UNIT 3 MEDICAL PATHOLOGIES OF DIGESTIVE SYSTEM
Key Unit Competences
To take an appropriate decision on management of common pathologies of digestivesystem.
Introductory activity 3.0
Carefully observe the picture below and answer the following questions:
Figure3.1 Patient with abdominal pain
1. What could be the patient complains?
2. Which body system is affected?3. What could be the possible medical conditions of that patient?
3.1 GASTRITIS
Learning Activity 3.1
Carefully read this below situation and answer the following questions:
A nurse is on day duty and receives Mr. N. J, a 54-year-old man who was
brought to RUBONA Health Center with complaints of epigastric pain (upper
abdominal pain), anorexia, and nausea. The history taking revealed that he is
alcohol dependent and cigarette smoker for 18 years ago. The body temperature
was 36.5 degree Celsius, blood pressure 110/70 mmHg, pulse rate was 74beats
per minute, respiratory rate was 19 breaths per minutes. Mr. N.J was treated with
anti-acid drug named Aluminum Hydroxide 500mg tablet three times a day for
5 days. After 1 day the patient returned with vomiting, general body weakness
and intravenous fluid (Ringer lactate 1litter in 4 hours) was given to him before
being transferred to the district hospital where through physical examination,
the physician noted pallor conjunctiva, complete blood count (CBC) was
performed and revealed white blood cells (WBC) of 105000, Hemoglobin level
of 9 mg/dl, Helicobacter Pylori test was positive. Prescribed medicine included
clarithromycin, omeprazole and flagyl, Vitamin B12 as well as blood transfusion.
Three days after the symptoms disappeared and the patient was encouraged by
the Registered Nurse to quit smoking and alcohol intake to maintain the healthy
state before being discharged to continue the oral treatment at home.
What are abnormal signs and symptoms that patient was presenting?
1. Basing on those signs and symptoms, what could be the medical problem
of this patient?
2. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
3. What was included in the management of this case?4. If not treated, what will be the consequences?
The human stomach has a protective lining of mucus called the mucosa. This lining
protects the stomach from the strong stomach acid that digests food. When something
damages or weakens this protective lining, the mucosa becomes inflamed, causing
gastritis. Gastritis is an inflammation of the stomach lining (gastric mucosa). It can
be classified as acute gastritis (erosive) or chronic gastritis (non-erosive). Erosive
(reactive): Erosive gastritis causes both inflammation and erosion (wearing
away) of the stomach lining. This condition is also known as reactive gastritis.
Causes include alcohol, smoking, nonsteroidal anti-inflammatory drugs (NSAIDs),
corticosteroids, viral or bacterial infections and stress from illnesses or injuries.
Non-erosive: Inflammation of the stomach lining without erosion or compromisingthe stomach lining.
Causes and risk factors of gastritis
Gastritis occurs when something damages or weakens the stomach lining (mucosa).
Different things can trigger the problem including dietary indiscretions; Bile reflux
(reflux of duodenal contents): the liver makes bile to help you digest fatty foods.
“Reflux” means flowing back. Bile reflux occurs when bile flows back into the
stomach instead of moving through the small intestine; Medications: Steady use of
nonsteroidal anti-inflammatory drugs (NSAIDs) such as Aspirin or corticosteroids
to manage chronic pain can irritate the stomach lining, alcohol or caffeine: Chronic
alcohol use can irritate the stomach lining; autoimmune disease: In some people,
the body’s immune system attacks healthy cells in the stomach lining;cigarette
smoking; ingestion of poisons or corrosive substances; food allergies; infection;
and gastric ischemia secondary to vasoconstriction caused by a stress response.
The bacterial infection: Helicobacter pylori may contribute to chronic gastritis,
the bacteria break down the stomach’s protective lining and causes inflammation.
Physical stress: A sudden, severe illness or injury can bring on gastritis. Gastritis
often develops even after a trauma that doesn’t involve the stomach. Severe burns
and brain injuries are the two common causes of gastritis. The risk of developing
gastritis goes up with age. Older adults have thinner stomach linings, decreased
circulation and a slower metabolism of mucosal repair, they are also more likely to
be on drugs that can cause gastritis such as nonsteroidal anti-inflammatory drugs
and other bacteria (staphylococci, streptococci, Escherichia coli), Herpes simplex
virus, cytomegalovirus (in acquired immunodeficiency syndrome; AIDS). In addition
the stress can induce acute gastritis especially for the critically ill patients. There
are other risk factors such as alcohol, caffeine, food containing acids (vinegar and
pepper).Pathophysiology overview
Gastric secretions are highly acidic. Parietal cells in the stomach increase acid
production (hydrochloric acid) in response to seeing, smelling, and eating food. The
release of histamine and acetylcholine by parasympathetic vagus nerve stimulates
the parietal cells. An increasing level of acid triggers the conversion of pepsinogen
to pepsin, creating a chemical mixture strong enough to digest the stomach wall.
However, because mucus protectively coats the stomach lining, pepsin normally
has little effect on the stomach wall. Prostaglandin E, a lipid compound secreted
in the stomach, apparently promotes the production of mucus, which contains
buffering substances and mechanically blocks penetration by stomach acids. Thesubmucosal layers of the stomach can become inflamed, however, when irritating
substances reduce or penetrate the mucous layer. Consequently, the client
experiences epigastric discomfort, often described as heartburn.
