UNIT 2 PATHOLOGIES OF CARDIOVASCULAR SYSTEM
Key unit Competencies
Take appropriate decision on different common medical pathologies of cardiovascularsystem.
Introductory Activity 1.0
Observe the following schematic representation that shows the connectionbetween the heart and blood vessels and answer the following questions:
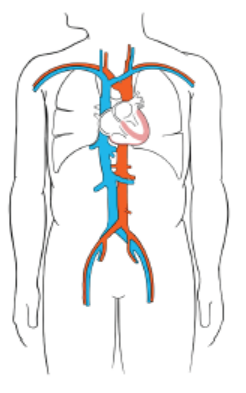
Figure 2.1 Blood Circulation system.
1. Basing on anatomy and physiology of the heart and circulatory system you
learnt, what do you think may happen to the human being if the required
cardiac output for better function of entire parts of the body changes are
noted?
2. What might be your interventions towards a patient with abnormal (lowand high) cardiac output?
1.1 HYPOTENSION
Learning Activity 2.1
Read carefully the case below and answer following questions:
A 52 years old female patient presented with general weakness, headaches and
occasional dizziness for the past three months. She had also had occasional
abdominal discomfort, moderate anorexia and weight loss due to nausea. She
tired more easily than before. She seemed frustrated and concerned about her
condition. During the examination, the blood pressure was 94/55 mmHg (Normal
systolic BP: 90-120mmHg/60-90 mmHg)), a regular pulse rate of 97 beats
per minute (Normal pulse 60-80 beats per minute), and a normal abdominal
examination. She was treated by some non-steroids anti-inflammatory drugs torelieve headache and sent back home.
During the following week, she continued to have same clinical manifestations
and decided to go back at health care setting. At arrival, blood pressure recheck
confirmed a significant drop from 94/55mmHg to 84/45mmHg. She also continued
to have headache associated with blurred vision. She was at that moment
unable to stand due to dizziness, severe headache and body weaknesses.
Her laboratory investigations revealed normal complete blood count with Hb:
12.5mg/dl (Normal value Hb: 11-16mg/dl), ASAT: aspartate aminotransferasee:
20U/l (Normal value: 10-30U/l), ALAT: alanine aminotransferase: 28U/l (10-40U/
l), creatinine: 0.8mg/dl (0.2-1mg/dl). The decision of hospitalizing her was taken,
prescribed the paracetamol 500mg three times per day for 3 days (painkiller)
and Ringer lactate and Normal saline 1.5 liter/24 hours (intravenous fluids)
and planned for further investigations to look for all possible causes of those
persistent signs and symptoms.
1. What are the abnormal signs and symptoms that the patient was
presenting?
2. From the case scenario, identify different investigations that have been
requested and their results?
3. Basing on those signs and symptoms, what could be the medical problem
of this patient?
4. What will be included in the medical and nursing management of this
case?5. If not treated, what will be the consequences?
The function of the cardiovascular system is to supply body cells and tissues with
oxygen-rich blood and eliminate carbon dioxide (CO2) and cellular wastes. Damage
and disease in the cardiovascular system greatly affect a person’s health and the
entire parts of his/her body. Cardiovascular diseases are conditions and diseases
that affect the heart and vasculature (blood vessels).
A good blood circulation requires the good cardiac output related to the capacity
of the heart to pump and the normal functionality of blood vessels that determine
the peripheral resistance. Blood pressure is the force exerted by the blood from
the heart against the walls of the blood vessels. It must be adequate to maintain
tissue perfusion during activity and rest. The maintenance of normal blood pressure
and tissue perfusion requires the integration of both systemic factors and local
peripheral vascular effects. Blood pressure is primarily a function of cardiac output
and systemic vascular resistance. Any condition that can have an impact on thesetwo aspects might have an impact on the blood pressure.
Hypotension is a decrease in systemic blood pressure below accepted values.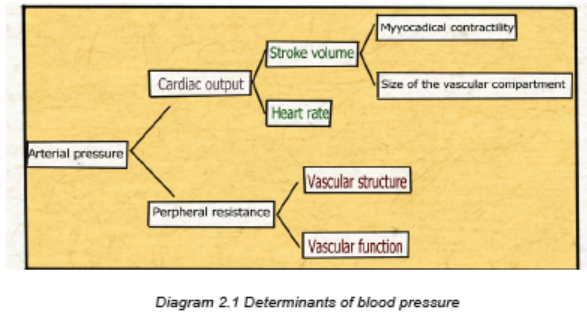
Even though there is no accepted standard hypotensive value, the blood pressure
less than systolic of 90-120mmHg/diastolic of 60-90mmHg is considered as
hypotension. The hypotension becomes a concern once pumping pressure is not
sufficient to perfuse key organs with oxygenated blood. This leads to symptomsimpacting the quality of life of a patient.
Causes and Pathophysiology
Blood pressure is determined by 2 major factors: cardiac output and total peripheral
vascular resistance. The cardiac output is determined by stroke volume and heart
rate. Therefore, any disease or pathology that impacts one or more of these factors
will induce hypotension.
Disease that reduces stroke volume or heart rate will decrease the total cardiacoutput of the heart, therefore decreasing the ability to generate blood pressure.
Some medications including diuretics, calcium channel and beta blockers can
cause hypotension by having impact on stroke volume and heart rate.
A combination of the weakened autonomic nervous system and mild hypovolemia
from dehydration causes orthostatic hypotension. When lying flat, there is equal
and smooth distribution of fluid throughout the body. However, on standing the
heart rate fails to increase appropriately and peripheral resistance fails to increase
appropriately leading to a rapid, transient decrease in blood pressure that improves
with postural changes, then classic symptoms like dizziness and syncope occur.
Certain conditions can cause prolonged periods of hypotension that can become
dangerous if left untreated: pregnancy, due to an increase in demand for blood
from both mother and the growing fetus; large amounts of blood loss through injury;
impaired circulation caused by heart attacks or faulty heart valves, weakness and
a state of shock due to dehydration, anaphylactic shock due to a severe form
of allergic reaction, infections of the bloodstream, endocrine disorders such as
diabetes, adrenal insufficiency and thyroid disease. Nutrient deficiency like lack of
vitamin B12 and folate can cause low blood pressure due to reason that nutrients
are essential to produce the red blood cells and their deficiency can lead to drop in
blood pressure levels.
Hypotension as a result of troubles of the factors determining the blood pressure,
when persistent the patient might be into different types of shock:
Distributive shock occurs as a failure of the ability to maintain total peripheral
resistance with maintained cardiac function attempting to compensate. This is
associated with anaphylactic allergic reactions and septic shock.
Cardiogenic shock is a failure to achieve sufficient cardiac output with maintained
total peripheral resistance.
Hypovolemic shock is a loss of total blood volume such that a blood pressure is
not maintained. Both cardiac output and total peripheral vascular resistance are
maintained. This is possible due to trauma with massive loss of blood, overuse of
diuretic medications with fluid volume loss via urine, burns, diarrhea and vomiting,
hemorrhage, etc.
Obstructive shock occurs with the obstruction, constriction, or compression of the
cardiovascular system such that blood flow does not efficiently occur or there is adecrease in stroke volume of the heart. This leads to drop in blood pressure.
Signs and symptoms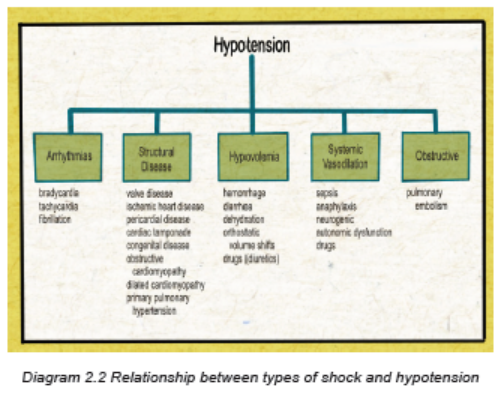
Patient with hypotension is most commonly asymptomatic. The chronic asymptomatic
hypotension isn’t usually harmful. But there are possibilities that sudden drop in
blood pressure may develop several health problems. The most common symptoms
are lightheadedness or dizziness. In extreme low blood pressures, syncope may
occur. Other symptoms are possible which typically begin from the underlying
etiology rather than hypotension itself. They may include chest pain, shortness of
breath, irregular heartbeat, headache, fatigue and weakness, pale skin color, rapid
breathing, blurred vision, fainting when having syncope, nausea, rapid pulse rate,etc.
Investigations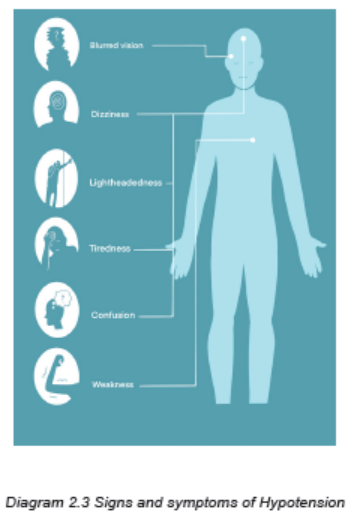
The investigations to be requested depend on the suspected cause. Basic lab work
including complete blood count (CBC), cardiac enzymes, renal function tests (urea
and creatinine), liver function tests, blood smear for malaria, blood sugar levels,
electrolytes (sodium, potassium, chloride, calcium, etc). If a patient present signs
and symptoms of shock, all these investigations must be ordered among others:
chest x-ray, electrocardiogram, blood culture, urine culture, ultrasound of the heart,
chest computerized tomography scan with angiography, etc).
