Pap tests with no abnormal results.
Investigations
Specimens from cervical tissue are examined microscopically immediately after
they are collected to reveal the abnormal cells growth, vinegar (acetic acid) solution
test. A vinegar solution applied to HPV-infected genital areas turns them white. This
may help in identifying difficult-to-see flat lesions.
Pap test: the doctor collects a sample of cells from your cervix or vagina to send
for laboratory analysis. Pap tests can reveal abnormalities that can lead to cancer.
DNA test: This test, conducted on cells from the suspect’s cervix, can recognize the
DNA of the high-risk varieties of HPV that have been linked to genital cancers. It›s
recommended for women 30 and older in addition to the Pap test.
The WHO recommends 3 different types of screening tests: HPV DNA testing for
high-risk HPV types, Visual inspection with Acetic Acid (VIA), conventional (Pap)
test and liquid-based cytology (LBC).
Adequate medical diagnosis
Human papillomavirus (HPV) is the most common sexually transmitted infection
(STI).
Many people with HPV don’t develop any symptoms but can still infect others
through sexual contact. HPV infection is a viral infection that commonly causes skin
or mucous membrane growths (warts). Symptoms may include warts on the genitals
or surrounding skin. An infection that causes warts in various parts of the body,
depending on the strain. If the warts are not visible, several tests/investigations can
be done to diagnose the HPV infection.
There is no cure for the virus and warts may go away on their own. Treatment
focuses on removing the warts. HPV vaccines work best if administered prior to
exposure to HPV. Therefore, WHO recommends to vaccinate girls, aged between
9 and 14 years, when most have not started sexual activity. A vaccine prevents the
HPV strains most likely to cause genital warts and cervical cancer is recommended
for boys and girls.
The vaccines cannot treat HPV infection or HPV-associated disease, such as
cancer. Because pre-cancerous lesions take many years to develop, screening
is recommended for every woman from aged 30 and regularly afterwards
(frequency depends on the screening test used). For women living with HIV who
are sexually active, screening should be done earlier, as soon as they know their
HIV status. Screening has to be linked to treatment and management of positive
screening tests.
Treatment plan
Medications to eliminate warts are typically applied directly to the lesion and
usually take many applications before they’re successful. Examples include:
Salicylic acid: Over-the-counter treatments that contain salicylic acid work by
removing layers of a wart a little at a time. For use on common warts, salicylic acid
can cause skin irritation and isn’t for use on the face.
Imiquimod: This prescription cream might enhance the immune system›s ability
to fight HPV. Common side effects include redness and swelling at the application
site.
Podofilox: Another topical prescription, podofilox works by destroying genital wart
tissue. Podofilox may cause burning and itching where it›s applied.
Trichloroacetic acid: This chemical treatment burns off warts on the palms, soles
and genitals. It might cause local irritation.
If medications don’t work, surgical management for treatment of pre-cancer
lesions will be used. WHO recommends the use of cryotherapy or thermal ablation/
Burning with an electrical current, Laser susrgery and Loop Electrosurgical Excision
Procedure (LEEP)/surgical removal when available. For advanced lesions,
women should be referred to gynaecologist for further investigations and adequate
management
For abnormal HPV or Pap test, the gynaecologist will perform a procedure called
a colposcopy. Using an instrument that provides a magnified view of the cervix
(colposcope), he/she will look closely at the cervix and take samples (biopsy) of any
areas that look abnormal.
Preventive measures
It’s difficult to prevent HPV infections that cause common warts. If there is a common
wart, prevent the spread of the infection and formation of new warts by not picking
at a wart and not biting your nails.
To reduce the risk of contracting HPV infections that cause plantar warts, wear
shoes or sandals in public pools and locker rooms.
To reduce the risk of developing genital warts and other HPV-related genital lesions,
there is need of being in a mutually monogamous sexual relationship, reducing
the number of sex partners, using a latex condom, which can reduce the risk
of HPV transmission.
HPV vaccine: Gardasil-9 is an HPV vaccine approved and can be used for males
and females to protect against cervical cancer and genital warts. CDC recommends
routine HPV vaccination for girls and boys ages from 9 to 14. It’s ideal for girls
and boys to receive the vaccine before they have sexual contact and are exposed
to HPV. Once someone is infected with HPV, the vaccine might not be as effective
or might not work at all.
Nurses play a key role in education and advocacy for receiving the vaccine. Nurses
must focus their care and health education on STI screenings, reproductive health
needs, lifestyle modifications, and primary prevention, and risk reduction education.
Evolution and complications
The human papilloma virus may cause oral and upper respiratory
lesions. Some HPV infections cause lesions on the tongue, tonsils, soft palate, or
within the larynx and nose.
Genital warts that go untreated may eventually cause abnormal urine flow in men (if
warts are present in the urethra); bleeding from the urethra, vagina, or anus; or
vaginal discharge.
The Pap test and HPV tests can detect cervical changes at an early stage, so that
cervical cancer can be avoided, in most cases. The HPV types that cause genital
warts are not linked to cancer, but some other types of HPV that also infect the
mucous membranes are linked to cancers. While most of those HPV infections
never cause any symptoms, some cause changes in the cells that eventually can
lead to cancer. High-risk types of HPV can cause these different types of cancers:
cervical cancer, vulvar cancer, vaginal cancer, penile cancer, anal cancer, cancer
of the back of the throat. There are no screening tests for the other types of
cancer caused by HPV, so it’s important to notice any changes in appearance,
lumps, skin changes, pain, abnormal bleeding, or any other abnormalities in the
areas potentially infected with HPV
Self-assessment 4.2.5
1. What is Human Papilloma virus?
2. Describe the causes and triggering factors contributing to the human
Papilloma Virus development
3. What are different treatment options for a patient with Human Papilloma
virus infection?