Signs and symptoms
Usually, the client complains of epigastric pain, feeling extra full during or after a
meal (fullness), pressure, anorexia (loss of appetite), nausea, and vomiting.
When the cause of gastritis is bacterial or viral, the patient may experience vomiting,
diarrhoea, fever, and abdominal pain. When the causes of gastritis are drugs,
poisons, toxic substances and corrosives, the patient may experience gastric
bleeding. Clients may describe seeing blood in emesis or note a darkening oftheir stool colour (black stool).
The chronic gastritis may be asymptomatic or presenting symptoms similar to mild
indigestion. As many people with gastritis don’t have symptoms, people who do
have symptoms often mistake them for indigestion. Other signs of gastritis include
bloating, loss of weight without meaning to, abdominal discomfort, hematemesis(vomiting blood).
Investigations
A complete blood count (CBC) may reveal anaemia from chronic blood loss.
Stool testing for occult blood often detects the presence of RBCs (Red blood cells)
in the stool. In difficult cases, gastroscopy or colonoscopy may be performed to
visualize the mucosa and obtain specimens, which are examined for pathogens or
cellular abnormalities. Helicobacter pylori test may also be performed to rule outHelicobacter pylori bacterial infection.
Medical diagnosis of gastritis
The health care personnel need to ask the client about the symptoms, conduct
a complete history taking and perform a physical exam, some tests may be also
performed to confirm the diagnosis including blood test which is designed to check
for antibodies titers that fight against H. pylori bacteria, stool test may also be
performed to rule out H. pylori in the patient’s stool. The physician may perform the
Upper endoscopy using an endoscope (a long thin tube with an attached camera)
to see in the patient’s stomach by inserting the scope through the oesophagus to
allow the physician to examine the stomach lining where the biopsy may be taken
from the patient stomach lining to test for infection. The X-ray images may be
taken after barium swallowing during upper gastrointestinal exam.
Treatment plan of gastritis
The treatment of gastritis depends upon its causes; poisons require emergency
treatment. In acute cases, eating is restricted and IV fluids such as Ringer lactate
or normal saline are given to correct dehydration and electrolyte imbalances,
particularly if vomiting is severe. Antiemetics are prescribed to control nausea and
vomiting, and antibiotics such as amoxicillin (Amoxil) and clarithromycin (Biaxin),
which exert bactericidal effects to eradicate H. pylori. Amebicides: Metronidazole
(Flagyl) assists in the eradication of H. pylori may be prescribed to inhibit or destroyinfection.
The usual treatment of chronic gastritis is the avoidance of irritating substances,
such as alcohol and NSAIDs. Some clients may wish to avoid spicy foods, high-fatfoods, and
caffeine, depending on the degree to which these items aggravate their symptoms.
Various drugs, such as antacids, H2- receptor antagonists such as Cimetidine,
and proton pump inhibitors such as Omeprazole may be prescribed to reducethe amount of stomach acid production.
Proton pump inhibitors also treat stomach ulcers and gastroesophageal reflex
disease (GERD). Antacids: example includes Aluminium Hydroxide Al (OH)3,
Magnesium Hydroxide (Mg(OH)3, these drugs initially are used to neutralize
existing stomach acid and provide quick pain relief. A combination of drugs may be
used to treat H. pylori including two antibiotics with an H2 antagonist (Amoxicillinor clarithromycin and Cimetidine).
The nurse monitors the client’s symptoms. Evaluating the client’s response to dietary
modifications and prescribed medications is important. The nurse observes the
colour and characteristics of any vomitus or stool that the client passes. In addition,
he or she teaches about diet, drug therapy, and the need for continued medical
follow-up. For complications such as ulcer formation, refer for better managementof peptic ulcer disease.
The preventive measures of gastritis may be encouraged to the general population
such as practicing good hygiene (hand- washing) to decrease the risk of H. pylori
infection transmission. H. pylori, can be contagious via the fecal-to-oral route. Good
hand washing before handling of foods and proper sanitation (sewer and water
systems) are the first line of defense against spread. Many people can develop
gastritis after being infected with H. pylori bacteria, minimizing indigestion and
heartburn as these conditions are linked to gastritis, avoiding fatty, spicy or acidic
foods, cutting back on caffeine, eating smaller meals throughout the day, managing
stress, not taking NSAIDs, reducing alcohol consumption and not lying down for 2to 3 hours after a meal would be taught to minimize the risk of contracting gastritis.
Evolution and complications
Most cases of gastritis improve quickly with treatment. For most people, medications
relieve gastritis. The healthcare provider will recommend the most appropriate
treatment based on what’s causing gastritis. Antacids reduce stomach acid, while
antibiotics clear up bacterial infections. The client can also make changes likereducing the alcohol consumption and managing pain without NSAIDs.
When the gastritis left untreated, it can lead to serious problems including
Anemia: H. pylori can cause gastritis or stomach ulcers (sores in the stomach)
that bleed, thereby lowering your red blood counts (called anemia). Pernicious
anemia due to the autoimmune gastritis can affect how the body absorbs vitamin
B12, which put the client at risk of pernicious anemia when there is not enough
B12 intake to make healthy red blood cells. Peritonitis may occur when stomach
ulcers are worse. Peritonitis may also be observed when ulcers are broken down
through the stomach wall thus causing stomach contents and spread of bacterial
to be found in the abdomen, which can lead later to sepsis and even death when
adequate measures are not taken timely. Stomach cancer: Gastritis caused by H.
pylori and autoimmune disease can cause growths in the stomach lining. Thesegrowths increase the patient‘s risk of developing stomach cancer.
