UNIT 1 MEDICAL PATHOLOGIES OF RESPIRATORY SYSTEM
Key Unit Competence
Demonstrate an understanding of the appropriate management of different commonMedical pathologies of respiratory system.
Introductory activity 1.0
Observe the picture below and answer the following questions:
1. Indicate the normal and abnormal lung on the above figure?
2. From the abnormal lung, what are the features did you observe?
3. What are the possible diseases that can affect the abnormal lung?
1.1 ASTHMA
Learning Activity 1.1
Read careflly this below situation and answer the following questions:
Mrs. T.N. is 40-year-old woman, an athlete comes to the clinical setting with
complaints of shortness of breathing, wheezing, mucus secretions, cough, chest
tightness and chest pain, the history taking revealed that her mother died due
to asthma, oxygen saturation was 78% on room air. Chest x-ray was normal,
complete blood count (CBC): within normal limits, white blood cells (WBC) were
10000 per microliter (Normal range: 4000-11000), eosinophils was 7% (Normalrange: 0.0-6.0%), allergy-skin test: Positive for dust, trees.
Mrs. T.N. then was prescribed treatment with a low-dose corticosteroid, fluticasone
44 microgram at two puffs twice per day. However, she remained symptomatic
and continued to use her rescue inhaler 3 times per week. Therefore, she was
switched to a combination inhaled steroid and long-acting beta-agonist (LABA)
(fluticasone propionate 250 microgram and salmeterol 50 microgram, one puff
twice a day) by her primary care doctor. Her dose of inhaled corticosteroid (ICS)
and LABA was increased to fluticasone 500 microgram/salmeterol 50 microgram,
one puff twice daily. However, she continued to have symptoms and returned tothe pulmonologist for further management.
1. What are abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the
confirmation of the medical problem?
4. What was included in the management of this case?5. If not treated, what will be the consequences?
The function of the respiratory system is to supply body cells and tissues with oxygen
and eliminate carbon dioxide (CO2). Damage and disease in the respiratory system
greatly affect a person’s normal health function. It is a must to maintain the normal
and clear respiration, the maintenance of normal respiration and tissue oxygen
supply requires the well-functioning of airway flow. Some medical condition such as
asthma among others alter the proper respiratory pattern thus disturb an individualwellbeing.
Asthma is a chronic inflammatory disorder of the airway that causes recurrent
spasmodic episodes due to increased hyperirritability or responsiveness of the
bronchial tree to the various stimuli. It is a deterioration of the baseline asthma
control leading to acute wheeze, shortness of breath and dyspnoea. Asthma isusually a reversible obstructive disease of the lower airway.
Causes and risk factors of asthma
The asthma is chronic disease characterized by the various associated risk factors:
• Upper respiratory tract infections (viral, etc)
• Exposure to triggers (occupational exposure: working in industry, smoking,
air, pollution, cold, dust, etc)
• Stress
• Family history
• Obesity
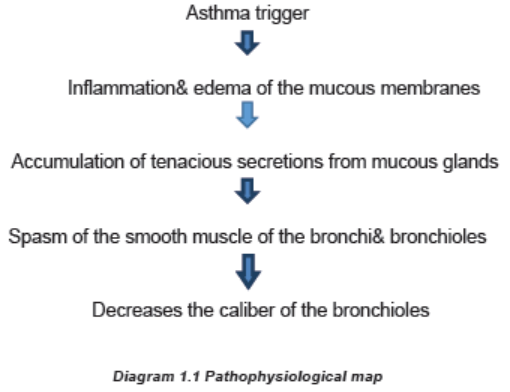
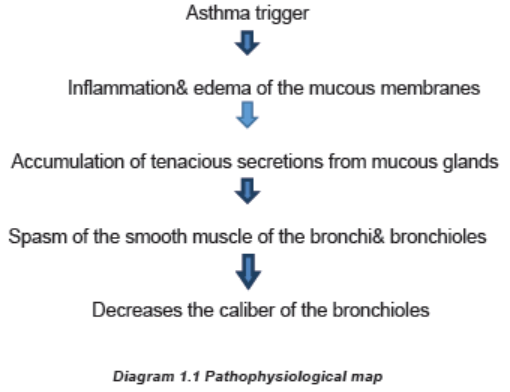
Pathophysiology overview of Asthma
The primary pathophysiologic process in asthma is persistent inflammation of the
airways which results in bronchoconstriction, airway hyper responsiveness (hyper
reactivity) and edema of the airways. The following is brief pathophysiologicalprocess of asthma development.