4. State the preventive measures to be taken to prevent Human Papilloma
Virus
5. What are possible investigations to be performed to diagnose HPV?
6. If HPV is not well treated effetely, what could be the complications?
4.2.6 HEPATITIS B
Learning Activity 4.2.6
Carefully read the case scenario below and answer the following
questions
A 28-year-old female presents to the clinic with a 10-day history of flu-like
symptoms, including anorexia and malaise. She does not report any pertinent
prior medical history or surgeries. She takes no medications. Her family history
is non-contributory, and she reports no sick contacts. She is sexually active with
multiple partners and has used oral contraceptives regularly for the past 12
years.
On physical examination, she is alert and oriented, in no acute distress. Her vital
signs are temperature of 38 degree celsius, pulse 78 beats/minute, respirations of
18 cycles/minute, and blood pressure of 121/78 mmHg. Her extraocular muscles
are intact; however, mild scleral icterus is noted. Heart sounds are regular rate
and rhythm without murmurs, and lungs are clear to auscultation bilaterally. The
abdomen is soft and not tender, except the liver that is tender when palpated and
extends 8 cm below the costal margin, with a smooth edge.
Initial laboratory testing is performed and shown Complete blood count
(CBC) that is within normal limits. Liver function tests are performed, and the
significant findings are Alanine aminotransferase (ALT) 3817 U/L (Normal 7-55
U/L), Aspartate aminotransferase (AST) 2152 U/L (Normal 8-48 U/L), Alkaline
phosphatase (ALP) 176 U/L (Normal 45-115 U/L), Albumin 3.4 g/dL (Normal 3.5-
5 g/dL), Total protein 6.7 g/dL (Normal 6.3-7.9 g/dL), Total bilirubin 8.5 mg/dL
(Normal 0.1-1.2 g/dL). Viral Serology for Hepatitis B revealed HBsAg Positive
(hepatitis B surface antigen), HBeAg (hepatitis B envelope antigen) Positive,
IgM Anti-HB core Positive, Ig (immunoglobulin) G Anti-HBe Negative, IgG Anti-
HBs Negative, Hepatitis B Virus-DNA Positive
1. Given the clinical case, what were the abnormal signs and symptoms the
patient was presenting?
2. What is mostly the medical diagnosis?
3. What are the causes and risk factors of developing the medical condition
described above?
4. What are different possible treatments of that medical condition?
5. What are the complications related to that medical condition?
Hepatitis B is a potentially life-threatening liver infection caused by the hepatitis
B virus (HBV). It can cause chronic infection and puts people at high risk of death
from cirrhosis and liver cancer. Hepatitis B is a serious liver infection caused by the
hepatitis B virus (HBV). For some people, hepatitis B infection becomes chronic,
meaning it lasts more than six months. Having chronic hepatitis B increases your
risk of developing liver failure, liver cancer or cirrhosis a condition that permanently
scars of the liver.
Hepatitis B infection may be either short-lived (acute) or long lasting (chronic).
Acute hepatitis B infection lasts less than six months. The immune system likely
can clear acute hepatitis B from the body, and patient should recover completely
within a few months. Most people who get hepatitis B as adults have an acute
infection, but it can lead to chronic infection.
Chronic hepatitis B infection lasts six months or longer. It lingers because the
immune system can›t fight off the infection. Chronic hepatitis B infection may last
a lifetime, possibly leading to serious illnesses such as cirrhosis and liver cancer.
Causes and risk factors
Hepatitis B infection is caused by the hepatitis B virus (HBV). The virus is passed
from person to person through blood, semen, or other body fluids. It does not spread
by sneezing or coughing.
Common ways that HBV can spread are:
Sexual contact: when having unprotected sex with someone who is infected. The
virus can be transmitted if the person’s blood, saliva, semen, or vaginal secretions
enter someone’s body.
Sharing of needles or Accidental needle sticks: HBV easily spreads through
needles and syringes contaminated with infected blood. Hepatitis B is a concern for
health care workers and anyone else who meets human blood.
Mother to child: Pregnant women infected with HBV can pass the virus to their
babies during childbirth. However, the newborn can be vaccinated to avoid getting
infected in almost all cases.
The hepatitis B virus can survive outside the body for at least 7 days. During this
time, the virus can still cause infection if it enters the body of a person who is not
protected by the vaccine. The incubation period of the hepatitis B virus ranges from
30 to 180 days. The virus may be detected within 30 to 60 days after infection and
can persist and develop into chronic hepatitis B, especially when transmitted in
infancy or childhood.
Pathophysiology
The hepatitis B virus is constructed of an outer capsule containing HBsAg (hepatitis
B surface antigen), an inner core containing HBcAg (HBV core antigen), and
the HBeAg (hepatitis Be antigen). As the blood becomes exposed to HBV, the
body mounts a cell-mediated immune response by sending cytotoxic T cells and
natural killer cells to the virus and release inflammatory cytokines. The greater the
immune response, the greater the chance of fighting the virus. As the hepatocytes
are attacked and infiltrated by the HBV, they appear to have a ground glass look
under histological exam due to the HBsAg infiltrating the cell’s cytoplasm – this is
a differentiator for HBV versus other forms of hepatitis. Because hepatocytes are
continually proliferating, the virus is constantly being shed into the blood which
contributes to chronic infection.
The liver cell injury during HBV infection occurs per these 3 mechanisms: first,
due to a restricted cytotoxic T cell response directed at HBcAg/HBeAg on HBV
infected hepatocytes (immune mediated cells injury); second, possible mechanisms
is direct cytopathic effect of HBcAg expression in infected hepatocytes (cytopathic);
thirdly, possible mechanism is high level expression and inefficient secretion of
HBsAg.