Adequate Medical diagnosis
The diagnosis of hypotension requires relying on clinical manifestations supported
by laboratory and imaging investigations, and hemodynamic findings. Imaging or
hemodynamic indices of low cardiac output or systemic vascular resistance are not
diagnostic but may help to classify hypotension.
Treatment plan
Asymptomatic hypotension patient should not receive extreme interventions.
However, if symptoms are present, the treatment of hypotension should focus on
reversing the underlying etiology. The management must focus on:
• Patients should be assessed (monitoring of all vital signs) for possible need
for an immediate intervention so that lifesaving therapies can be administered
very early. After immediate stabilization, the comprehensive physical
examination must be followed.
• The airway should be stabilized and adequate intravenous access secured
so that patients can be immediately treated with intravenous fluids to restore
adequate tissue perfusion. The first priorities must be focused on the airway
and breathing with oxygen and/or mechanical ventilation, when necessary;
and insertion of intravenous catheter and IV fluids (Normal saline or Ringer
lactate) must be initiated to restore adequate tissue perfusion.
• Ensure the investigations needed are done to investigate the suspected
cause of hypotension
• Monitoring the inputs and outputs
• Treat underlying medical conditions, and this should include medications for
heart disease, diabetes, or infection. Patients with suspected infection (eg,
fever, hypotension, and a suspected septic source) must benefit from the
early administration of intravenous antibiotics.
• Shock-induced hypotension is the most serious form of the condition. Severe
hypotension must be treated immediately, should give IV fluids and possibly
blood products to increase the blood pressure and stabilize the vital signs and
hemodynamic status.
• Advise the patient to drink plenty of water to avoid hypotension due to
dehydration, especially if you are vomiting or have diarrhea. Staying hydrated
can also help treat and prevent the symptoms of mediated hypotension. If
you experience low blood pressure when standing for long periods, be sure
to take a break to sit down. And try to reduce your stress levels to avoid
emotional trauma.
• Treat orthostatic hypotension with slow, gradual movements. Instead of
standing up quickly, work your way into a sitting or standing position using
small movements. Avoid orthostatic hypotension by not crossing the legs
when you sit.
• Exercise regularly aiming at raising the heart rate and resistance exercises
two or three days a week.Evolution and complications
The prognosis of hypotension is very good, but symptomatic hypotension might
have variable prognosis depending on the etiology and its severity.
Some complications resulting from Hypotension are:
• Shock depending on etiology of hypotension
• Injury resulting from falls due to fainting. Falls are particularly dangerous
because they cause other secondary injuries (fractures, lacerations, wounds,
limited movements, etc.) that might have an impact on a person’s quality of
life.
• Severe hypotension deprives the body of oxygen, which can damage the
heart, brain, kidney and other organs (multiple organ dysfunction); and thiscondition can be life threatening if not immediately treated.
Self-assessment 2.1
1. What are the signs and symptoms of hypotension?
2. What are the possible causes of hypotension?
3. What are the investigations for the patient with hypotension?
4. What is the most appropriate treatment for hypotension?
CASE STUDY
Carefully read the case scenario below and answer the following
questions:
K.L., a 25 year old man, was not wearing his seat belt when he was the driver
involved in a motor vehicle crash.
K.L. was found 10 meters away from his car and was crying. His wife and daughter
were found in the car with their seat belts on. They sustained no serious injuries,
but were upset. All passengers were taken to the emergency department. He
states that he can’t breathe and cries when abdomen is palpated. His vital signs
were: temperature of 37.6oC blood pressure of 80/56 mm Hg; apical pulse 138 but
no palpable radial or pedal pulses; carotid pulse present but weak. Respiratory
rate 38 cycles/min; oxygen saturation of 86% on room air and asymmetric chest
wall movement; he had slight distended and left upper quadrant pain on the
abdomen. He had open wound of the lower left leg.
1. What is the medical condition is K.L. experiencing?
2. What clinical manifestations did he display that support your answer?
3. What would be included into this patient’s comprehensive assessment?
4. What investigations would you advise to be done to K.L to confirm the
medical condition? Justify the rationale of them.
5. What are the nursing interventions towards for K.L. medical condition?
6. After stabilization of K.L, what will be included into his medical and nursing
management?7. What are the possible complications related to K.L medical condition?
2.2 HYPERTENSION
Learning Activity 2.2
H.E. is a 45-years-old man with 88Kgs and 1.60m (obese) presented at a health
clinic and was found having the blood pressure of 170/95 mmHg (Normal BP:
90-120mmH/60-90mmHg). His father died of stroke at age 80 years; the mother
is alive but has hypertension. He states that he feels fine except the headache,
dizziness, chest pain especially during physical activities. He smokes one pack
of cigarettes daily for the past 28 years. He drinks 1-2 bottles of beer on most
Friday and Saturday nights. From the Laboratory investigations, he had full blood
count with Hb of 14mg/dl (Normal range 11-16 mg/dL), triglycerides of 350mg/
dl (Normal value: <150 mg/dL), sodium of 143 mEq/l (Normal range: 135-145
mEq/l). His care provider prescribed the hydrochlorothiazide 12.5 mg/day and
gave him the appointment to come back at clinic once a month.
1. From the case described above, what are the abnormal signs and
symptoms was he presenting?
2. What type of information you may ask the patient, family members to
guide in diagnosis?
3. What do you think is the medical condition of H.E?
4. Enumerate all risk factors that predisposed H.E for developing that
medical condition.
5. What are the investigations that have been requested to H.E?
6. What are different medical and nursing management options are effective
in managing H.E medical condition?
7. H.E. wants to know the most effective preventive strategies for lifestyles
changes to lower his blood pressure. What will be the content of lifestyles
modifications would you tell him?
8. What do you think will happen to H.E if there is poor adherence toprescribed treatment regimen?
The blood pressure reflects the ability of the arteries to stretch and fill with blood,
the efficiency of the heart as a pump, and the volume of circulating blood. Blood
pressure is affected by age, body size, diet, activity, emotions, pain, position,
gender, time of day, and disease states.
All these factors can have an impact on lowering or increasing the blood pressure.
Hypertension, or high blood pressure, is an important medical and public health
problem.There is a direct relationship between hypertension and cardiovascular disease.
Hypertension is a repeatedly elevated blood pressure exceeding the 90-120mmHg
as systolic and 60-90mmHg of diastolic pressure. When measuring the blood
pressure, we are looking for the pressure during systole and diastole, and is
expressed as a fraction. The top number is the systolic blood pressure; the bottomnumber is the diastolic blood pressure.
A. Systolic Blood Pressure
Systolic blood pressure is determined by the force and volume of blood that the left
ventricle ejects during systole and the ability of the arterial system to distend at thetime of ventricular contraction.
B. Diastolic Blood Pressure
Diastolic blood pressure reflects arterial pressure during ventricular relaxation
where the heart is being filled by blood either from his automatism functionality orfrom venous return.
Classification of blood pressure for Adults age 18 years or older
The term hypertension, sustained elevations in systolic or diastolic blood pressure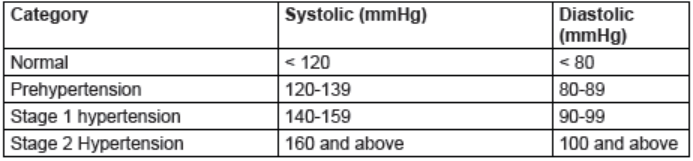
that exceed prehypertension levels, is divided into two categories:
Stage 1 hypertension: is systolic blood pressure of 140 to 159 mm Hg or a diastolic
blood pressure between 90 and 99 mm Hg.
Stage 2 hypertension: is systolic blood pressure that equals or exceeds 160 mmHg or a diastolic pressure that equals or exceeds 100 mm Hg.
Other terminologies:
When elevated blood causes a cardiac abnormality, the term hypertensive heart
disease is used. When vascular damage is present without heart involvement, theterm hypertensive vascular disease is used.
When both heart disease and vascular damage accompany hypertension, theappropriate term is hypertensive cardiovascular disease.
Causes and pathophysiology overview
A. Causes and Risk Factors
Basing on causes and risk factors, hypertension is divided into two main categories:
essential (primary; idiopathic) and secondary.
Primary (essential or idiopathic) hypertension: represent about 90-95% of all
hypertension cases. It is sustained elevated blood pressure with no known cause.
Although the exact cause of primary hypertension is unknown, there are several
contributing factors which include increased sympathetic nervous system activity,
overproduction of sodium-retaining hormones and vasoconstricting substances,
increased sodium intake, overweight, diabetes mellitus, tobacco use, and excessivealcohol consumption.