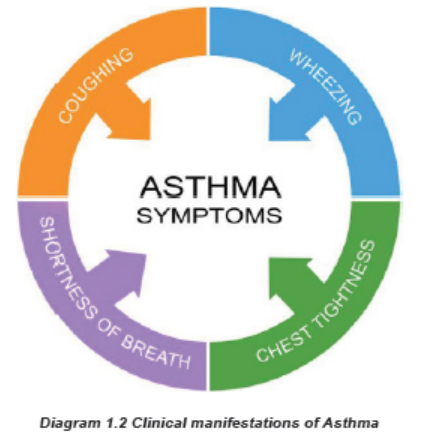
The clinical manifestations of asthma/ Signs and symptoms of asthma
The asthma symptoms are associated with shortness of breath, wheezing, mucoussecretions, cough, chest tightness, quiet chest and decreased oxygen saturation.
Investigations
The following medical investigations that are most used in diagnosis of asthma
include Laboratory (Full blood account (FBC), Immunoglobulin E); Spirometry; andImagery (chest x- ray).
Treatment plan for asthma
The goals of asthma therapy are to reduce symptoms, improve lung function, andminimize impairment of normal activity and sleep.
The goals of asthma therapy are to reduce symptoms, improve lung function, and
minimize impairment of normal activity and sleep.
Properly using asthma medication, as prescribed by the doctor, is the basis of
good asthma control, in addition to avoiding triggers and monitoring daily asthmasymptoms.
There are two main types of asthma medications:
a. Anti-inflammatories: This is the most important type of medication for most
people with asthma. Anti-inflammatory medications, such as inhaled steroids
(Beclomethazone) to reduce swelling and mucus production in the airways.
Oral steroids (Prednisolone) are taken for acute flares and help increase theefficacy of other medications and help reduce inflammation.
Possible side effects of steroids: Increased appetite, Weight gain, Changes
in mood, Muscle weakness, Blurred vision, Increased growth of body hair, Easybruising, Lower resistance to infection.
b. Bronchodilators: These medications relax the muscle bands that tighten
around the airways. This action rapidly opens the airways, letting more air inand out of the lungs and improving breathing.
The two main types of bronchodilator medicines
There are beta 2-agonists (short- and long-acting forms) and anticholinergics.
a. Short-acting beta 2-agonists (also called SABAs)
In inhaled forms, these medications include: Albuterol (Proventil® HFA, Ventolin®)
Short-acting beta 2-agonists (SABAs) are called “reliever” or “rescue” medicines
because they stop asthma symptoms very quickly by opening the airways.
They work within 15 to 20 minutes and last four to six hours. They are also the
medicines to use 15 to 20 minutes before exercise to prevent exercise-inducedasthma symptoms.
Asthma medications can be taken by inhaling the medications (using a metered
dose inhaler, dry powder inhaler, or asthma nebulizer) or by swallowing oralmedications (pills or liquids).
b. Long-acting beta-2 agonists (also called LABAs):
These medications include: Salmeterol (Serevent®), Formoterol (Foradil®),
Theophylline (Amnophylline): They contain both the long-acting beta agonistand an inhaled corticosteroid.
They are used twice a day to maintain open airways for long-term control, and they
must be used with an inhaled corticosteroid for the treatment of asthma.
Theophylline may be used to treat difficult-to-control or severe asthma and must betaken daily.
When taking theophylline, blood tests are needed to make sure you are receivingthe right amount of medicine.