The process by which the HBV virus replicates occurs in six (simplified) steps:
Attachment: The virus enters the cell using endocytosis by binding to a receptor
on the surface of the cell.
Penetration: The viral membrane merges with the host cell membrane then sends
its DNA and several proteins into the host cell’s cytoplasm.
Uncoating: Unlike other viruses, HBV uses RNA to replicate. HBV has partially
double stranded DNA that must be made into fully double stranded DNA first. Core
proteins separate from the partially double stranded viral DNA and make covalently
closed circular DNA (cccDNA). The cccDNA becomes the transcription template for
four mRNAs.
Replication: The largest of the four mRNA is used to make new copies of the
genetic material.
Assembly: The four mRNA are reprocessed, forming progeny virions that are
returned to the nucleus where they are recycled and make additional virions.
Release: DNA is synthesized via reverse transcriptase and new virus is sent into
the cytoplasm, then towards the cell membrane where it is released.
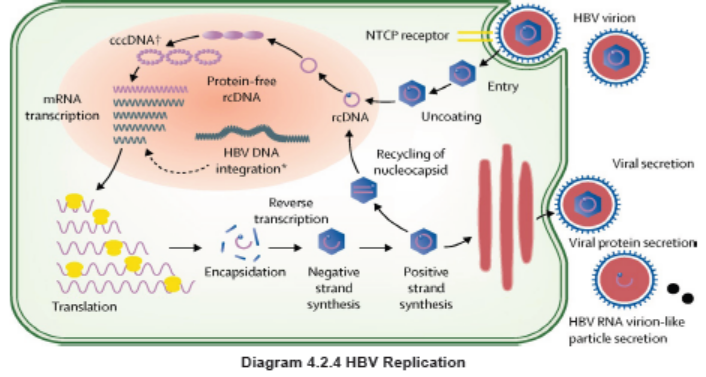
Signs and Symptoms
Most people do not experience any symptoms when newly infected with HBV.
However, some people have acute illness with symptoms that last several weeks,
including yellowing of the skin and eyes (jaundice), dark urine, extreme fatigue,
nausea, vomiting and abdominal pain. People with acute hepatitis can develop
acute liver failure, which can lead to death. Other Hepatitis B signs and symptoms
may include fever, joint pain, loss of appetite, nausea and vomiting, weakness and
fatigue, yellowing of your skin and the whites of your eyes (jaundice). The signs and
symptoms of hepatitis B range from mild to severe. They usually appear about one
to four months after you’ve been infected, although you could see them as early as
two weeks post-infection. Some people, usually young children, may not have any
symptoms.
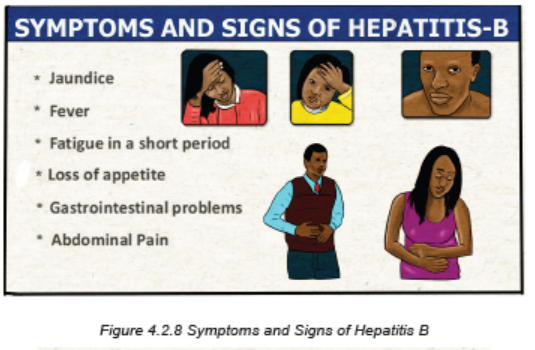
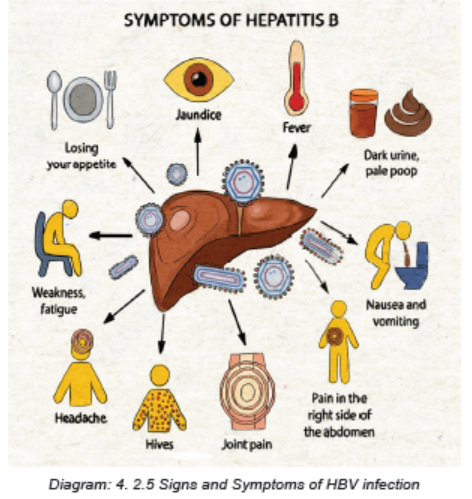
Investigations
It is not possible on clinical grounds to differentiate hepatitis B from hepatitis caused
by other viral agents; hence laboratory confirmation of the diagnosis is essential.
Several blood tests are available to diagnose and monitor people with hepatitis B.
They can be used to distinguish acute and chronic infections.
The initial evaluation of patients with chronic HBV infection should include:
• A history and physical examination, emphasizing risk factors for coinfection
with hepatitis C virus (HCV), hepatitis delta virus (HDV), and/or HIV; use of
alcohol; family history of HBV infection and hepatocellular carcinoma (HCC);
and signs and symptoms of cirrhosis.
• Laboratory tests, including: a complete blood count with focus on
platelets, liver chemistry tests like aspartate aminotransferase [AST], alanine
aminotransferase [ALT], total bilirubin, alkaline phosphatase, albumin,
international normalized ratio (INR), and tests for HBV replication (HBeAg,
antibody to HBeAg [anti-HBe], HBV DNA). Testing for immunity to hepatitis A
virus (HAV) with HAV immunoglobulin G (IgG) antibody should be performed
in patients who are not known to be immune.
• Evaluation for other causes of liver disease (eg, hemochromatosis, HCV,
HDV) by testing for iron, total iron binding capacity, ferritin, and HCV antibody
in all patients. Other experts suggest one-time screening for HDV in all
patients with chronic hepatitis B.
• Screening for HIV infection in those who have not undergone routine screening,
and in those persons with ongoing risk factors for HIV (eg, injection drug use,
multiple sexual exposures, men who have sex with men).
• Screening for HCC if indicated.