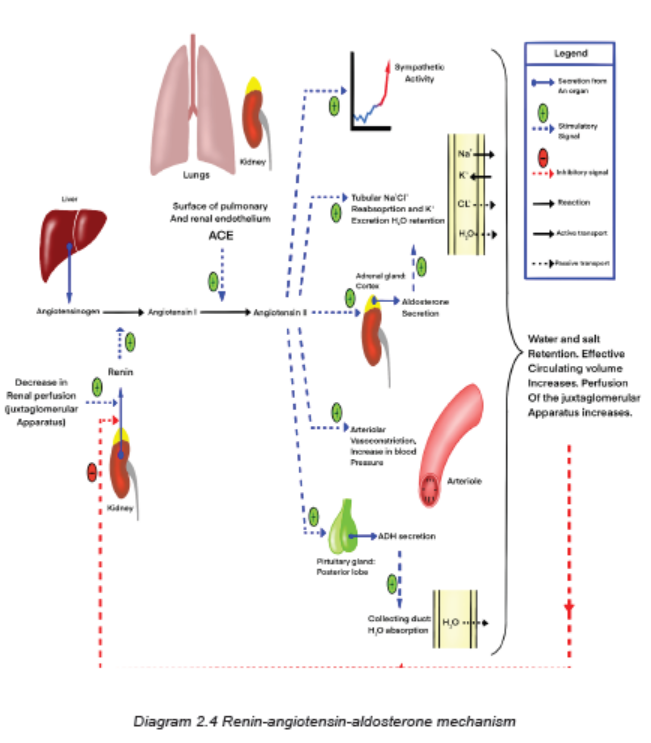
Essential hypertension also may develop from alterations in other body chemicals
such as defects in blood pressure regulation resulting from an impairment in the
renin-angiotensin-aldosterone mechanism.
Secondary hypertension: is elevated blood pressure with a specific cause that often
can be identified and corrected. It results from some other disorders such as kidney
disease, pheochromocytoma (a tumor of the adrenal medulla), hyperaldosteronism
(increased secretion of mineral corticoid by the adrenal cortex), atherosclerosis,
use of cocaine or other cardiac stimulants (e.g., weight-control drugs, caffeine), and
use of oral contraceptives. This type of hypertension accounts for 5% to 10% of all
hypertension cases. It should be suspected in people who suddenly develop high
blood pressure, especially if it is severe.
Treatment of secondary hypertension is aimed at removing or treating the underlying
cause. Secondary hypertension is a contributing factor to hypertensive crisis.
Hypertension is the most prevalent modifiable risk factor for most of cardiovascular
diseases, being more common than cigarette smoking, dyslipidemia, or diabetes,
which are the other major risk factors. Hypertension often coexists with these other
risk factors as well as with overweight/obesity, an unhealthy diet, and physical
inactivity. The presence of more than one risk factor increases the risk of adversecardiovascular events.
B. Pathophysiology Overview
Hypertension results from a sustained increase in peripheral resistance (arteriolar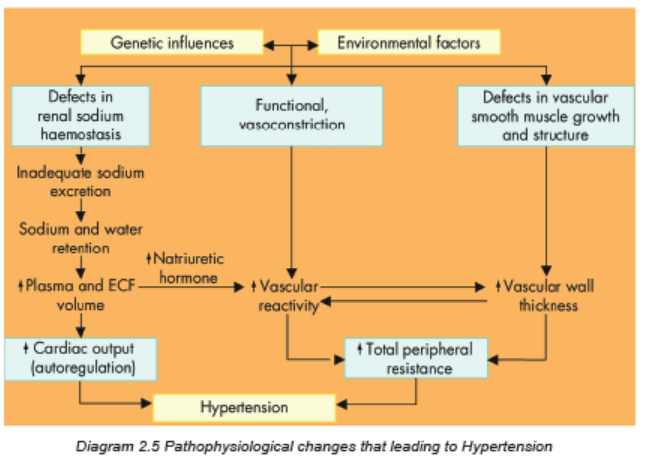
vasoconstriction), an increase in circulating blood volume, or both. Chronic
hypertension damages the walls of systemic blood vessels.Signs and symptoms
Hypertension is often called the silent killer because it is frequently asymptomatic
until it becomes severe and targeted organ disease occurs. A patient with severe
hypertension may experience a variety of symptoms secondary to the effects on
blood vessels in the various organs and tissues or to the increased workload of
the heart. These secondary symptoms include fatigue, dizziness, palpitations,
angina/chest pain, and dyspnea. Headache, nosebleeds and bleeding from other
organs might come when the blood pressure is very high. However, patients with
hypertensive crisis may experience severe headaches, dyspnea, anxiety, and
nosebleeds.
Investigations
Most hypertension is not classified as primary hypertension, testing for secondary
causes should be routinely done. Basic laboratory studies are performed to:
• Identify or rule out causes of secondary hypertension,
• Evaluate target organ disease,
• Determine overall cardiovascular risk, or
• Establish baseline levels before initiating therapy.
Basic diagnostic studies performed in a person with hypertension are the following:
1. Full blood count (FBC) to assist in establishing the baseline levels before
initiating the therapy or detect infection if any.
2. Routine urinalysis, bilirubin urea and nitrogen (BUN), liver function tests
(ASAT, ALAT) and serum creatinine levels used to screen for renal and
liver involvement and to provide baseline information about kidney and liver
function.
3. Measurement of serum electrolytes (sodium, potassium, chloride), especially
potassium, is important to detect hyperaldosteronism, a cause of secondary
hypertension.
4. Blood glucose levels (serum glucose) assist in the diagnosis of diabetes
mellitus.
5. A lipid profile (total lipids, triglycerides, cholesterol) provides information
about additional risk factors related to atherosclerosis
6. Uric acid levels establish a baseline, since the levels often rise with diuretic
therapy.
7. An electrocardiogram (ECG) provides baseline information about cardiac
status. It can identify the presence of cardiac ischemia, or previous
myocardial infarction, etc.
8. Ophtalmic examination: may reveal vascular changes in the eyes, retinal
hemorrhages, or edema of the optic nerves, known as papilledema.
Adequate medical diagnosis of HypertensionBlood pressure measurement is the initial strategy and the gold standard to
confirm the diagnosis of hypertension in most patients. In practice, blood pressure
measurement is simple and quick and should be performed at every clinical
encounter.
When hypertension is suspected or confirmed based on blood pressure readings,
a physical examination and all related investigations should be performed to
determine the extent of target-organ damage if any. Look for the presence of
cardiovascular or kidney disease, the presence or absence of other cardiovascular
risk factors, lifestyle factors that could potentially contribute to hypertension,
potential interfering substances (eg, chronic use of nonsteroidal antiinflammatory
drugs, estrogen-containing oral contraceptives) that can lead to hypertension.
The physical examination should include the funduscopic examination to evaluate
for hypertensive retinopathy and must be able to detect/predict all other possible
complications.
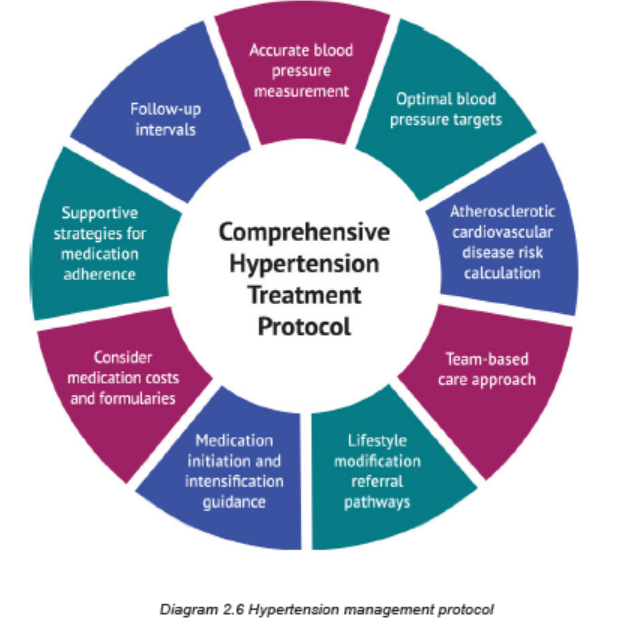
Treatment plan
Goals include achieving and maintaining normal blood pressure and reducing
cardiovascular risk and target organ disease. This treatment plan includes lifestyle
modifications and medications:
1. Weight reduction: overweight persons have an increased incidence of
hypertension and increased risk for cardiovascular diseases. When a person
decreases caloric intake, sodium and fat intake are usually also reduced.
Although reducing the fat content of the diet has not been shown to produce
sustained benefits in blood pressure control, it may slow the progress of
atherosclerosis and reduce overall cardiovascular diseases risk.
2. Dietary sodium and potassium reduction: this involves avoiding foods
known to be high in sodium and not adding salt in the preparation of foods
or at meals.
3. Avoid/Moderation of alcohol consumption,
4. Regular physical activity: physically active lifestyle is essential to promote
and maintain good health. Physical activity is more likely to be done if it is
safe and enjoyable, fits easily into one’s daily schedule, and is inexpensive.
People with hypertension must increase their physical activity. Advise
sedentary people to increase activity levels gradually.
5. Avoidance of tobacco use (smoking and chewing), and
6. Management of psychosocial risk factors.
7. Medications: the drugs currently available for treating hypertension have
two main actions: (1) they decrease the volume of circulating blood and (2)
they reduce systemic vascular resistance. The drugs used in the treatment of
hypertension include diuretics, the adrenergic inhibitors, direct vasodilators,angiotensin and renin inhibitors, and calcium channel blockers.