Side effects include: Nausea and/or vomiting, Diarrhea and/or stomach ache,
Headache, Rapid or irregular heartbeat, Muscle cramps, Jittery or nervous feeling,hyperactivity.
c. Anticholinergic drugs
There are two anticholinergic bronchodilators currently available ipratropium
bromide (Atrovent® HFA). These are not quick-relief medications, but they can add
to the bronchodilator effect for certain asthmatics with difficult-to-control symptoms.Treatment plan of patient with asthma
• Monitor vital signs (temperature, respiratory rate, pulse, blood pressure,SP02)
• Conduct basic health assessment
• Decision making (identify disturbed patient needs)
• Ensure the client safety and quality patient care
• Collaborate with health care team (Registered Nurse (RN), Physician)
• Implement medical prescription (administration of bronchodilators and
corticosteroids, antibiotics if signs of infection, oxygen therapy if desaturating).
• Keep confidentiality of patient
• Demonstrate ethical and moral values principles while nursing care delivery
• Demonstrate effective communication skills with patient, family members and
multidisciplinary team.
Evolution and complications of asthma
Although asthma is a chronic disease with no cure, most people with mild to
moderate signs and symptoms, asthma can improve with time or go into remission
for long periods. Without treatment of asthma, the improvement can occur. Somecomplications related to asthma are:
• Severe asthma can disrupt daily life
• Sleeping disturbance
• Patient may be hospitalized
• Chronic airway inflammation/Chronic obstructive pulmonary disease
• Respiratory failure and death.
Self-assessment 1.1
Carefully read below case study and answer the following questions:
A 44-year-old woman, currently working in a bakery, presents with cough,
wheeze, shortness of breath and chest tightness with itchy red watery eyes anda stuffy, runny, itchy nose.
These symptoms become worse within 1-2 hours of starting work each day,
and worsen throughout the workweek. She especially finds red bran to worsen
her symptoms almost immediately on exposure. She notices an improvement
within 1-2 hours outside of being at her workplace. Her past medical history is
significant for seasonal allergic rhinitis in the summer months since childhood.
She is a lifelong smoker. Her family history is significant for asthma in her motherand brother.
1. According to the above signs and symptoms of patient, what is possible
medical diagnosis?
2. Describe the triggering factors contributing to the asthma development
3. What are different drugs that you can administer to this patient
4. Describe the nursing and medical management of this patient5. If this patient is not treated effectively, what could be the complications?
1.2 PNEUMONIA
Learning Activity 1.2
Read carefully the clinical case scenario below and answer the questionsthat follow.
You were going to fetch water and you meet a person who is having transpiration,
chills, coughing. While talking to him, he states that he has been in this condition
for 1 week, where he is starting to experience the productive cough like bloody
mucopurulent discharge. He has also difficulty in breathing associated withchest pain.
You accompanied him to the nearest health center. On his arrival, the vital signs
were performed and revealed respiratory rate: 36 cycles/min, Temperature: 39
Celsius degrees, pulse rate: 98 beats/min. Due to seriousness of his condition,
he has been transferred to the nearest district hospital where the medical doctor
ordered the following investigations: CBC (complete blood account) with white
blood cells of 14000/microliter (Normal 4000-11000/microliter) and chest x-ray
revealed infiltrations, blood smear was negative. His general status deteriorated
and the medical doctor decided to hospitalize the patient, ordered antibiotics
intravenous ceftriaxone 1gram BID for 7 days, oxygen therapy 3 liters/minute,
intravenous fluids therapy and required the continuous suctioning due to high
secretions causing the depletion of oxygen saturation (SPO2 of 86% on roomair, Normal value above 95-100%).
1. What are the signs and symptoms that the patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What diagnostic studies have been ordered to guide the confirmation of
that medical problem?
4. What will be included in the nursing and medical management for this
case?5. If not well treated, what will be the consequences?
The respiratory system supplies oxygen for cellular metabolic need and removes
carbon dioxide (CO2), a waste product of cellular metabolism. Respiratory disorders
and diseases are common, ranging from mild to life threatening. Disorders that
interfere with breathing or the ability to obtain sufficient oxygen greatly affect
respiratory and overall health status, the disorders that affect this system includes
inflammatory and infective disorders, the pneumonia is predominant infectivedisorder among others.
Pneumonia is an acute infection of the pulmonary parenchyma. Despite being the
cause of significant morbidity and mortality, pneumonia is often misdiagnosed,mistreated, and underestimated.