• Screening for fibrosis using noninvasive tests (eg, vibration-controlled
transient elastography, serum fibrosis panel) or liver biopsy. Noninvasive
assessments of liver fibrosis, notably measurements of liver stiffness, are
increasingly used instead of liver biopsies; however, liver stiffness can be
influenced by inflammation as well as fibrosis, and therefore, liver stiffness
measurements may overestimate liver fibrosis in patients with a high ALT
(more than 100 units/L)
• Liver biopsy: Most patients will not need a liver biopsy.
Adequate medical diagnosis
Hepatitis B is a vaccine-preventable liver infection caused by the hepatitis B virus
(HBV).
Hepatitis B is spread when blood, semen, or other body fluids from a person
infected with the virus enters the body of someone who is not infected. This can
happen through sexual contact; sharing needles, syringes, or other drug-injection
equipment; or from mother to baby at birth. Not all people newly infected with HBV
have symptoms, but for those that do, symptoms can include fatigue, poor appetite,
stomach pain, nausea, and jaundice. For many people, hepatitis B is a short-term
illness. For others, it can become a long-term, chronic infection that can lead to
serious, even life-threatening health issues like cirrhosis or liver cancer. The best
way to prevent hepatitis B is to get vaccinated.
Treatment Plan
There is no specific treatment for acute hepatitis B. Therefore, care is aimed at
maintaining comfort and adequate nutritional balance, including replacement
of fluids lost from vomiting and diarrhea. Most important is the avoidance of
unnecessary medications. Acetaminophen, paracetamol, and medication against
vomiting should be avoided.
Chronic hepatitis B infection can be treated with medicines, including oral antiviral
agents. Treatment can slow the progression of cirrhosis, reduce incidence of liver
cancer, and improve long term survival.
In low-income settings, most people with liver cancer die within months of diagnosis.
In high-income countries, patient present to hospital earlier in the course of the
disease and have access to surgery and chemotherapy which can prolong life for
several months to a few years. Liver transplantation is sometimes used in people
with cirrhosis or liver cancer in high-income countries, with varying success.
The goals of antiviral therapy are suppression of HBV DNA, loss of HBeAg (in
patients who were initially HBeAg-positive), and loss of HBsAg. Antiviral agents for
chronic HBV include pegylated interferon (PegIFN) or nucleos(t)ide analogs (eg,
entecavir and tenofovir). WHO recommends the use of oral treatments (tenofovir
or entecavir) as the most potent drugs to suppress hepatitis B virus. Most people
who start hepatitis B treatment must continue it for life. Antiviral agents that are
treatment strategies for chronic HBV typically include interferons or nucleoside
analogs (entecavir and tenofovir):
1. Interferon: the main role of interferon is primarily treatment of young patients
with well compensated liver disease who do not wish to be on long-term
treatment. The advantages of interferon compared to nucleoside analogs are
its finite duration of treatment. Furthermore, interferon should not be used in
pregnant women and patients with decompensated disease or compensated
cirrhosis and portal hypertension.
2. Nucleoside analogs: Several nucleoside analog agents are available. The
available agents include: Entecavir, Tenofovir, Lamivudine, Adefovir and
Telbivudine.
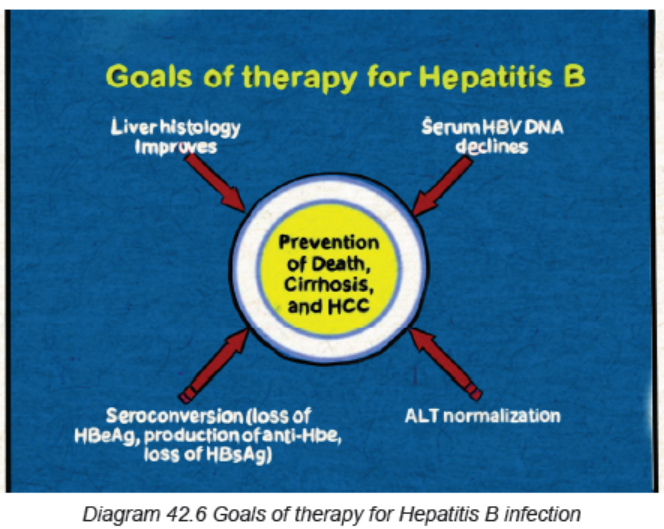
Prevention
A safe and effective vaccine that offers 98% to 100% protection against hepatitis B is
available. Preventing hepatitis B infection averts the development of complications
including chronic disease and liver cancer. The hepatitis B vaccine is typically given
as three or four injections over six months. The hepatitis B vaccine is recommended
for newborns, children and adolescents not vaccinated at birth, those who work or
live in a center for people who are developmentally disabled, people who live with
someone who has hepatitis B, health care workers, emergency workers and other
people who come into contact with blood, anyone who has a sexually transmitted
infection including HIV, Men who have sex with men, people who have multiple
sexual partners, sexual partners of someone who has hepatitis B, people who
inject illegal drugs or share needles and syringes and the health care professionals,
people with chronic liver disease, people with end-stage kidney disease, travelers
planning to go to an area of the world with a high hepatitis B infection rate.
Evolution and Complications
Most patients with hepatitis B recover fully, even if their signs and symptoms are
severe. Infants and children are more likely to develop a chronic (long-lasting)
hepatitis B infection. A vaccine can prevent hepatitis B, but there’s no cure if
you have the condition. If infected, taking certain precautions can help prevent
spreading the virus to others. The diagnosis of acute HBV infection is based upon
the detection of hepatitis B surface antigen (HBsAg) and IgM antibody to hepatitis B
core antigen (anti-HBc). For most patients, treatment is mainly supportive. Having
a chronic HBV infection can lead to serious complications such as:
Self-assessment 4.2.6
1. What are different modes of HBV transmission?
2. Briefly described the pathogenesis of HBV infection.
3. What are different investigations used to the diagnosis of HBV?
4. What are the complications resulting from HBV infection?
4.2.7 GENITAL HERPES
Learning Activity 4.2.7
Carefulyl read the case study below and answer the following questions
Mrs B.A is 28 year old female patient who was presented at Rubona Health
Center with complaints fever, headache, pain during sex intercourse, itching and
sores in the vagina and anus area. The vital signs were the body temperature
of 38.5 degree Celius, blood pressure of 120/70 mm Hg, PR was 88bpm. Mrs
B.A was immediately referred to Rwamagana Hospital where she received an
antiviral drugs tha she doesn’t remember. After six months the same symptoms
reappeared and she revisited the Rwamagana Hospital for further management.