Key nursing interventions:
1. Health promotion: Primary prevention of hypertension is a cost-effective
approach. Current recommendations for primary prevention include lifestyle
modifications that prevent or delay the rise in blood pressure in at-risk people.
2. Blood Pressure Measurement: Initially, take the blood pressure in both
arms to note any differences. Proper size and correct placement of the blood
pressure cuff are critical for accurate measurement.
3. Screening Programs: screening programs in the community are widely
used to check individuals for high blood pressure. At the time of the blood
pressure measurement, give each person a written, numeric value of the
reading. If necessary, explain why further evaluation is needed. Effort and
resources should focus on the following: (1) controlling blood pressurein persons already identified as having hypertension; (2) identifying and
controlling blood pressure in at-risk groups such as obese people, and
relatives of people with hypertension; and (3) screening those with limitedaccess to the health care system.
4. Monitoring of Patient Adherence to medications and regimen: A major
problem in the long-term management of the patient with hypertension
is poor adherence with the prescribed regimen. The reasons for poor
adherence include inadequate patient teaching, unpleasant side effects of
drugs, return of blood pressure to normal range while on medication, lack
of motivation, high cost of drugs, lack of insurance, and lack of a trusting
relationship between the patient and the health care provider.
Also assess the patient’s diet, activity level, and lifestyle as additional
indicators of adherence. Individually assess patients to determine the
reasons why the patient is not adhering to the treatment and develop a
plan with the patient to improve adherence. The plan should be compatible
with the patient’s personality, habits, and lifestyle. Active patient participation
increases the likelihood of adherence to the treatment plan. Measures
such as including the patient in the development of a medication schedule,
selecting medications that are affordable, and involving caregivers help
increase patient adherence.
Substituting combination drugs for multiple drugs once the BP is stable may
also facilitate adherence. Combination drugs reduce the number of pills the
patient has to take each day and may reduce costs. It is important to help
the patient and caregiver understand that hypertension is a chronic illness
that cannot be cured. Emphasize that it can be controlled with drug therapy,
diet changes, physical activity, periodic follow-up, and other relevant lifestyle
modifications.Evolution and complications of hypertension
Hypertension is associated with a significant increase in risk of adverse cardiovascular
and kidney outcomes. Each of the complications is closely associated with thepresence of hypertension.
Complications of hypertension
Regardless of whether a person has essential or secondary hypertension, the
accompanying organ damage and complications are the same. Hypertension
causes the heart to work harder to pump against the increased resistance. The extra
work and the greater mass increase the heart’s need for oxygen. If the myocardium
doesn’t receive sufficient oxygenated blood, myocardial ischemia occurs and theclient experiences angina. Consequently, the size of the heart muscle increases.
When the heart no longer can pump adequately to meet the body’s metabolic needs,
heart failure occurs. In addition to its direct effects on the heart, high blood pressure
damages the arterial vascular system. It accelerates atherosclerosis. Furthermore,
the increased resistance of the arterioles to the flow of blood causes serious
complications in other body organs, including the eyes, brain, heart, and kidneys.
Hemorrhage of tiny arteries in the retina may cause marked visual disturbances
or blindness. A cerebrovascular accident (stroke) may result from hemorrhage or
occlusion of a blood vessel in the brain. Myocardial infarction (MI) may result from
occlusion of a branch of a coronary artery. Impaired circulation to the kidneys mayresult in renal failure.
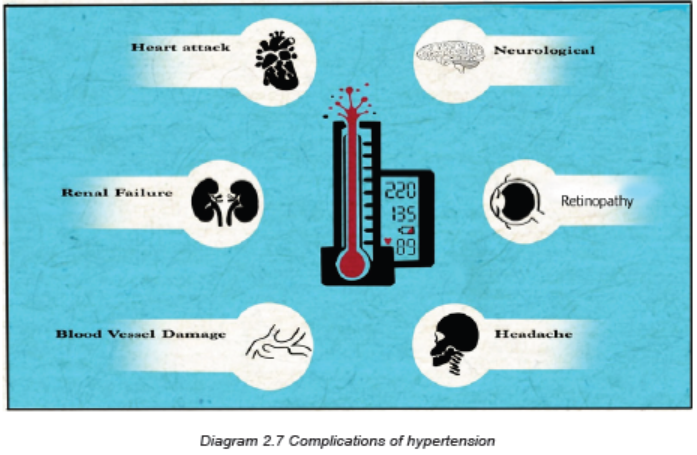
In summary, the complications of hypertension are:
– Hypertension emergency
– Atherosclerotic coronary artery disease
–Myocardial ischemia/ infarction
– Heart failure
– Renal Failure
– Stroke/ Cerebral hemorrhage/ Cerebral ischemia
– Aortic aneurysm
– Retinal vascular sclerosis– Gangrene of extremities
Hypertensive Crisis:
Hypertensive crisis is a term used to indicate either a hypertensive urgency or
emergency. This is determined by the degree of target organ disease and how
quickly the blood pressure must be lowered.
A hypertensive emergency develops over hours to days. It is a situation in which
a patient’s blood pressure is severely elevated (often above 220/140 mm Hg) with
clinical evidence of target organ disease. It can cause encephalopathy, intracranial
or subarachnoid hemorrhage, acute left ventricular failure, myocardial infarction,
renal failure, dissecting aortic aneurysm, and retinopathy.
Hypertensive urgency develops over days to weeks. This is a situation in which a
patient’s blood pressure is severely elevated (usually above 180/110 mm Hg), but
there is no clinical evidence of target organ disease.
Prompt recognition and management of hypertensive crisis are essential to decrease
the threat to organ function and life. Hypertensive crisis occurs more often in patients
with a history of hypertension who have not adhered to their medication regimens
or who have been under-medicated. In such cases, rising blood pressure is thoughtto trigger endothelial damage and the release of vasoconstrictor substances.
Clinical Manifestations
A hypertensive crisis is often manifested as hypertensive encephalopathy, a
syndrome in which a sudden rise in blood pressure is associated with severe
headache, nausea, vomiting, seizures, confusion, and coma. Patients can have
chest and back pain, dyspnea, and possibly reduced or absent pulses in theextremities.
Management of Hypertensive crisis:
Blood pressure level alone is a poor indicator of the seriousness of the patient’s
condition. It is not the major factor in deciding the treatment for a hypertensive
crisis. The link between elevated blood pressure and signs of new or progressive
target organ disease determines the seriousness of the situation. Hypertensive
crisis require hospitalization, intravenous administration of antihypertensive drugsand intensive care monitoring.
Self-assessment 2.2
1. What is included in the correct technique for BP measurements?
a. Always take the BP in both arms.
b. Position the patient supine for all readings.
c. Place the cuff loosely around the upper arm.d. Take readings at least two times at least 1 minute apart.
2. Which BP-regulating mechanism(s) can result in the development of
hypertension if defective (select all that apply)?
a. Release of norepinephrine
b. Stimulation of the sympathetic nervous system
c. Stimulation of the parasympathetic nervous systemd. Activation of the renin-angiotensin-aldosterone system
3. While obtaining subjective assessment data from a patient with
hypertension, the nurse recognizes that a modifiable risk factor for the
development of hypertension is:
a. A low-calcium diet.
b. Excessive alcohol consumption.
c. A family history of hypertension.d. Consumption of a high-protein diet.
4. When obtaining a health history from a client, which finding is most
suggestive that the client is hypertensive? (select all that apply)
a. The client experiences occasional heart palpitations associated with chestpain.
b. The client has experienced fainting episodes.
c. The client has difficulty sleeping all night.
d. The client is having pounding headache
5. Basing on the causes and risk factors, differentiate briefly the essentialand secondary hypertension.
6. What are two physiologic components that determine blood pressure?
7. You are caring for P.N., a 46-year-old man with a history of poorly
controlled hypertension and chronic kidney disease. You note that he is
taking the antihypertensive medications. He tells you that he can no longer
live with the side effects of these drugs (e.g., fatigue, dry mouth, erectile
dysfunction). He states that he wants to stop taking the medications. He
believes that if he changes his lifestyle by reducing salt from his diet,
losing weight, and beginning exercise, he can control his hypertension.
a. Explain different lifestyle changes you would advise P.N. to practice in
order to be able to control her hypertension.
b. P.N. must continue to take her medications. Justify the importance ofadherence to hypertensive medications.