Causes of pneumonia
Pneumonia is classified according to its etiology; bacterial pneumonia is referred
to as typical pneumonia. Some of the most common causal microorganisms
include bacteria, virus, fungi. Some examples of bacterial microorganisms that may
cause pneumonia including pneumococcal pneumonia caused by streptococcus
pneumonia, staphylococcus pneumonia caused by staphylococcus aureus, gram
negative bacterial pneumonia caused by klebsiella pneumonia, anaerobic bacterial
pneumonia caused by normal oral flora. Some examples of virus that may cause
pneumonia are viral pneumonia: Influenza virus A&B adenoviruses, respiratory
syncytial virus, parainfluenza viruses. Mycoplasma: Mycoplasma pneumonia: by
mycoplasma microorganism. Fungal agents: Fungal pneumonia: by histoplasmosis,
candidiasis. Protozoa: Parasitic pneumonia, common organism is pneumocystis
carinii.
Nosocomial pneumonia is acquired within a hospital to the patient admitted to
the hospital for something else. Risk increased with an underlying illness, recent
surgery, recent intubation, and in persons already on antibiotics.
The following are some risk factors for pneumonia: advanced age,
immunocompromised, underlying lung disease, alcoholism, altered consciousness,
smoking, endotracheal intubation, malnutrition, immobilization, most cases of
pneumonia are preceded by an upper respiratory infection (often viral).
Pathophysiology overview of pneumonia
Pneumonia results from the proliferation of microbial pathogens at the alveolar
level and the host’s response to those pathogens. Many pathogens are inhaled as
contaminated droplets.
When microorganisms evade upper respiratory defense mechanisms, the alveolar
macrophage is capable of removing most infectious agents without triggering
a significant inflammatory or immune response. However, if the microbe is
virulent or present in sufficiently high numbers, it can overwhelm macrophages
and result in a full-scale activation of systemic defense mechanisms. These
mechanisms include the release of multiple chemical mediators of inflammation,
infiltration of white blood cells, and activation of the immune response.
Tight adherence of some bacteria (e.g., Pseudomonas) to the tracheal lining and biofilm
of an endotracheal tube makes clearance of these microbes from the airways
difficult and accounts, in part, for their highly virulent nature. In non-hospitalized
people, bacteria reach the lung by one of four routes:
• Inhalation of microorganisms that have been released into the air when an
infected individual coughs or sneezes
• Aspiration of bacteria from the upper airways
• Spread from contiguous infected site
• Hematogenous spread
Signs and symptoms of pneumonia
Symptoms vary for the different types of pneumonia. The onset of bacterial
pneumonia is sudden. The client experiences fever, headache, myalgia, arthralgia,
chills, chest pain, a productive cough (mucoid, purulent, bloodstained sputum),
dry cough, dyspnea, tachypnea, and hemoptysis and discomfort in the chest wall
muscles from coughing. 20% of patients may have gastrointestinal symptoms such
as nausea, vomiting, and/or diarrhea. Physical examination: Dullness to percussion,
crackles, egophony, individuals also may demonstrate signs and symptoms of
underlying systemic disease or sepsis and decreased level of consciousness.
Pneumonia can be categorized into 3 types:
• Community Acquired Pneumonia (CAP) caused by Streptococcus
pneumonia, Haemophilus influenza, Legionella pneumophila, Mycoplasma
pneumonia, Influenza virus types A, B, adenovirus, parainfluenza,
cytomegalovirus, coronavirus, Chlamydia pneumonia.
• Hospital Acquired Pneumonia (HAP) caused pseudomonas aeruginosa,
Staphylococcus aureus, Klebsiella pneumonia.
• Pneumonia in Immunocompromised Host caused by Pneumocystis carinii,
Aspergillus fumigatus, Mycobacterium tuberculosis.
Investigations
The sputum culture and sensitivity studies can help to identify the infectious
microorganism. A chest film (chest x-ray) shows areas of infiltrates and consolidation.
A complete blood count (CBC) discloses an elevated with Blood Cells (WBC) count.Blood cultures also may be performed to rule out any microorganisms in the blood.