Arriving at hospital, the medical doctor did complete physical eamination and
found that she had sores at external genitalia and inside the vagina.
He decided to hospitalise her, gave her IV fluids 1.5 liters/24 hours, brufen 400mg
three times a day for 3 days, IV ceftriaxone 500mg TDS for 5 days, Acyclovir
200mg TDS for 7 days and local care of sores. He also requested the complete
blood count, vaginal and cervical swabs that the results were pending.
1. What are the abnormal signs and symptoms that the patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been requetsed to confirm the
medical condition of Mrs B.A?
4. What was included in the treatment plan of this case?
5. If not well treated, what will be the complications?
Genital herpes is a common sexually transmitted infection caused by the herpes
simplex virus type 1 or type 2 and manifests as either a primary or recurrent
infection, Sexual contact is the primary way that the virus spreads. After the initial
infection, the virus lies dormant in the body and can reactivate several times a year.
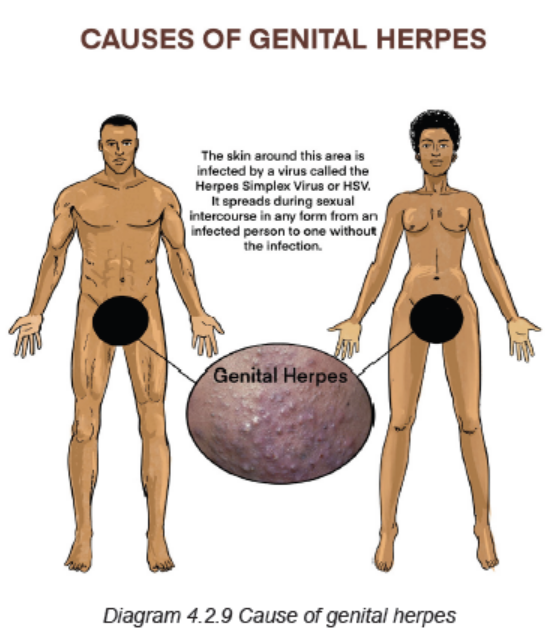
Two types of herpes simplex virus infections can cause genital herpes:
HSV-1: This is the type that usually causes cold sores or fever blisters around the
mouth. HSV-1 is often spread through skin-to-skin contact, though it can be spread
to the genital area during oral sex. Recurrences are much less frequent than they
are with HSV-2 infection.
HSV-2: This is the type that commonly causes genital herpes. The virus spreads
through sexual contact and skin-to-skin contact. HSV-2 is very common and highly
contagious, whether or not there is an open sore.
Because the virus dies quickly outside of the body, it’s nearly impossible to get the
infection through contact with toilets, towels or other objects used by an infected
person.
Risk factors for acquiring HSV-2 infection revolve around direct exposure to fluids
(i.e., semen, blood, saliva, etc.) from a seropositive individual containing viral
products most often during sexual intercourse. HSV-2 is mainly transmitted through
sexual intercourse, attributing to its predominant rise starting at puberty. Due to its
low stability outside the body, HSV can only remain infectious for days on moist
surfaces. Therefore, modes of transmission other than sexual intercourse are often
insignificant. Both primary and recurrent HSV infections in pregnant women can
lead to intrauterine transmission and resultant congenital HSV infection.
Pathophysiology
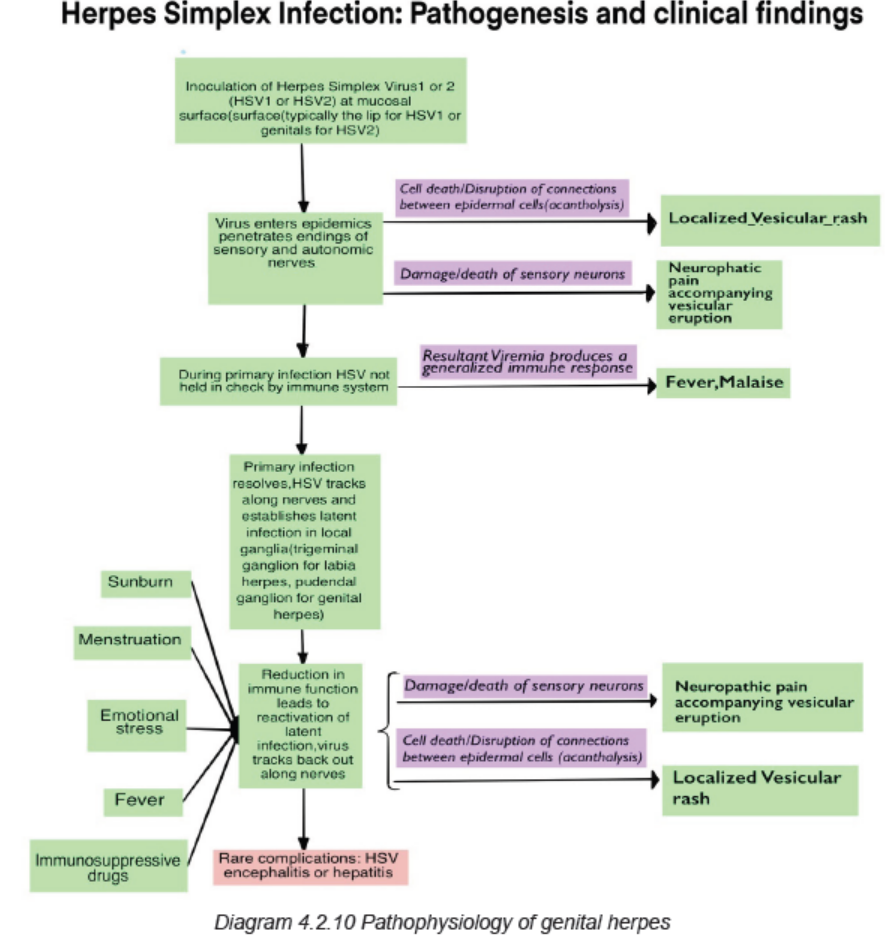
HSV-2 is transmitted through direct contact of sections in a seropositive individual
who is actively shedding the virus. The virus preferentially affects the skin and
mucous membranes with the virus invading epithelial cells on initial exposure
and ultimately replicating intracellularly at that site. After the initial exposure and
symptoms resolve, in 10 to 14 days, on average, the virus then lays dormant in
the periaxonal sheath of the sensory nerves of either the trigeminal, cervical,
lumbosacral, or autonomic ganglia. In these locations, the viral replication is often
controlled by the patient’s immune system and remains in a dormant state only to
later reactive later in life. When reactivation does occur, the virus travels through
the sensory nerves until it reaches the muco-cutaneous sites where replication then
takes place and leads to vesicular clusters at the dermatological site of that sensory
neuron.