Self-assessment 3.1
1. Define the term gastritis
2. Describe the causes and triggering factors contributing to the gastritis
development
3. What are different treatment options for a patient with acute gastritis?
4. State the preventive measures to be taken to prevent gastritis
5. What are possible investigations to be performed to confirm gastritis?6. If acute gastritis is not well treated, what could be the complications?
3.2 DIARRHEA
Learning Activity 3.2
Read carefully this below situation and answer the following questions:
Mr. B.V a 40 -year-old male was admitted to the emergency department of
RUHANGO Hospital where you are working as an Associate nurse. He came with
complains of headache, abdominal pain, discomfort and cramps (mesogastric
pain and epigastric pain), tiredness, anorexia, nausea, thirst, frequent watery
stool elimination with fats containing 5time a day. The history taking revealed
that he is from abroad where he took uncleaned food and drinks on the street
and bought water two days ago at the same area. Vital signs on admission were
as follows: body temperature was 36.5 degree Celsius, blood pressure 70/35
mmHg, pulse rate was 123bpm, and respiratory rate was 18 breaths per minutes.
Mr. B.V was urgently given ringer lactate 2litters bolus through intravenous and
the following investigations were performed: stool examination which revealed
amoebic infection, blood smear was negative. The patient was given loperamide
and oral rehydration salts to be taken home after intravenous rehydration.
1. What are the abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
4. What was included in the management of this case?5. What could be the appropriate topics of health education for this case?
In differentiating normal from abnormal, the consistency of stools and the comfort
with which a person passes them are more reliable indicators than is the frequency
of bowel elimination. The type and amount of food a person consumes greatlyaffect stool consistency.
Diarrhea is loss of watery stools (or bloody) for more than 3 times a day (more than
5 times a day for the neonates and small infants) or Diarrhea is the frequent passage
of larger-than-normal amounts of liquid or semiliquid stool (more than three bowel
movements per day). There are actually several different ways to classify diarrhea.
These types of diarrhea include:
• Acute diarrhea is loose watery diarrhea that lasts one to two days. This type
doesn’t need treatment and it usually goes away after a few days.
• Persistent diarrhea is a type of diarrhea that generally persists for severalweeks (two to four weeks).
• Chronic diarrhea is a diarrhea that lasts for more than four weeks or comesand goes regularly over a long period of time is called chronic diarrhea.
Causes and risk factors
Diarrhea is a common problem that can come suddenly or be a chronic complaint.
Some possible causes of diarrhea include food poisoning, infections, food allergies
or intolerances, and medication. There are also some conditions that cause chronic
diarrhea that run in families or, rarely, have a genetic basis.
Many different things can cause diarrhea in human gastro-intestinal tract in differentforms.
Acute diarrhea
Bacterial infections: Several types of bacteria consumed through contaminated
food or water can cause diarrhea. Common cause includes Campylobacter,
Salmonella, Shigella, and Escherichia coli (E. coli). If you eat something that
was improperly cooked or contaminated after cooking, the infection is called food
poisoning. Diarrhea, cramps, and vomiting are common with food poisoning.
Viral infections: Many viruses cause diarrhea, including rotavirus, Norwalk virus,
cytomegalovirus, herpes simplex virus, and viral hepatitis.
Food intolerances (maldigestion and or malabsorption syndrome): Some
people are unable to digest food components such as lactose; the sugar found in
milk, infants can also have milk-protein allergies.
Parasites: Parasites can enter the body through food or water and settle in the
digestive system. Parasites that cause diarrhea include Giardia lamblia, Entamoeba
histolytica.
Reaction to medicines (Medication): Antibiotics, cancer drugs (chemotherapy),
and antacids containing magnesium can all cause diarrhea, laxatives, digitalis,
metformin, cholesterol lowering agents, Lithium, Theophylline, Thyroid hormone
and colchicine.
Intestinal diseases: Inflammatory bowel disease, colitis, Crohn’s disease,
congenital aganglionic megacolon often lead to diarrhea.
Functional bowel disorders: Diarrhea can be a symptom of irritable bowel
syndrome
Too much caffeine or alcohol: there is a need to cut back on one or both to see if
that does the trick.
Toxins: such as insecticides, psychedelic mushrooms and arsenic cause diarrheatoo.
A digestive problem: this could be lactose intolerance, celiac disease or pancreaticproblems
A number of non-infectious medical conditions that may cause diarrhea including
inability to digest certain foods, including lactose intolerance (difficulty digesting
sugar found in dairy products); celiac disease (an immune reaction to consuming
gluten, a protein found in wheat, barley, and rye); and pancreatic problems, such as
those caused by cystic fibrosis, which interfere with production of important digestive
substances. Surgery to remove part of your small intestine. A shortened small
intestine may be unable to absorb all the substances you eat.
This is referred to as short-bowel syndrome. Surgical removal of the gallbladder.
An increase in bile in the colon may result in watery stools. Certain diseases of the
endocrine (hormonal) system, including overactive thyroid disease, diabetes,
adrenal disease, and Zollinger-Ellison syndrome. Certain rare tumors
(including carcinoid tumor and pheochromocytoma) that produce diarrhea-causing
substances (hormones). Inflammation in the intestinal tract, which can result in
chronic diarrhea. If you have inflammatory bowel disease (such as ulcerative colitis,
Crohn’s disease, or microscopic colitis), you will have regular bouts of diarrhea
during a flare-up of your disease. Irritable bowel syndrome, which may cause
alternating bouts of diarrhea and constipation. Ischemic bowel disease, which
can be caused by blocked arteries. Symptoms might include abdominal pain withbloody diarrhea.