Figure 1.4 Sample chest x-ray of the lungs, lung A revealed the normal lung while Lung B shows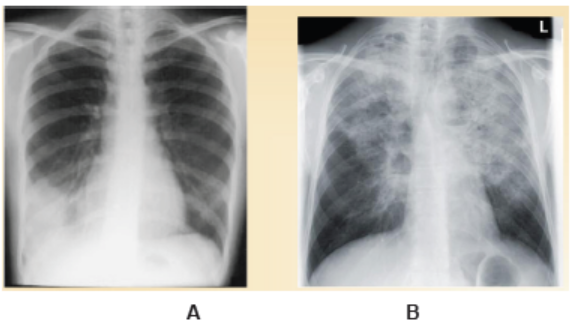
abnormal lung image.
Adequate medical diagnosis
The auscultation of the chest reveals wheezing, crackles, and decreased breath
sounds. Cyanosis of nail beds, lips, and oral mucosa may be observed duringphysical examination (inspection).
The most common investigations to be carried out during pneumonia suggests
the chest x-ray, the biological laboratory tests needed to be performed such as full
blood count (FBC) elevated (more than10000/mm3), although it may be low (below
6000/mm3) if the individual is debilitated. Sputum: Gam-stain and culture, blood
culture, Chest x-ray show infiltrates that may involve a single lobe of the lung (lobarpneumonia) or may be more diffuse (bronchopneumonia).
Treatment plan for pneumonia
Medical management of bacterial pneumonia consist of initiating antibiotic therapy,
hydration to thin secretions, supplemental oxygen to alleviate hypoxemia, bed
rest, chest physical therapy and postural drainage, bronchodilators, analgesics,
antipyretics, and cough expectorants or suppressants depending on the nature ofthe client’s cough chest physiotherapy and postural drainage.
The following are different treatment options:
• Antibiotics in case of bacterial pneumonia such as a macrolide (clarithromycin/
Erythromycin or Doxycycline.
• In case of comorbidities or antibiotics in past 3 months: High dose Amoxicilline
or Ceftriaxone plus Macrolide/ doxycicline
• In case of hospitalization: Cefotaxime or Ceftriaxone or Ampicillin plus a
macrolide/ doxycline
• Supportive therapy in case of viral pneumonia
• Adequate hydration
• Good pulmonary hygiene (deep breathing, coughing, chest physical therapy)
The nursing management of pneumonia depends on the degree of which upon the
patient is admission. The nurse auscultates lung sounds and monitors the client
for signs of respiratory difficulty. He or she checks oxygenation status with pulse
oximetry. Assessments of cough and sputum production also are necessary. The
nurse places the client in the semi-Fowler’s position to aid breathing and increase
the amount of air taken with each breath. Increased fluid intake is important to
encourage because it helps to loosen secretions and replace fluids lost through
fever and increased respiratory rate. The nurse monitors fluid intake and output,
skin turgor, vital signs, and serum electrolytes. He or she administers antipyreticsas indicated and ordered
Evolution and complications of pneumonia
When pneumonia is early and managed effectively, the outcome is observed in fewdays. However, in case of late management the following complications may occur:
• Pleural effusion
• Lung abscess
• Respiratory failure
Self-assessment 1.2
1. Describe the different causes of pneumonia
2. Explain the overview pathophysiology of pneumonia
3. Outline the signs and symptoms of pneumonia
4. List the investigations that should be ordered for confirming pneumonia
5. What is the treatment plan of patient with pneumonia?
6. What are the complications of pneumonia?
1.3 BRONCHIOLITIS
Learning Activity 1.3
Read carefully this below situation and answer the following questions:
A 5-month-old boy presents with a 3-day history of cough, rhinorrhea, congestion,
and fevers. Today his mother noticed he was breathing faster and taking in less
formula than normal. His 4-year-old sister has a cold and he attends a local
day care. On physical exam, the boy’s temperature is 102.5°F (39°C), heart
rate is 140beats per minute, respiratory rate is 60 breaths per minute, and
blood pressure is 90/50mmHg. His oxygen saturation is 95%. He appears alert
and smiling but is tachypneic and coughing. He has subcostal and intercostal
retractions. On auscultation of his lungs, wheezing is heard on both inspirationand expiration. The complete blood count was performed and revealed normal.