Signs and Symptoms
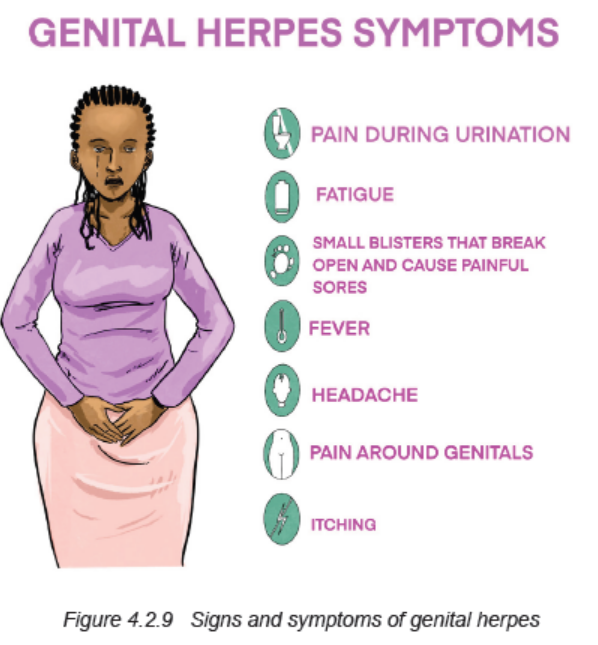
Most people infected with HSV do not know they have it because they don’t have
any specific signs or symptoms or because their signs and symptoms are so mild.
When present, symptoms may begin about two to 12 days after exposure to the
virus.
The signs and symptoms of genital herpes include:
Pain or itching: client may experience pain and tenderness in your genital area
until the infection clears.
Small red bumps or tiny white blisters or sores: These may appear a few days
to a few weeks after infection. Sores appear where the infection entered the body.
The infection can be spread by touching a sore and then rubbing or scratching
another area of the body, including the eyes.
Men and women can develop sores on the buttocks and thighs, anus, mouth and
urethra. Women can also develop sores in or on the vaginal area, external genitals,
and cervix. Men can also develop sores in or on the penis, and scrotum.
Ulcers: These may form when blisters rupture and ooze or bleed. Ulcers may make
very painful when urinating.
Scabs: Skin will crust over and form scabs as ulcers heal.
Genital herpes is different for each person. The signs and symptoms may recur,
off and on, for years. Some people experience numerous episodes each year. For
many people, however, the outbreaks are less frequent as time passes. During a
recurrence, shortly before sores appear, the client may feel burning, tingling and
itching where the infection first entered your body, pain in your lower back, buttocks
and legs. However, recurrences are generally less painful than the original outbreak,
and sores generally heal more quickly.
Investigations
Sometimes people mistake a pimple or ingrown hair for herpes. The doctor can
take a small sample from sores by using a swab test for laboratory examination.
If a client doesn’t have symptoms but think he/she might have herpes, the doctor
can order other test:
Viral culture: This test involves taking a tissue sample or scraping of the sores for
examination in the laboratory.
Polymerase chain reaction (PCR) test: PCR is used to copy the DNA from a
sample of the blood, tissue from a sore or spinal fluid. The DNA can then be tested
to establish the presence of HSV and determine which type of HSV the client has.
Blood test: This test analyzes a sample of the blood for the presence
of HSV antibodies to detect a past herpes infection.
Adequate medical diagnosis
Genital herpes is a common sexually transmitted infection marked by genital pain
and sores. It is caused by the herpes simplex virus, and this disease can affect
both men and women. Pain, itching and small sores appear first. They form ulcers
and scabs. After initial infection, genital herpes lies dormant in the body. Symptoms
can recur for years. Medication (mainly painkillers, antiviral drugs) can be used to
manage the condition.
Treatment plan
There’s no cure for genital herpes, but the treatment with antiviral medications may
help sores heal sooner during an initial outbreak, lessen the severity and duration
of symptoms in recurrent outbreaks, reduce the frequency of recurrence, minimize
the chance of transmitting the herpes virus to another. There are three major drugs
commonly used to treat genital herpes symptoms: acyclovir (zovirax), famciclovir
(famvir), and valacyclovir (valtrex). Moderate and minor cases are treated with
oral medications and severe cases may be treated with the intravenous (IV) drugs
seven to 10 days. Therapy should be initiated as early as possible following onset
of signs and symptoms.