Chronic diarrhea
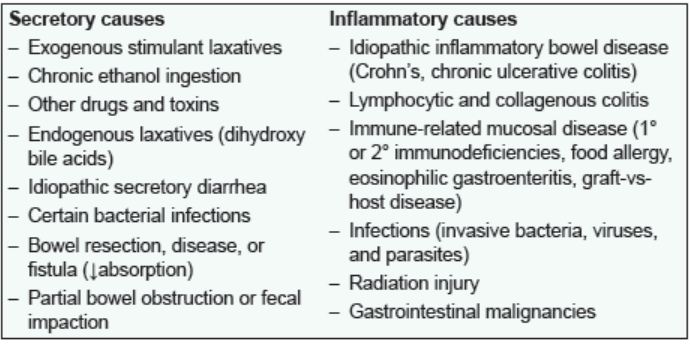
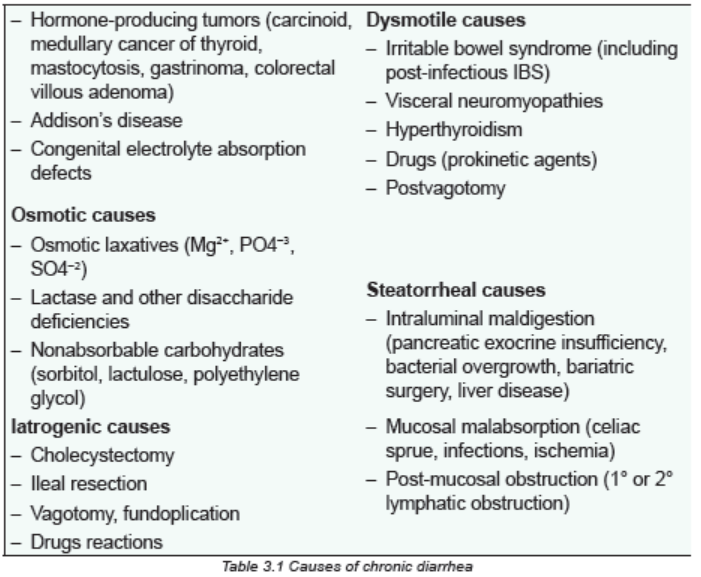
Diarrhea that persists longer than 4 weeks is considered to be chronic
Major Causes of Chronic Diarrhea according to predominantpathophysiologic mechanism.
Pathophysiology overview
Diarrhea results from increased peristalsis, which moves fecal matter through the GI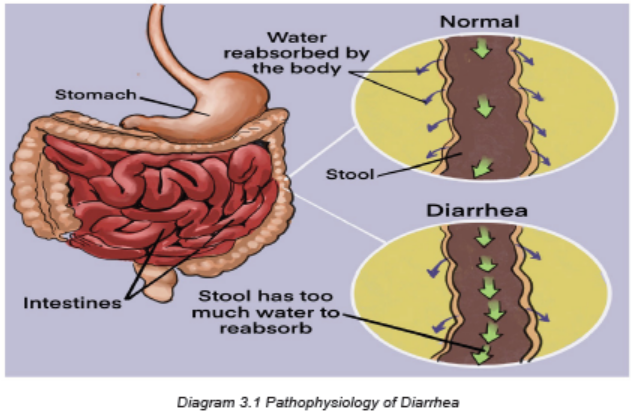
tract much more rapidly than normal. The swift velocity causes intestinal cramping
and decreases the time available for water to be absorbed from stool in the largeintestine. Consequently, the stool is either very soft or liquid.
Osmotic Diarrhea
Absorption of water in the intestines is dependent on adequate absorption of
solutes. If excessive amounts of solutes are retained in the intestinal lumen, water
will not be absorbed and diarrhea will result. Osmotic diarrhea typically results from
one of two situations: Ingestion of a poorly absorbed substrate, Malabsorption:
inability to absorb certain carbohydrates is the most common deficit in this categoryof diarrhea, but it can result virtually any type of malabsorption.
A common example of malabsorption, afflicting many adults humans and pets is
lactose intolerance. In such cases, a moderate quantity of lactose is consumed
(usually as milk), but the intestinal epithelium is deficient in lactase, and lactose
cannot be effectively hydrolyzed into glucose and galactose for absorption. The
osmotically-active lactose is retained in the intestinal lumen, where it “holds” water.
To add insult to injury, the unabsorbed lactose passes into the large intestine where
it is fermented by colonic bacteria, resulting in production of excessive gas.
A distinguishing feature of osmotic diarrhea is that it stops after the patient is fastedor stops consuming the poorly absorbed solute.
Secretory Diarrhea
Large volumes of water are normally secreted into the small intestinal lumen,
but a large majority of this water is efficiently absorbed before reaching the large
intestine. Diarrhea occurs when secretion of water into the intestinal lumen exceeds
absorption. Example in case of cholera, the Vibrio cholerae, produces cholera
toxin, which strongly activates adenylyl cyclase, causing a prolonged increase in
intracellular concentration of cyclic AMP within crypt enterocytes. This change results
in prolonged opening of the chloride channels that are instrumental in secretion of
water from the crypts, allowing uncontrolled secretion of water. Additionally, cholera
toxin affects the enteric nervous system, resulting in an independent stimulus of
secretion. Exposure to toxins from several other types of bacteria (e.g. E. coli
heat-labile toxin) induce the same series of steps and massive secretory diarrhea
that is often lethal unless the person or animal is aggressively treated to maintainhydration.