8. List all essential needed investigations and their rationale in themanagement of hypertension.
9. What are the elements that constitute the nursing management of theclient with hypertension?
10. List all potential complications of uncontrolled hypertension.
11. Which manifestation is an indication that a patient is having a hypertensiveemergency?
a. Symptoms of a stroke with an elevated BP
b. A systolic BP >220 mm Hg and a diastolic BP >140 mm Hg
c. A sudden rise in BP accompanied by neurologic impairment
d. A severe elevation of BP that occurs over several days or weeks
12. Discuss the medical and nursing management of the client withHypertensive crisis.
Case study:
Carefully read the case scenario below and answer the followingquestions:
K.J. is a 73-year-old woman with no history of hypertension. She came to the
clinic for dizziness and chronic headache. She says she has gained 10Kgs over
the past year. Her father died from stroke. She has never smoked and uses no
alcohol. She takes one medication (multivitamin). She eats a lot of carbohydrates
food and does not do exercise because she feels tiredness whenever she wants
to do exercises. Her vital parameters are: height: 168 cm, weight: 86 kgs, BP:
190/82 mm Hg Pulse: 82 beats per minute, Temperature: 36.2 degree Celsius,
Respiratory rate: 18 cycles per minute. During her physical examination there
are no abnormalities at other systems except BMI and blood pressure that are
high. She was primarily diagnosed to have primary hypertension while waiting
for additional investigations.
1. What are the contributing factors to the development of hypertension was
K.J. presenting?
2. What additional information would you need to collect that will help in
deciding about the medical condition of K.J?
3. From her condition, what would you advise as investigations to be
requested that might be helpful in deciding further management of K.J
medical condition? Justify the rationale.
4. Discuss all aspects that might be included into her medical and nursing
management.
5. If drug therapy became necessary to treat K.J.’s hypertension, give three
examples of antihypertensive drugs that would be indicated based on herclinical status?
6. Explain the different lifestyles changes would you recommend to K.J.?7. If her condition is not well managed, what do you expect as complications?
2.3 STROKE
Learning Activity 2.3
Observe the image below and read carefully the scenario below andanswer the questions that follow:

Figure2.5 Patient with left side body functional impairment.
N.J. is a 66-years-old woman who lives in Kigali. She arrives in the emergency
department at CHUK after falling down during the night when she tried to get
up to go to the bathroom. She had history of high blood pressure. She states
that she fell because she could not control her left leg. Her husband brought
her to the hospital, but states that it was not possible for him to get his wife to
the car alone because most of her body parts were not functioning and were
weak. When arrived at CHUK, she was having paralysis of entire left side of the
body involving left arm and left leg, inability to sit and stand alone, general body
weakness, and unable to speak.
1. Referring to the above situation, what might be the possible cause for her
left side body functional impairment and general body weaknesses?
2. What are other additional information you would ask to guide in diagnosing
the medical condition that patient has?
3. In general, what are the causes and risk factors do you think can be at the
origin of that medical problem?
4. What investigations might you expect to be ordered in order to confirm
the medical diagnosis?
5. What will be included into the comprehensive physical assessment of
N.J?
6. What is the medical diagnosis is N.J presenting?
7. What should be included into the treatment plan for N.J?
8. Identify all possible complications that might result from the medicalcondition of N.J.?
the brain, with stroke being the most frequent manifestation of cerebrovascular
disease.
Brain and cerebral nerve cells are extremely sensitive to a lack of oxygen; if they
are deprived of oxygenated blood for 3 to 7 minutes, both the brain and nerve cells
begin to die. Prolonged interruption in the flow of blood and oxygen through one of
the arteries supplying the brain leads to stroke or cerebrovascular accident.
A stroke also called cerebrovascular accident occurs when the blood supply to parts
of the brain is interrupted or reduced, preventing brain tissue from getting oxygen
and nutrients. A stroke is a medical emergency, and prompt treatment is crucial.
Early recognition and action can reduce brain damage and further complications.
Causes, risks factors and pathophysiology
Genetic risk factors (among non-modifiable risk factors) are important in the
development of all vascular diseases, including stroke. A person with a family
history of stroke has an increased risk of having a stroke. Genes encoding products
involved in lipid metabolism, thrombosis, and inflammation are believed to be
potential genetic factors for stroke. Modifiable risk factors are those that can be
altered through lifestyle changing and medical treatment, thus reducing the risk ofstroke.
Cerebrovascular disease arises from pathological processes in blood vessels of
Modifiable risk factors for hypertension are: metabolic syndrome, heart disease,
heavy alcohol consumption, poor diet, drug abuse, sleep apnea, obesity, physicalinactivity and smoking.
Non modifiable risk factors for hypertension are: age, gender, race, heredity/family history.
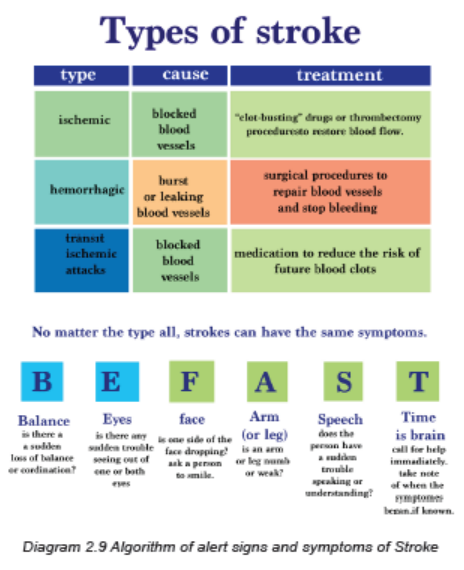
Strokes are classified on the basis of underlying pathophysiologic findings: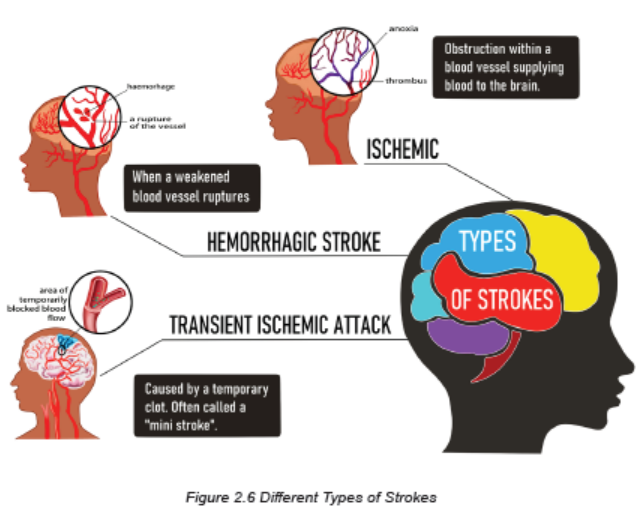
A. Ischemic (represent 80% of all Strokes): mainly due to thrombus, emboli,
systemic hypo perfusion, and atherosclerosis. When ischemic strokes occur,
glucose and oxygen to brain cells are reduced. The reduced glucose quickly
depletes the stores of adenosine triphosphate (ATP), resulting in anaerobic
cellular metabolism and the accumulation of toxic products such as lactic
acid. Although some brain cells die from anoxia, the lack of oxygen destroysadditional brain cells by a secondary mechanism
1. Atherosclerotic: Fatty streak is covered by collagen, forming a fibrous
plaque that appears grayish or whitish, that result in narrowing of vessel
lumen, and continued inflammation can result in plaque instability, ulceration,
and rupture, platelets accumulate and thrombus forms, Increased narrowingor total occlusion of lumen.
2. Systemic hypoperfusion: Reduced blood flow is more global in patients
with systemic hypoperfusion and does not affect isolated regions. The
reduced perfusion can be due to cardiac pump failure caused by cardiac
arrest or arrhythmia, or to reduced cardiac output related to acute myocardial
ischemia, pulmonary embolism, pericardial effusion, or bleeding. Hypoxemia
may further reduce the amount of oxygen carried to the brain.
3. Thrombotic stroke: Thrombosis occurs in relation to injury to a blood
vessel wall and formation of a blood clot that result to narrowing of the blood
vessel. It is the most common cause of stroke. The thrombotic strokes are
associated with hypertension or diabetes mellitus, both of which accelerate
atherosclerosis.
4. Embolic stroke: Occurs when an embolus lodges in and occludes a
cerebral artery. It is the second most common cause of stroke. Most emboli
originate in the endocardial (inside) layer of the heart, with plaque breaking
off from the endocardium and entering the circulation. The embolus travels
upward to the cerebral circulation and lodges where a vessel narrows.
Patient with an embolic stroke commonly has a rapid occurrence of severe
clinical symptoms but warning signs are less common with embolic than with
thrombotic stroke. Onset of embolic stroke is usually sudden and may or
may not be related to activity. Patient usually remains conscious, althoughmay have a headache.
B. Hemorrhagic (represent 20% of all Strokes): due to intracerebral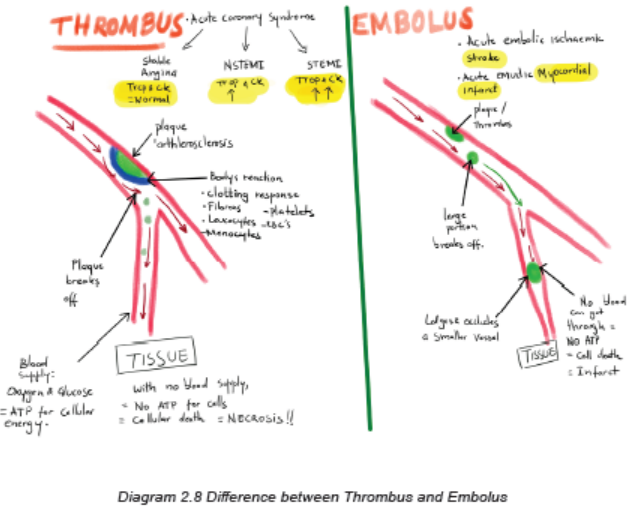
hemorrhage (ICH) or subarachnoid hemorrhage (SAH). Hypertension is
the most important cause. This type of stroke results from bleeding into the
brain tissue itself or into the subarachnoid space or ventricles. Hemorrhage
commonly occurs during periods of activity. It often has a sudden onset of
sympt oms, with progression over minutes to hours because of ongoing
bleeding.