1. What are the abnormal clinical manifestations can you identify from above
scenario?
2. What do you think is the medical condition the boy is presenting?
3. List the causes and risk factors contributing to the development of the
identified medical condition.
4. Outline the treatment modalities of the above medical condition.
5. Describe the preventative measures that will be advised to the family to
avoid cross-contamination.
Bronchiolitis is a common lower respiratory tract infection that affects babies and
young children. The early symptoms are similar to those of a common cold, such
as runny nose or cough.
Causes of bronchiolitis
Bronchiolitis is usually caused by a viral infection. Many different viruses can be the
culprit, including the flu, but the most common in children is what’s called respiratorysyncytial virus.
Outbreaks of this virus happen every winter. They may only get mild symptoms, butin severe cases it can cause bronchiolitis or pneumonia
Pathophysiology overview
The pathophysiology of bronchiolitis begins with an acute infection of the epithelial
cells lining the small airways within the lungs. Such infection results in edema,increased mucus production, and eventual necrosis and regeneration of these cells.
The inflammation, edema, and debris result in obstruction of bronchioles, leading
to hyperinflation, increased airway resistance, atelectasis, and ventilation-perfusion
mismatching. Bronchoconstriction has not been described. Infants are affected
most often because of their small airways, high closing volumes, and insufficient
collateral ventilation. Recovery begins with regeneration of bronchiolar epithelium
after 3-4 days; however, cilia do not appear for as long as 2 weeks. Mucus plugsare instead predominantly removed by macrophages.
The pathogenesis of bronchiolitis involves a combination of airway edema,
increased mucus production, and necrosis of airway epithelial cells due to direct
cytotoxic injury. Respiratory syncytial virus transmission occurs from person to
person either by direct inoculation of nasal mucosa with contaminated secretions
or by inhalation of large infectious droplets. Virus replicates in the nasal epithelium,
and an exaggerated immune response occurs, with an influx of natural killer cells,
lymphocytes, and granulocytes into the epithelium. After an incubation period of 4
to 6 days from transmission, upper respiratory tract symptoms appear, includingnasal congestion and rhinorrhea.
Signs and symptoms
The most common signs and symptoms of bronchiolitis are: runny nose, fever,
stuffy nose, loss of appetite and cough are the first signs of the infection. Symptoms
may worsen after a few days and may include wheezing, shortness of breath, andworsening of the cough. The child might show more severe signs, including:
• Making grunting noises.
• Having trouble sucking and swallowing, this makes feeding difficult on top of
having a poor appetite.
• Trying so hard to breathe that the chest retracts (the skin is drawn down
tightly against the rib cage and looks like it is going inward).
• Turning blue or gray in the lips, fingertips or toes.• Being sluggish.
Investigations
The diagnosis of bronchiolitis is mainly based on clinical manifestations. Pulseoximetry is useful if hypoxia is suspected. It is not unusual for these infants to
experience mucous plugs leading to hypoxia. If supplemental oxygen is required,
the goal should be to maintain saturation levels between 90 and 100%.
Beyond the physical exam, the following diagnostic tests might be done:
• Laboratory: Full blood count (FBC), white blood cells are increased (Normal
range: 4000-11000/mm3), chain reactive protein might be positive and
increased (Normal range: 6.8-820 mcg/dL), neutrophils are increased (Normal
range: 0-8%), increased erythrocyte sedimentation rate (Normal value: <30
mm/hr).
• Chest Radiograph: A chest radiograph is indicated if pneumonia, a chest
mass, a foreign body, or heart failure are suspected. In bronchiolitis, the
radiograph may show hyperinflation or scattered areas of atelectasis. This is
can be misinterpreted as bacterial pneumonia.
• Nasal Specimen: A nasal aspirate for antigen detection of respiratory
syncytial can be performed. Influenza A and B and adenovirus can also be
detected by this method.