Prevention
If the client is sexually active, there’s a chance to get herpes. He or she will make
it a lot less likely if he/she use a latex or polyurethane condom or dental dam every
time, for every activity. The dam or condom only protects the area it covers. If client
has herpes, he/she and his or her partner should get tested for STDs before sex.
To feel better during an outbreak, the client should wear loose-fitting clothes and
cotton underwear, avoid sun or heat that could cause more blisters, take a warm,
soothing bath, not use perfumed soaps or douches near the blisters.
Evolution and Complications
During vaginal birth, the herpes virus could spread to the baby, especially if the first
outbreak happens around the delivery time. The virus could give the baby rashes,
eye problems, or more serious issues. A caesarean section makes that less likely.
The doctor may also prescribe an anti-viral medicine starting at about 34 weeks to
avoid an outbreak around the due date.
Complications associated with genital herpes may include:
Other sexually transmitted infections: having genital sores increases the risk
of transmitting or contracting other sexually transmitted infections, including HIV/AIDS.
Newborn infection: babies born to infected mothers can be exposed to the virus
during the birthing process. This may result in brain damage, blindness or death forthe newborn.
Bladder problems: in some cases, the sores associated with genital herpes
can cause inflammation around the tube that delivers urine from the bladder to
the outside world (urethra). The swelling can close the urethra for several days,requiring the insertion of a catheter to drain the bladder.
Meningitis: in rare instances, HSV infection leads to inflammation of the membranesand cerebrospinal fluid surrounding the brain and spinal cord.
Rectal inflammation (proctitis): genital herpes can lead to inflammation of thelining of the rectum, particularly in men who have sex with men.
Pregnancy precautions: in case of pregnancy, the doctor may ask the woman
to be tested for genital Herpes and recommend her to start taking herpes antiviral
medications late in pregnancy to try to prevent an outbreak around the time of
delivery. If she is having a disease during the time she goes into labor, the doctorwill suggest a cesarean section to reduce the risk of passing the virus to the baby.
Self-assessment 4.2.7
1. What are the causes of genital Herpes?
2. Describe the pathophysiology of genital herpes.
3. What are the signs and symptoms of genital Herpes?
4. Which investigations should be requested to confirm the diagnosis of
genital Herpes?
5. What is the treatment plan of Genital Herpes?6. What are the complications of Genital Herpes?
4.2.8 TRICHOMONIASIS
Learning Activity 4.2.8
A 29-year-old man presented at Muhima DH complaining of oozing pus from
discrete areas over his glans penis with leaking of urine from those same
areas on micturition. This illness evolved over the preceding 7 months. He
was otherwise well. During the physical examination, the initial genitourinary
examination revealed a circumcised penis with two wart-like lesions and pus
oozing from the urethra. Prior to visit to Muhima Hospital, at Remera Health
center he was given cefixime 400 mg oral single dose, doxycycline 100 mg 12
hourly for 7 days, and metronidazole 2 g single dose over the preceding 7 months
with no improvement. At Muhima they did cytological examination of the purulent
discharge and found squamous epithelial cells and suppurative inflammation.
Organisms with features suggestive of Trichomonas vaginalis were observed.
The patient was treated with KMnO4 soaks for the lesions and tinidazole 2gr
single dose. He was sent back home and given the appointment to come after 1month for evaluation and possible biopsy of the wart lesions.
1. What were the signs and symptoms was the patient presenting?
2. What are the differential medical diagnoses that the patient was having?
3. What were the investigations requested to look for accurate medical
diagnosis?
4. What was involved into his treatment plan?5. If poorly treated, what will be the complications?
Trichomoniasis is a very common sexually transmitted disease (STD). It is caused
by infection with a protozoan parasite called Trichomonas vaginalis. Although
symptoms of the disease vary, most people who have the parasite cannot tell theyare infected.
Causes and risk factors
Trichomoniasis is caused by a one-celled protozoan “Trichomonas vaginalis “, a
type of tiny parasite that travels between people during sexual intercourse. The
incubation period between exposure and infection is unknown, but it’s thought to
range from four to 28 days.
The risk factors of trichomoniasis include having multiple sexual partners, a history
of other sexually transmitted infections, a previous episode of trichomoniasis, andsex without a condom.
Physiopathology
The parasite passes from an infected person to an uninfected person during sex.
In women, the most commonly infected part of the body is the lower genital tract
(vulva, vagina, cervix, or urethra). In men, the most commonly infected body part
is the inside of the penis (urethra). During sex, the parasite usually spreads from
a penis to a vagina, or from a vagina to a penis. It can also spread from a vagina
to another vagina. It is not common for the parasite to infect other body parts, like
the hands, mouth, or anus. It is unclear why some people with the infection get
symptoms while others do not. It probably depends on factors like a person’s age
and overall health. Infected people without symptoms can still pass the infection onto others.
Signs and symptoms
About 70% of infected people do not have any signs or symptoms. When
trichomoniasis does cause symptoms, they can range from mild irritation to severe
inflammation. Some people with symptoms get them within 5 to 28 days after
being infected. Others do not develop symptoms until much later. Symptoms can
come and go. Men with trichomoniasis may notice itching or irritation inside the
penis, burning after urination or ejaculation, discharge from the penis. Women with
trichomoniasis may notice itching, burning, redness or soreness of the genitals,
discomfort with urination, a change in their vaginal discharge (i.e., thin discharge or
increased volume) that can be clear, white, yellowish, or greenish with an unusual
fishy smell. Having trichomoniasis can make it feel unpleasant to have sex. Withouttreatment, the infection can last for months or even years.