Inflammatory and Infectious Diarrhea
The epithelium of the digestive tube is protected from insult by a number of
mechanisms constituting the gastrointestinal barrier, but like many barriers, it can
be breached. Disruption of the epithelium of the intestine due to microbial or viral
pathogens is a very common cause of diarrhea in all species. Destruction of the
epithelium results not only in exudation of serum and blood into the lumen but often
is associated with widespread destruction of absorptive epithelium. In such cases,absorption of water occurs very inefficiently and diarrhea results.
The immune response to inflammatory conditions in the bowel contributes
substantively to development of diarrhea. Activation of white blood cells leads them
to secrete inflammatory mediators and cytokines which can stimulate secretion, in
effect imposing a secretory component on top of an inflammatory diarrhea. Reactive
oxygen species from leukocytes can damage or kill intestinal epithelial cells, which
are replaced with immature cells that typically are deficient in the brush border
enyzmes and transporters necessary for absorption of nutrients and water. In thisway, components of an osmotic (malabsorption) diarrhea are added to the problem.
Diarrhea Associated with Deranged Motility
In order for nutrients and water to be efficiently absorbed, the intestinal contents
must be adequately exposed to the mucosal epithelium and retained long enough
to allow absorption. Disorders in motility than accelerate transit time could decrease
absorption, resulting in diarrhea even if the absorptive process per se was
proceeding properly. Alterations in intestinal motility (usually increased propulsion)are observed in many types of diarrhea.
Signs and symptoms
The signs and symptoms of diarrhea depend on the cause. Symptoms and signs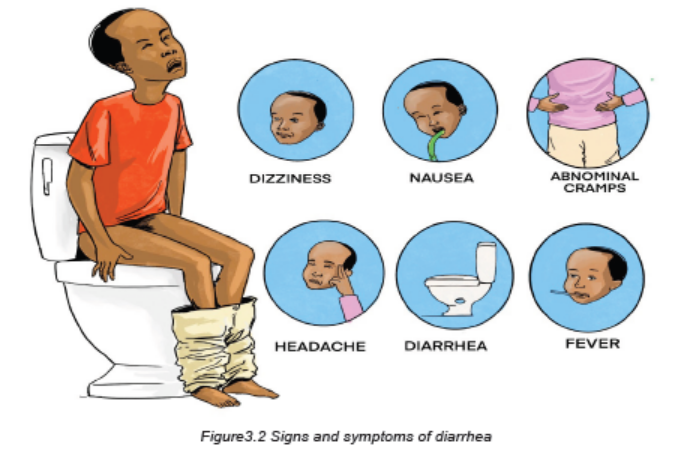
that often accompany with diarrhea may include: loose or watery stools for 4
weeks or longer in chronic diarrhea. The stools may be any color. The diarrhea
may appear even green in color, because stool passes through the intestines faster
than usual. Red stools indicate intestinal bleeding, so it may be a sign of a more
serious infection, bloating and gas, more frequent bowel movements, a sense of
urgency to pass stools, abdominal cramps, nausea, a burning sensation, fever,
dehydration. If diarrhoea causes dehydration, it is a sign of possibly severe health
issues. Some signs of dehydration are dark urine, dizziness and shakiness,
tiredness, fever, fatigue, dry mucous membranes, increased heart rate, a
headache, light-headedness, increased thirst, decreased urination, dry mouth.
In severe cases, blood and mucus pass with the stool. The client usually experiences
urgency (tenesmus) and abdominal discomfort. Bowel sounds are hyperactive.
Skin around the anus may become excoriated from contact with fecal matter
and products of the digestive process (e.g., gastric acid, bile salts). Fever may
be present. Infectious diarrhea typically has a sudden onset, with accompanyinggeneralized malaise.
Diarrhea in very young people is a serious condition. Seek urgent medical care
if any of the following symptoms apply to the child: diarrhea for 24 hours or more,
stools that contain blood, fever of 102°F (39°C) or higher, stools that contain pus,
stools that are black and tarry, signs and symptoms of dehydration (Dry mouth,
a headache, fatigue, a lack of tears when crying, dry skin, sunken eyes, Sunkenfontanel, sleepiness, irritability, decreased urination).
Investigations
Routine stool cultures are obtained to identify bacterial infections as the cause for
infectious diarrhea. Stool specimens obtained to identify parasites and their ova
are placed in special preservatives and analysed separately by the microbiology
department. Several samples may be needed because parasites are not typically
shed with each stool. Routine ova and parasite analysis may identify amoebic
infections; however, such infections may require serologic (blood) tests.
Blood in the stool may be common with certain infections and disease processes.
Nurses typically test stool specimens, collecting a specimen from the client (e.g.,
Hemoccult testing).
A proctosigmoidoscopy or colonoscopy may be performed to identify chronic
inflammation or alteration in the mucosal layer of the large intestine. These studies
often are carried out to identify the cause of chronic inflammation. An upper GI
series with small-bowel follow-through allows for radiologic examination of the
small bowel and identification of inflammation. Upper GI endoscopy allows foridentification of malabsorptive disorders such as celiac disease.