C. Transient ischemic attack (TIA): It is a transient episode of neurologic
dysfunction caused by focal brain, spinal cord, or retinal ischemia, without
acute infarction of the brain. The symptoms last less than one hour and most
TIAs resolve. We need to encourage patients to consult a health facility at any
symptom onset/occurrence since once a TIA starts, one does not know if it
will persist and become a true stroke, or if it will resolve.
Clinical Manifestations
Primary assessment focuses on cardiac and respiratory status (ABC: Airway,
Breathing, Circulation) and neurologic assessment. If the patient is stable, the
history is obtained as follows: (1) description of the current illness with attention to
initial symptoms, particularly symptom onset and duration, nature (intermittent or
continuous), and changes; (2) history of similar symptoms previously experienced;
(3) current medications; (4) history of risk factors and other illnesses such as
hypertension; and (5) family history of stroke or cardiovascular diseases. This
information is gained through an interview of the patient, family members, significant
others, and/or caregiver.
Secondary assessment includes a comprehensive neurologic examination of
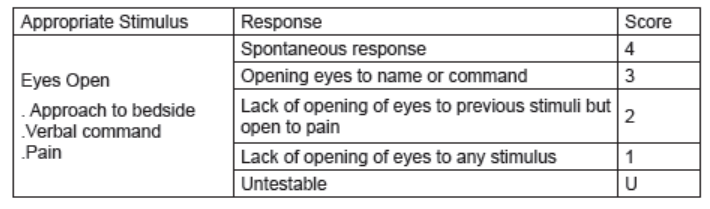
the patient. This includes (1) level of consciousness (using the Glasgow Coma
Scale), (2) cognition; (3) motor abilities; (4) cranial nerve function; (5) sensation; (6)
proprioception; (7) cerebellar function; and (8) deep tendon reflexes.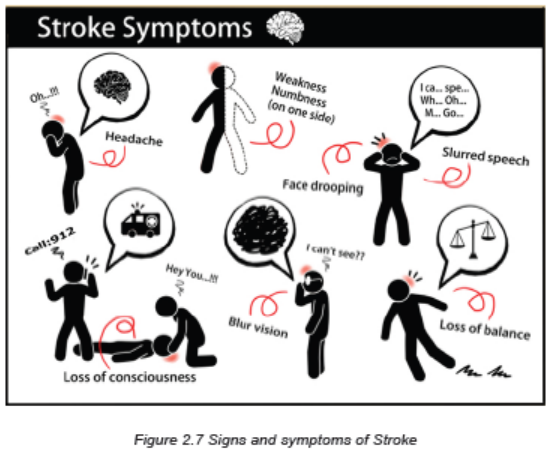
Motor deficits are the most obvious effect of stroke. Motor deficits include impairment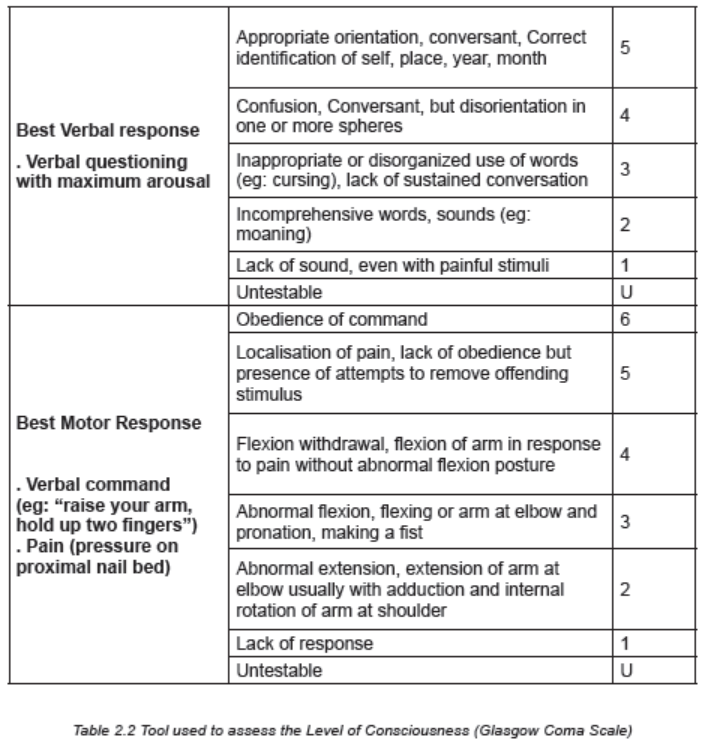
of (1) mobility, (2) respiratory function, (3) swallowing and speech, (4) gag reflex,and (5) self-care abilities.
Investigations
When manifestations of a stroke occur, diagnostic studies are done to:
• Confirm that it is a stroke and not another brain lesion and
• Identify the likely cause of the stroke.
Important diagnostic tools for patients who have experienced a stroke are a non
and/or contrasted computed tomography scan (CT Scan) or magnetic resonanceimaging (MRI). These tests can rapidly distinguish between ischemic and
hemorrhagic stroke and help determine the size and location of the stroke.
The following Blood tests are also done to help identify conditions contributing to
stroke and to guide in deciding the management: Complete blood count (including
platelets, coagulation studies: prothrombin time, troponin, international normalization
rate: INR), Electrolytes (sodium, potassium, calcium, chloride, etc), Blood glucose
levels, Renal function tests (urea and creatinine), and Liver function tests (ASAT,
ALAT), Lipid profile, Cerebrospinal fluid analysis. The Electrocardiogram can alsobe performed.
Adequate Medical Diagnosis
Stroke is diagnosed through several technics: history taking, and comprehensive
physical exam that include the neurological examination. Imaging investigations like
CT scan and MRI are helpful. These imaging are helpful in determining the extent
of injury and location, therefore determining the causes and subtypes. Laboratory
investigations are needed to look for other factors that might be associated withstroke.
Treatment Plan
Hypertension is the single most important modifiable risk factor, therefore it needsto be detected early and adequately treated. The goals for collaborative and
comprehensive management of stroke are:
1. To prevent secondary brain injury (intracranial hypertension, hematoma
expansion, elevated intracranial pressure, seizures, herniation )
2. To maintain and secure the airways (due to paralysis of the pharynx
muscles),
3. To provide general body support (vital signs, fluid and electrolyte balance,
hemodynamic patient monitoring: all Systems to be cared for) and
4. To anticipate the occurrence of complications (atelectasis, aspiration
pneumonia, airway obstruction that might require tracheal intubation and
mechanical ventilation), and plan for Respiratory system management asPriority.
Interventions
While caring for patient with stroke, the care providers must ensure the following:
A. Cardiac and Respiratory System:
• Ensure patent airway, Call for resuscitation team/shout for help, Perform
pulse oximetry (SP02) and oxygen therapy as urgency to maintain adequate
oxygenation.
• Obtain IV access.
• Monitor and maintain normal BP and other vital signs, and watch for
hypertension post stroke (Continuous effective monitoring of BP). Eligible to
thrombolysis: BP≤ 185/110 mmHg before and 180/105 mmHg after for at
least 24 hours. Blood pressure should not be treated acutely for patients with
ischemic stroke who are not eligible to thrombolysis, except Hypertension
is extreme, BP >220/120 mmHg. Intravenous agents are recommended for
blood pressure lowering, labetalol& nicardipine as first line , IV Nitroprusside
as second-line therapy.
• Obtain CT scan or MRI immediately, Perform baseline laboratory tests (FBC,
Troponin, INR(International Normalization Rate), etc).
• Proper Positioning of patient head: The appropriate position of the patient
and the head of bed should be respected to prevent the risk of elevated
intracranial pressure and aspiration. The head in neutral alignment with the
body elevation of the head of the bed to 30 degrees are recommended if no
symptoms of shock or injury occur.
• Implement anti-seizure precautions and Anticipate thrombolytic therapy for
ischemic stroke.
• Adjusting fluid intake to the individual needs of the patient, Regulating IV
infusions and calculating intake and output, noting imbalance. Fluid andelectrolyte balance must be controlled carefully: Adequate hydration promotes
perfusion and decreases further brain injury. Adequate fluid intake during
acute care via oral, intravenous (IV), or tube feedings should be 1500 to 2000
mL/day. Over hydration may compromise perfusion by increasing cerebral
edema.
• Monitoring lung sounds for crackles and rhonchi (pulmonary congestion) and
monitoring heart sounds for murmurs.
• Monitoring and Management of blood glucose levels: Hypoglycemia can
cause focal neurologic deficits mimicking stroke, therefore check the blood
sugar and rapidly correct low serum glucose (<60 mg/dL /3.3 mmol/L).