Investigations
It is not possible to diagnose trichomoniasis based on symptoms alone. For both
men and women, the health care provider can examine the woman and get a
laboratory test to diagnose trichomoniasis. The healthcare provider may performthe following to diagnose trichomoniasis:
Complete physical exam (For women, this exam includes a pelvic exam)
Lab test: The healthcare provider examines a sample of the genital discharge
under a microscope to check for the cause of infection. The vaginal swab collected
may be sent to the lab for further testing if trichomonas are not seen under the
microscope. Trichomoniasis can be diagnosed by looking at a sample of vaginal
fluid for women or urine for men under a microscope. If the parasite can be
seen under the microscope, no further tests are needed. If this test isn’t conclusive,
tests called rapid antigen tests and nucleic acid amplification may be used.
Adequate medical diagnosis
Trichomoniasis also called trich, is a common sexual transmitted disease (STDs).
It is caused by a tiny one-celled parasite named Trichomonas vaginalis. Anyone
who’s sexually active can get it. It affects women more than men, older women
more than younger ones. People with trich often don’t have any symptoms, and
it doesn’t usually cause problems. But if you don’t get treatment, it raises your
chances of getting or spreading other STDs including HIV. Trichomoniasis can be
diagnosed by looking at a sample of vaginal fluid for women or urine for men under
a microscope. If the parasite can be seen under the microscope, no further tests
are needed. If this test isn’t conclusive, tests called rapid antigen tests and nucleic
acid amplification may be used. Without treatment, trich can last for months or even
years. It doesn’t go away on its own. The entire time the client is infected, he or shecan give the STD to his or her sexual partners.
Treatment plan
Trichomoniasis can be treated with medication prescribed by a doctor. These pills
are taken by mouth. It is safe for pregnant women to take this medication. People
who have been treated for trichomoniasis can get it again. About 1 in 5 people get
infected again within 3 months after receiving treatment. To avoid getting reinfected,all sex partners should get treated with antibiotics at the same time.
Oral anti-infective medications kill trich. The healthcare provider may prescribe
metronidazole (Flagyl®) or tinidazole (Tindamax®). It’s important to keep thefollowing points in mind while undergoing treatment:
• A single medication dose cures up to 95% of infected women. Men and
women may need to take the medication for five to seven days.
• Don’t drink alcohol for 24 hours after taking metronidazole or 72 hours after
taking tinidazole, because it can cause severe nausea and vomiting.
• Both sexual partners must be treated for trich.
• The client shouldn’t have sex for one week after finishing the medication to
give the drug time to kill off the infection and for symptoms to clear up. Having
sex too soon can lead to reinfection.
• The client should see the healthcare provider in three months to ensure you’re
no longer infected.
Wait to have sex again until everyone has been treated and any symptoms go away
(usually about a week). Get checked at 3 months to make sure that there is not a
new infection, or sooner if the symptoms come back before then.
Prevention
The only way to avoid STDs is not to have vaginal, anal, or oral sex.
If the client is a sexually active, he/she can do the following things to lower the
chances of getting trichomoniasis:
• Be in a long-term mutually monogamous relationship with a partner who has
been tested and has negative STD test results
• Use latex condoms the right way every time you have sex. This can lower the
chances of getting trichomoniasis.
• Get tested routinely for trichomoniasis and other STDs.
• Get treated if a client has trichomoniasis or other STDs.
• Tell the sexual partners if they have trich so they can get tested and treated.
• Limit the number of sexual partners.
Evolution and complications
Trichomoniasis can increase the risk of getting or spreading other sexually
transmitted infections. For example, trichomoniasis can cause genital inflammation
that makes it easier to get infected with HIV, or to pass the HIV virus on to a sex
partner. Untreated HIV can lead to AIDS. Women who have trich and HIV are
more likely to pass both diseases on to their partners. For this reason, the CDC
recommends that HIV-positive women get tested for trich at least once a year.
Pregnant women with trichomoniasis while pregnant or breastfeeding, it’s generally
safe to take anti-infective medication. Left untreated, trich increases the risk of
premature labor (childbirth before the 37th week of pregnancy), low birth weight(new-borns who weigh less than 2kg500), limit your number of sexual partners.
Self-assessment 4.2.8
1. What are the signs and symptoms of Trichomoniasis in man and woman?
2. Describe the pathophysiology of Trichomoniasis
3. What are the investigations that should be requested to confirm the medical
diagnosis of Trichomoniasis?
4. What is involved into the treatment plan of Trichomoniasis?
5. Explain the preventive measures for trichomoniasis.6. What are the complications of trichomoniasis?
4.3. END UNIT 4 ASSESSMENT
End unit assessment
1. Enumerate different commonest causes of UTI
2. Pathophysiological, describe how a UTI can lead to acute kidney injury.
3. What are the goals for UTI treatment?
4. What are general signs and symptoms of UTI.
5. Describe different complications of UTI.
6. Discuss different causes of urethritis.
7. Discuss different causes and risk factors of pyelonephritis.
8. Discuss different investigations helpful in diagnosis of pyelonephritis.
9. Different treatment options for pyelonephritis.
10. What are the investigations to be requested for diagnosing the prostatitis.
11. What are the investigations to request for diagnosing the syphilis?
12. What are different treatment options for gonorrhea?
13. Discuss different ways of HIV contamination.
14. Describe different preventive measures of HIV infection.
15. Discuss different complications related to HIV infection.
16. What are the risk factors of HPV infection?
17. Basing on the pathogenesis, discuss how HPV can lead do cervical cancer.
18. Describe different preventive measures of HPV.
19. What are different risk factors for development of Hepatitis B?
20. What are different investigations of diagnosing hepatitis B?
21. What are different treatment options for hepatitis B?
22. What are the complications of hepatitis B virus infection?23. What are different preventive measures of STDs?