Adequate Medical Diagnosis
For the majority of mild diarrhea cases, there is no need for medical attention.
These cases are self-limited (only lasts for a fixed amount of time) and get better
without medical intervention. The key to mild diarrhea is supportive therapy –
staying hydrated and eating a bland diet. More serious cases of diarrhea may
require medical attention. In these situations, there are a few diagnostic tests that
the health care provider may order to determine the diagnosis. These tests can
include:
• Discussing a detailed family history, as well as physical and medical conditions,
the travel history, and any sick contacts the client may have.
• Doing a stool test on a collected stool sample to check for blood, bacterial
infections, parasite and inflammatory markers.
• Doing a breath test for lactose or fructose intolerance checkup and bacterial
overgrowth.
• Doing blood work to rule out medical causes of diarrhea such as a thyroid
disorder, celiac sprue (immune reaction to eating gluten, a protein found in
wheat, barley and rye) and pancreatic disorders.
• Doing endoscopic evaluations of the upper and lower digestive tract to ruleout organic abnormalities (ulcers, infections, neoplastic process).
Treatment plan
Treatment of diarrhoea that is mild or of short duration, such as that caused by
dietary changes or acute illness, involves resting the bowel by limiting intake to
clear liquids for one or two meals and gradually advancing to a regular diet. When
diarrhoea persists and stools are frequent and large, or if the person is very young,
elderly, or debilitated, medical treatment may include one or more of the followingmeasures:
• Administration of an antidiarrheal agent, such as diphenoxylate hydrochloride
with atropine sulfate (Lomotil), loperamide hydrochloride (Imodium), or a
combination product such as kaolin and pectin (Kaopectate)
• Fluid and electrolyte replacement by either the oral or intravenous (IV) route
• Dietary adjustments, which may involve eliminating foods that cause diarrhea.
Foods such as mashed potatoes, pasta, bread made with white flour, white
rice, and low fiber cereals are easy to tolerate. Yogurt is usually well tolerated
and contains probiotics that promote the growth of healthy GI bacteria. Milk
should be avoided for a few days because lactose intolerance may occur
during periods of acute diarrhea.
• Encourage potassium-rich foods as tolerated. Examples include bananas,
canned apricots and peaches, apricot nectar, orange juice, grapefruit juice,
tomato juice, fish, potatoes, and meat. Encourage client to withhold foods
until the acute attack subsides. Withholding food rests, the bowel and slows
peristalsis.
• Total parenteral nutrition (TPN) if diarrhea is severe and prolonged and if the
introduction of oral fluid and food results in another episode of diarrhea
• Reintroducing food after a bout of diarrhea usually calls for a diet low in
insoluble fiber to reduce the volume of stool. Insoluble fiber is found mostly
in whole grains, high-fiber cereals, raw vegetables, corn, nuts, seeds, and
the skins and seeds of fruit. Foods high in soluble fiber help slow GI motility;
examples include oatmeal, ripe bananas, and applesauce.
• Give clear liquids as tolerated, but limit high-sugar drinks. Drinking clear
liquids prevents dehydration; high-sugar drinks have high osmolality, which
may aggravate diarrhea.
• Advance oral intake as tolerated, initially offering foods high in soluble fiber
such as oatmeal, ripe bananas, and applesauce. Soluble fiber helps slow GI
motility.
• Teach client to avoid foods high in insoluble fiber, such as whole grain bread
and cereals, bran cereals, and raw vegetables. Caffeinated and carbonated
beverages should also be avoided. Such items stimulate GI motility.
• Encourage the intake of yogurt. Yogurt contains probiotics that help promotethe growth of healthy GI bacteria.
• Administer antidiarrheal medications as ordered for prolonged diarrhea.
These medications slow intestinal motility and inhibit peristalsis.
• Encourage client to rest in a comfortable position with legs bent toward the
abdomen. This position relaxes abdominal muscles and reduces discomfort.
• Advise client to avoid carbonated beverages or drinking with a straw. These
increase volume of swallowed air, which in turn increases gas and cramping.
The treatment of diarrhea focuses of signs and symptoms, etiology (antibiotics if
needed, etc) and aiming at preventing complications.
Preventive measures
The general preventive measures for diarrhea includes:
Improving sanitation mainly drinking water and sanitation lead to decreased risks
of diarrhea. Such improvements might include for example use of water filters,
provision of high-quality piped water and sewer connections.
Hand washing: Basic sanitation techniques can have a profound effect on the
transmission of diarrheal disease. The implementation of hand washing using soap
and water, for example, has been experimentally shown to reduce the incidence of
disease by approximately 30–48.
Vaccination: Immunization against the pathogens that cause diarrheal disease is a
viable prevention strategy, however it does require targeting certain pathogens for
vaccination such as Rotavirus vaccine.
Nutrition: dietary deficiencies in developing countries can be combated by
promoting better eating practices. Zinc supplementation proved successful showing
a significant decrease in the incidence of diarrheal disease compared to a control
group.
Breastfeeding practices have been shown to have a dramatic effect on the
incidence of diarrheal disease in poor populations. Studies across a number of
developing nations have shown that those who receive exclusive breastfeeding
during their first 6 months of life are better protected against infection with diarrheal
diseases.