Hyperglycemia in diabetic patients or stress hyperglycemia is associated with
poor functional outcome. Hyperglycemia may augment brain injury by several
mechanisms including increased tissue acidosis from anaerobic metabolism,
free radical generation, and increased blood brain barrier permeability.
• Check for fever and other signs and symptoms of infection: Meningitis,
subdural empyema, brain abscess, and infective endocarditis need to be
excluded as the etiology of fever if acute neurologic deterioration
• After stroke, patient is at risk for deep vein thrombosis related to immobility,
loss of venous tone, and decreased muscle pumping in leg, most effective
prevention is keeping the patient moving, and encourage ambulation.
B. Musculoskeletal and Integumentary system: Goal is to maintain optimal
function:
• Prevention of joint contractures and muscular atrophy: Range-of-motion
exercises and positioning are important. Paralyzed or weak side needs
special attention when positioning.
• Avoidance of pulling the patient by the arm to avoid shoulder displacement
• Good skin hygiene, Early mobility, ambulation and Change position of the
patient because the stroke patient is susceptible to skin breakdown related to
Loss of sensation, Decreased circulation, Immobility compounded by patient
age, poor nutrition, dehydration, oedema, and incontinence
C. Gastrointestinal system:
• Patients may be placed on stool softeners.
• Physical activity promotes bowel function.
• Implement a bowel management program for problems with bowel control,
constipation, incontinence
D. Urinary system:
• Promote normal bladder function.
• Avoid the use of indwelling catheters as much as you can.
E. Nutrition:
• Nutritional needs require quick assessment and treatment.
• May initially receive IV infusions to maintain fluid and electrolyte balance
• May require nutritional support
• First feeding should be approached carefully, and always test swallowing,
chewing, gag reflex, before beginning oral feeding.
• Feedings must be followed by oral hygiene.
• High-fiber diet and adequate fluid intake
F. Antiplatelet drugs are usually the chosen treatment: Aspirin is the most
frequently used as antiplatelet agent. Recombinant Tissue plasminogen
activator: to reestablish blood flow from blocked blood vessel. To be given
3 to 4.5 hours after signs and symptoms of ischemic stroke. Determining
eligibility to IV thrombolytic therapy for patients with acute ischemic stroke: IV
Alteplase is first-line therapy, to be initiated within 4.5 hours of symptom onset
or the time last known to be well. Oral anticoagulation using warfarin is the
treatment of choice for individuals with atrial fibrillation.
G. Surgical interventions might be needed depending on medical diagnosis
and goal of treatment (eg: hematoma evacuation, removing the plaque,opening the blocked artery, anastomosis, etc).
Preventive Strategies
1. Teaching patients and families about all Preventive measures (reduce salt
and sodium intake, Maintain a normal body weight, Maintain a normal blood
pressure, Increase level of physical exercise, Avoid cigarette smoking or
tobacco products, Limit consumption of alcohol to moderate levels, Follow a
diet that is low in saturated fat, total fat, and dietary cholesterol and high in
fruits and vegetables).
2. Teaching patients and families about signs and symptoms, stroke
pathophysiology, complications and when to seek health care for symptoms.
3. Education about hypertension control and adherence to medication,
particularly in persons with known risk factors.
4. Education and management of modifiable risk factors to change lifestyle:
Patients with known risk factors (Diabetes mellitus, Hypertension, Obesity,
High serum lipids, Cardiac dysfunction, etc) require close and effective
management.
Evolution and Complications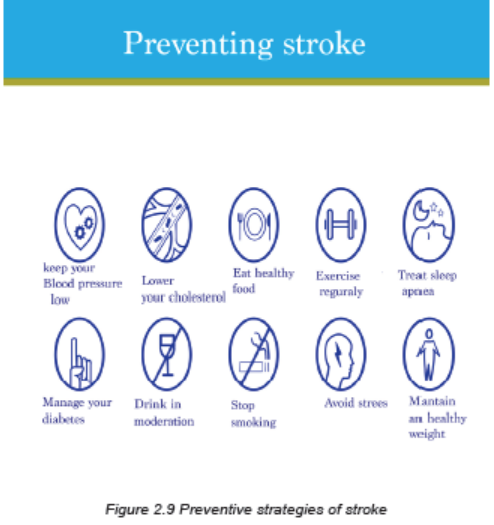
Stroke is a significant cause of death and disability. The highest incidence of stroke
occurs among older adults and the people with comorbidities. Stroke can result
in a profound disruption in the life of a person. The ability to perform activities of
daily living may require many adaptive changes because of physical, emotional,
perceptual, and cognitive deficits. There is need to assist the patient and caregiver
in the transition through acute phase of care, rehabilitation, long-term care, and
home care. The needs of the patient, the caregiver, and the family involvement
require ongoing health education.
The most common complications of stroke are:
• Brain edema: swelling of brain post stroke
• Pneumonia: causes breathing problems
• Swallowing problems: that can potentially cause the aspiration pneumonia
• Blood clot or deep vein thrombosis: related to limited range of motion/physical
activity
• Aphasia and speech disorders• Depression and other mood disorders, chronic headache,etc
Self-assessment 2.3
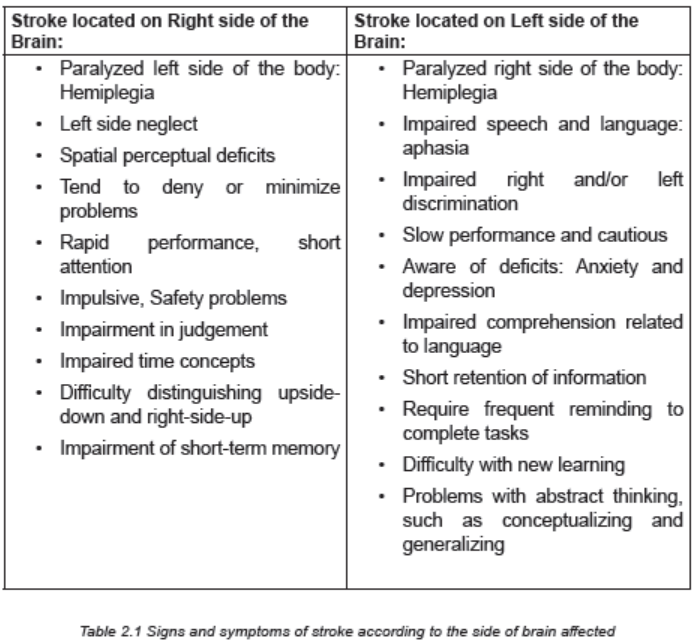
1. Indicate whether the following manifestations of a stroke are more likely
to occur with right brain damage (R) or left brain damage (L).
a. Aphasia
b. Impaired judgment
c. Quick, impulsive behavior
d. Inability to remember words
e. Neglect of the left side of the body
f. Hemiplegia of the right side of the body
2. Four days following a stroke, a patient is to start oral fluids and feedings.
Before feeding the patient, what should the nurse do first?
a. Check the patient’s gag reflex.
b. Order a soft diet for the patient.
c. Raise the head of the bed to a sitting position.
d. Evaluate the patient’s ability to swallow small amounts of crushed ice or
ice water.
3. What is the priority intervention in the emergency department for the
patient with a stroke?
a. Intravenous fluid replacement
b. Administration of osmotic diuretics to reduce cerebral edema
c. Initiation of hypothermia to decrease the oxygen needs of the brain
d. Maintenance of respiratory function with a patent airway and oxygen
administration
4. What is the difference between ischemic and hemorrhagic stroke?
5. Describe different criteria that are assessed to determine the level of
consciousness using Glasgow coma scale
6. List the preventive strategies of stroke for (1) healthy people and
overweight people, and (2) patient with hypertension and diabetes.
7. What therapeutic options are available for the patient with a hemorrhagicand ischemic stroke?
Case studyCarefully read the case study below and answer the following questions:
R.C., a 52-year-old married man, was admitted to the hospital with unconscious
after his family find that he could not wake up in the morning. He was accompanied
by his wife and one daughter 20 years. He had history of hypertension with poor
adherence on captopril and had overweight. He complained of severe headache
associated with epistaxis the day before he became unconsciousness. Vital
signs at arrival at hospital: BP 198/102 mmHg, RR 16 cycles/minute, HR 74
bpm, Temp 36.7°C, SPo2: 82% on room air. His Glasgow Coma Scale score:
9/15. He is not able to open the mouth, unable to sit or stand without support,and has right sided hemiplegia. Blood sugar: 94 mg/dl.
Questions:
1. What will be additional information you will ask the family members toguide in deciding about the diagnosis and the management?
2. What investigations will you advise to be requested to determine the
cause of R.C. unconsciousness? What is the rationale of requestingthose investigations?
3. List all nursing interventions that have the highest priority for R.C. at thisstage of his illness?
4. What should the family be told to expect in terms of R.C. medicalcondition
2.4 END UNIT 2 ASSESSMENT
End of unit 2 assessment
SECTION A: Short Answer Questions
1. Cardiac output is the product of ……………………….. multiplied
by…………………………..
2. Prolonged hypertension can cause significant damage to these four
“target organs”: A)………………… B)…………………………….,
C)…………………………, and D)………………..
3. Discuss in detail several hypotheses about the pathophysiologic basis for
elevated blood pressure.
4. Explain how lifestyle changes and medications can control, not cure,
hypertension.