Evolution and complications of diarrhea
Diarrhea is extremely common, but that doesn’t mean it can’t be dangerous. In
extreme cases of diarrhoea, a patient with diarrhoea can become very dehydrated
and this can lead to serious complications including hypovolemic choc and death
if poorly managed. Dehydration is one of the most dangerous side effects of
diarrhea. In the very young infants, small children and the very old this can haveserious consequences.
Diarrhea is a life-threatening condition because of dehydration and electrolyte
loss. The following are severe signs of dehydration: low blood sugar, fever and
chills, changes in breathing patterns, altered mental state, skin that when pinched
doesn’t immediately go back into place. If severe dehydration persists or is poorly
managed, it can lead to kidney failure, loss of consciousness, shock, coma, anddeath.
Self-assessment 3.2
1. Distingwish acute from chronic diarrhea.
2. State at least any five causes of diarrhoea disease development
3. What are treatment options for a patient with diarrhoea disease?
4. State at least three preventive measures to be taken to prevent diarrhoea
disease
5. What are possible investigations to be performed to rule out diarrhoeadisease?
3.3 CONSTIPATION
Learning Activity 3.3
Read carefully this below situation and answer the following questions:
A 40-year-old woman reports having infrequent bowel movements and bloating.
For many years, she typically has had bowel movements of hard, pellet-like stools
every two or three days. Over the last year, they have decreased in frequency to
every three or four days and are preceded by bloating and discomfort in the left
lower quadrant. The patient also usually strains excessively to pass stools. Vital
signs on admission were as follows: body temperature was 36.5 degree Celsius,
blood pressure 100/70 mmHg, pulse rate was 80bpm, and respiratory rate was
18 breaths per minutes. She was put on laxative drugs such as busacodyl as
stool softeners and encouraged fiber food intake and doing regular physicalexercise.
1. What are the abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What was included in the management of this case?
4. What could be the appropriate topics of health education for betterprevention of the above medical condition?
Constipation is known as difficulty in evacuation of faeces that may be accompaniedby the inability to defecate.
Causes and risk factors of constipation
• Irregular bowel habits, ignoring the need to defecate
• Chronic illness; e.g. Parkinson disease
• Low fibre diet and high animal fat intake
• Lack of fluid intake
• Stress
• Lack of physical exercises
• Colon cancer
• People depending on heavy laxative drugs
• Old age
Pathophysiology
Constipation is a condition in which stool becomes dry, compact, and difficult and
painful to pass. Normally, fecal matter collects in the rectum and presses on the
internal anal sphincter, creating an urge to defecate (eliminate stool). Peristalsis
and distention of the colon facilitate the signal to release stool. The gastrocolic
reflex facilitates stool passage by accelerating peristalsis. This reflex is most active
after eating, particularly after the first meal of the day. A diet low in fiber predisposes
people to constipation because the stools produced are small in volume and dry.
The lower GI tract propels low-volume stools more slowly. Whenever stool remains
stationary in the large intestine, moisture continues to be absorbed from the residue.
Consequently, retention of stool for any number of reasons, causes stool to become
dry and hard.
Rectal bleeding may result as the tissue stretches and tears while the person tries
to pass the hard, dry stool. When a practitioner inserts a gloved and lubricated
finger in the rectum, the stool may feel like small rocks, a condition referred to as
scybala (hardened masses of feces). Sometimes, if the client has been constipated
for a long time, he/she may begin passing liquid stool around an obstructive stool
mass (encopresis), a phenomenon sometimes misinterpreted as diarrhea. The
liquid stool results from dry stool stimulating nerve endings in the lower colon and
rectum, which increases peristalsis. The increased peristalsis sends watery fecesfrom higher in the bowel than the retained stool.
Signs & Symptoms
– Abdominal pain
– Bloating
– Staining during defecation
– No stool for 3 consecutive days or solid stool of inadequate volume...
– Fewer than three bowel movements a week
– Hard, dry, or lumpy stools
– Straining when using the bathroom
– Taking a long time to pass stools
– Feeling like having not passed all the stool
– Distention (bloating) of the belly
– Traces of liquid or clay-like stool in your child’s underwear—this can be a sign
that the stool is backed up in the rectum
– Blood on the surface of hard stool
– Fussiness and crying in infants in children
– Decreased appetite in infants and children
– Other odd behavior in infants and children
Investigations
A thorough history and physical examination (including digital rectal exam)
are necessary to determine the underlying cause and need for further diagnostic
testing. Frequently the diagnosis is based on findings of the history and physicalexamination, precluding the need for a more aggressive approach.
Abdominal radiography helps determine the extent of the constipation. A barium
enema is performed if a structural abnormality is suspected. In defecography, a
thick barium paste is inserted into the rectum. Radiographs are taken as the client
expels the barium to determine whether there are any anatomic abnormalities or
problems with the muscles surrounding the anal sphincter.
Colonic transit or marker studies are used to determine how long it takes for food
to travel through the intestines. For one or more days, clients swallow capsules
or solutions that contain radiographically visible plastic particles. After some days,
radiographs are taken to determine whether any particles are left and if so, where
they are. The location of the particles can help determine whether there is colonic
inertia related to muscle and/or nerve impairment or pelvic floor dysfunction.
Anorectal motility and/or colonic motility studies may be performed to confirm
a motility disorder. These studies use flexible catheters with sensors that measure
the pressure of muscle contractions.
Lower gastrointestinal (GI) endoscopy, sigmoidoscopy, and Colonoscopy
that represents the current criterion standard can also be done.