5. Compare and contrast the different medications used to treat hypertension
and the associated nursing considerations.
6. Compare and contrast a hypertensive crisis with a hypertensive
emergency.
7. List four non modifiable risk factors for stroke.
8. Compare the etiology and symptoms of two types of stroke: ischemic
stroke and hemorrhagic stroke.
9. Describe the focus of nursing interventions when helping a patient recoverfrom an ischemic stroke.
10. Identify the significance of the following laboratory test results when foundin patients with hypertension:
11. A 42-year-old man has been diagnosed with primary hypertension with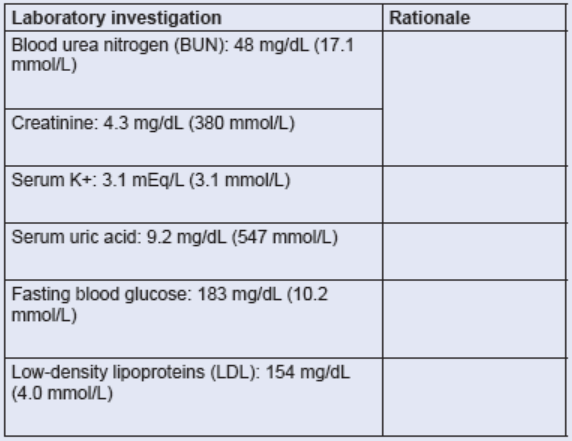
an average blood pressure of 162/92 mm Hg on three consecutive clinic
visits. What are four priority lifestyle modifications that should be exploredin the initial treatment of the patient?
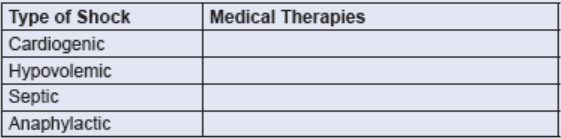
12. Identify two medical therapies that are specific to each of the followingtypes of shock.
SECTION B: Multiple Choice Questions
1. After taking vital signs, you write down your findings as temperature of
36.6 degree Celsius, Pulse of 66 beats per minute, respiratory rate of 18
cycles per minutes, Blood Pressure of 124/82 mmHg. Which of thesenumbers represents the systolic blood pressure?
a. 36.6
b. 124
c. 82
d. 66
2. Stroke volume of the heart is determined by:
a. The degree of cardiac muscle strength (pre-contraction).
b. The intrinsic contractility of the cardiac muscle.
c. The pressure gradient against which the muscle ejects blood duringcontraction.
d. All of the above factors.
3. The most important factor in regulating the caliber of blood vessels, whichdetermines resistance to flow, is:
a. Hormonal secretion.
b. Independent arterial wall activity.
c. The influence of circulating chemicals.
d. The sympathetic nervous system.
4. Stage 1 hypertension is defined as persistent blood pressure levels in
which the systolic pressure is higher than …………. and the diastolic ishigher than …………….
a. 110/60 mm Hg
b. 120/70 mm Hg
c. 130/80 mm Hgd. 140/90 mm Hg
5. Georgia, a 30-year-old woman, is diagnosed as having secondary
hypertension when serial blood pressure recordings show her average
reading to be 170/100 mm Hg. Her hypertension is the result of renal
dysfunction. The kidneys help maintain the hypertensive state in essential
hypertension by:
a. Increasing their elimination of sodium in response to aldosterone secretion.
b. Releasing renin in response to decreased renal perfusion.
c. Secreting acetylcholine, which stimulates the sympathetic nervous system
to constrict major vessels.
d. Doing all of the above.
6. The first priority of treatment for a patient with altered level of consciousness
is:
a. Assessment of pupillary light reflexes.
b. Determination of the cause.
c. Positioning to prevent complications.
d. Maintenance of a patent airway.
7. The degree of neurologic damage that occurs with an ischemic stroke
depends on the:
a. Location of the lesion.
b. Size of the area of inadequate perfusion.
c. Amount of collateral blood flow.
d. Combination of the above factors.
8. The initial diagnostic test for a stroke, usually performed as emergency is:
a. 12-lead electrocardiogram.
b. Carotid ultrasound study.
c. Non contrasted computed tomogram.
d. Transcranial doppler flow study.
9. How is secondary hypertension differentiated from primary hypertension?
a. Has a more gradual onset than primary hypertension
b. Does not cause the target organ damage that occurs with primaryhypertension
c. Has a specific cause, such as renal disease, that often can be treated by
medicine or surgery
d. Is caused by age-related changes in BP regulatory mechanisms in people
over 65 years of age
10. What is most organ damage in hypertension related to?
a. Increased fluid pressure exerted against organ tissue
b. Atherosclerotic changes in vessels that supply the organs
c. Erosion and thinning of blood vessels from constant pressure
d. Increased hydrostatic pressure causing leakage of plasma into organ
interstitial spaces
11. A 38-year-old man is treated for hypertension with triamterene and
hydrochlorothiazide and metoprolol. Four months after his last clinic
visit, his blood pressure returns to pretreatment levels and he admits he
has not been taking his medication regularly. What is the nurse’s best
response to this patient?
a. “Try always to take your medication when you carry out another daily
routine so you do not forget to take it.”
b. “You probably would not need to take medications for hypertension if you
would exercise more and stop smoking.”
c. “The drugs you are taking cause sexual dysfunction in many patients. Are
you experiencing any problems in this area?
d. “You need to remember that hypertension can be only controlled with
medication, not cured, and you must always take your medication.”
12. What does the nursing responsibility in the management of the patient
with hypertensive urgency often include?
a. Monitoring hourly urine output for drug effectiveness
b. Titrating IV drug dosages based on BP measurements every 2 to 3 minutes
c. Providing continuous electrocardiographic (ECG) monitoring to detect side
effects of the drugs
d. Instructing the patient to follow up with a health care professional within 24hours after outpatient treatment
13. What is included in the correct technique for blood pressure
measurements?
a. Always take the BP in both arms.
b. Position the patient supine for all readings.
c. Place the cuff loosely around the upper arm.
d. Take readings at least two times at least 1 minute apart.
14. A patient comes to the emergency department immediately after
experiencing numbness of the face and an inability to speak but while
the patient awaits examination, the symptoms disappear and the patient
requests discharge. Why should the nurse emphasize that it is important
for the patient to be treated before leaving?
a. The patient has probably experienced an asymptomatic lacunar stroke.
b. The symptoms are likely to return and progress to worsening neurologic
deficit in the next 24 hours.
c. Neurologic deficits that are transient occur most often as a result of small
hemorrhages that clot off.
d. The patient has probably experienced a transient ischemic attack (TIA),
which is a sign of progressive cerebrovascular disease.
15. What are characteristics of a stroke caused by an intracerebral hemorrhage
(select all that apply)?
a. Carries a poor prognosis caused by rupture of a vessel
b. Strong association with hypertension
c. Commonly occurs during or after sleep
d. Creates a mass that compresses the brain
16. A patient is admitted to the hospital with a left hemiplegia. To determine
the size and location and to ascertain whether a stroke is ischemic or
hemorrhagic, the nurse anticipates that the health care provider will
request (select all that apply):
a. Lumbar puncture.
b. Cerebral arteriogram.
c. Magnetic resonance imaging (MRI).d. Computed tomography (CT) scan with or without contrast.
17. Which intervention should the registered nurse delegate to the associate
nurse when caring for a patient following an acute stroke?
a. Assess the patient’s neurologic status.
b. Assess the patient’s gag reflex before beginning feeding.
c. Administer ordered antihypertensives and platelet inhibitors.
d. Teach the patient’s caregivers strategies to minimize unilateral neglect.
18. What is the key factor in describing any type of shock?
a. Hypoxemia
b. Hypotension
c. Vascular collapse
d. Inadequate tissue perfusion
19. Which hemodynamic monitoring description of the identified shock is
accurate?
a. Tachycardia with hypertension is characteristic of neurogenic shock.
b. In cardiogenic shock the patient will have an increased pulmonary artery
wedge pressure (PAWP) and a decreased cardiac output (CO).
c. Anaphylactic shock is characterized by increased systemic vascular
resistance (SVR), decreased CO, and decreased PAWP.
d. In septic shock, bacterial endotoxins cause vascular changes that result in
increased SVR and decreased CO.
20. As the body continues to try to compensate for hypovolemic shock, there
is increased angiotensin II from the activation of the renin-angiotensinaldosterone
system. What physiologic change occurs related to the
increased angiotensin II?
a. Vasodilation
b. Decreased blood pressure (BP) and CO
c. Aldosterone release results in sodium and water excretiond. Antidiuretic hormone (ADH) release increases water reabsorption
21. Progressive tissue hypoxia leading to anaerobic metabolism and
metabolic acidosis is characteristic of the progressive stage of shock.What changes in the heart contribute to this increasing tissue hypoxia?
a. Arterial constriction causes decreased perfusion.
b. Vasoconstriction decreases blood flow to pulmonary capillaries.
c. Increased capillary permeability and profound vasoconstriction lead to the
increased hydrostatic pressure.
d. Decreased perfusion occurs, leading to dysrhythmias, decreased CO, anddecreased oxygen delivery to cells.