Other investigations to be considered are complete blood count (CBC), thyroid
function tests, blood glucose, serum electrolytes (sodium, potassium,
calcium, and magnesium).
Adequate Medical diagnosis
Functional constipation is clinical diagnosis that can generally be made on the basis
of typical history and an essentially normal physical examination including one of
the rectal examination is a key part of the initial evaluation.
Treatment plan of Constipation
Treating the cause provides the best relief. For quick symptomatic relief, the
physician prescribes an enema or a laxative in oral or suppository form, followed by
prophylactic administration of a stool softener. Diet therapy: encourage fibre food
intake (green vegetables, fruits like papaya), fluid intake, advice physical exercises,
enema (cleansing) may be required, laxative: e.g. Oral polyethylene glycol is better
tolerated.
Evolution and complications
Short term constipation typically does not cause complications and can usually
be treated with self-care. For example, if a patient is simply constipated due to a
change in the diet, he/she may feel full or bloated, but will not have any long-termcomplications. However chronic constipation can cause complications:
Hemorrhoids: are swollen and inflamed veins in the rectum or anus. They can
occur inside or outside and are usually not serious. External hemorrhoids may
cause itchiness or pain when having a bowel movement. Internal hemorrhoids
typically do not cause pain and, instead, you may see bright red-streaked stool in
the toilet.
Anal Fissures: are usually the result of some form of trauma to the anus, like hard
stool. Anal fissures are usually painful and may also cause itching. Client may also
notice blood on the toilet tissue or on the stool.
Rectal prolapse: occurs when the last portion of the colon, the rectum, protrudes
beyond the anus and is visible on the outside of the body. It is not necessarily
painful, and in many cases will go away without treatment. It should be evaluated
by the healthcare provider, though.
Faecal impaction: is a state of prolonged constipation. It occurs when the
stool is so hard that it cannot pass with a normal bowel movement. It can cause
abdominal pain and cramping, among other symptoms. It often must be treated with
medications or procedures such as enemas or water irrigation. Chronic constipation
can lead to fecal impaction and fecal incontinence. They state that in severe cases,
fecal impaction can cause stercoral ulcerations, intestinal obstruction, or bowel
perforation. If left untreated, these complications can be life-threatening.
Self-assessment activity 3.3
A 37-year-old woman comes to your clinic for “constipation,” that she had since
childhood. She states that a work-up by her paediatrician turned up nothing. She
reports intermittent crampy abdominal pain that reaches 8 out of 10 in severity
and is relieved “mostly” by a bowel movement. She has a bowel movement
nearly every day, but her stools are usually hard. When the pain occurs, her
stools are “really hard”. She was recently laid off from her job and has noted an
increase in her abdominal pain and hard stools.
1. What additional questions would you ask to learn more about her
symptoms?
2. What is constipation?
3. State at least any five causes of constipation disease development
4. What are possible investigations to be performed to rule out constipation
disease?
5. What are treatment options for a patient with constipation disease?
6. State at least three preventive measures to be taken to prevent constipation
disease.7. What are the complications of chronic constipation?
3.4 END UNIT 3 ASSESSMENT
End of unit assessment
1. Nursing management of the patient with chronic gastritis includes teaching
the patient to
a. Take antacids before meals to decrease stomach acidity.
b. Maintain a nonirritating diet with six small meals a day.
c. Eliminate alcohol and caffeine from the diet when symptoms occur.
d. Use nonsteroidal antiinflammatory drugs (nsaids) instead of aspirin for
minor pain relief.
2. A nurse is doing a nursing assessment on a patient with chronic constipation.
What data obtained during the interview may be a factor contributing to the
constipation?
a. Taking methylcellulose (Citrucel) daily
b. High dietary fiber with high fluid intake
c. History of hemorrhoids and hypertension
d. Suppressing the urge to defecate while at work
3. Which method is preferred for immediate treatment of an acute episode of
constipation?
a. An enema
b. Increased fluid
c. Stool softeners
d. Bulk-forming medication
4. A patient is admitted to the emergency department with acute abdominal
pain. What nursing intervention should the nurse implement first?
a. Measurement of vital signs
b. Administration of prescribed analgesics
c. Assessment of the onset, location, intensity, duration, and character of
the pain
d. Physical assessment of the abdomen for distention, bowel sounds, and
pigmentation changes
5. A 22-year-old patient calls the outpatient clinic complaining of nausea and
vomiting and right lower abdominal pain. What should the nurse advise the
patient to do?
a. Use a heating pad to relax the muscles at the site of the pain.
b. Drink at least 2 quarts of juice to replace the fluid lost in vomiting.
c. Take a laxative to empty the bowel before examination at the clinic.
d. Have the symptoms evaluated by a health care provider right away.
6. The appropriate collaborative therapy for the patient with acute diarrhea
caused by a viral infection is to:
a. Increase fluid intake.
b. Administer an antibiotic.
c. Administer antimotility drugs.
d. Quarantine the patient to prevent spread of the virus.
7. What are the preventive strategies of constipation?
8. What are the investigations to request for a patient with constipation?
9. What are the investigations to request for diagnosing gastritis?
10. What must be included into the treatment plan of gastritis?
11. What are the treatment modalities of diarrhea?
12. Discuss different risk factors of gastritis.
13. Referrring to pathophysiology, differentiate the osmotic, secretory andinflammatory diarrhea.