Adequate medical diagnosis of bronchiolitis
The diagnosis of bronchiolitis is made primarily based on history and physical
examination findings. A mucus sample test (where a sample of mucus from your
child’s nose will be tested to identify the virus causing their bronchiolitis) urine or
blood tests. A pulse oximeter test (where a small electronic device is clipped to the
child’s finger or toe to measure the oxygen in their blood) must be performed.Treatment plan of bronchiolitis
The physician has the role to diagnose and prescribe the medication according
the signs and symptoms, also the results of investigation done; the physician
orders the following medications according the medical decision and guideline:
Bronchodilators. Bronchodilators are frequently tried in infants presenting with
wheezing due to bronchiolitis because of its similarity to asthma, Anticholinergicagents, Corticosteroids, Ribavirin, Antibiotics, Surfactant, Heliox.
Treatment at home:
• Keep the child upright. Keeping the child upright may make it easier for them
to breathe, which may help when they are trying to feed.
• Make sure the child drinks plenty of fluids.
• Do not smoke at home.
• Relieving a fever.
• Saline nasal drops.
Symptomatic care: There is no cure for bronchiolitis, so treatment is aimed atthe symptoms (eg, difficulty breathing, fever). Treatment at home usually includes
making sure the child drinks enough and saline nose drops (with bulb suctioningfor infants).
The nurse carries out the following activities at hospital: Provide oxygen if saturations
are low, Assist with oral hydration, Listen to the lungs, Monitor oxygenation, Assess
vitals, Intake and output, IV (intravenous) fluids if your child can’t drink well, Extra
oxygen and a breathing machine (ventilator) to help with breathing, Frequent
suctioning of the child’s nose and mouth if respiratory tract secretions, Breathingtreatments, as ordered by your child’s healthcare provider.
Evolution and complications of bronchiolitis
In most cases, the disease is mild and self-limited. With bronchiolitis, as any other
diseases, various complications are possible. If the child develops complications from
bronchiolitis, it’s likely that they’ll need hospital treatment. Potential complicationsof bronchiolitis include:
• Cyanosis (a blue tinge to the skin caused by a lack of oxygen)
• Dehydration (when the normal water content of the body is reduced)
• Fatigue (extreme tiredness and a lack of energy)• Severe respiratory failure (an inability to breathe unaided)
Self-assessment 1.3
Carefully read the following case scenario and answer the followingquestions:
J.N is a 5-month-old previously healthy boy who presents today with a 3-day
history of cough, runny nose and fever. His mother brought him into the
emergency department because since this morning he has been sleepy and
not interested in feeding. He has no significant gestational or birth history, and
is meeting his developmental milestones, but of note, he is bottle-fed. He is upto-
date on his immunizations. The only other significant detail is that his older
sister was home sick from daycare last week. On exam, his heart rate is 120
beats/minute, his respiration rate is 60 breaths /minute, and his temperature
is 39°Celsius and oxygen saturation (88 %). His weight is 7kg. He has signs
of respiratory distress and on auscultation; bilateral wheeze and crackles, andnasal flaring was observed.
1. After reading the above situation, identify the signs and symptoms that
present this patient.
2. Basing on clinical manifestations of J.N, what could be the medical
diagnosis?
3. Briefly, describe the pathogenesis of the medical diagnosis?
4. What are the most common causes of J.N medical condition?
5. What are investigations might be ordered to J.N?
6. What is the medical and nursing management of J.N medical condition?
7. What are the most complications that might occur to J.N if it’s poorlymanaged?
1.4 END UNIT 1 ASSESSMENT
End unit 1 assessment
Section A: Multiple Choice Questions
Circle the letter that corresponds to the best answer for each question
1. Pneumonia is infection of the lungs caused by :
a. Bacteria
b. Virus
c. Fungid. All the above
2. Nosocomial pneumonia is pneumonia that is acquired from:
a. The community
b. Hospital environment
c. Within the place of residenced. From the neighbors at home
3. Pneumonia that develops following passage of food particles, drink etc.
into the lungs is called:
a. Community acquired pneumonia
b. Aspiration pneumonia
c. Atypical pneumoniad. None of the above
4. Which of these causes atypical pneumonia?
a. Pneumococcus
b. Mycoplasma
c. Influenza virusd. Respiratory Syncytial Virus
5. …………………is a common lung infection in young individuals
a. Bronchiolitis
b. Pneumonia
c. Bronchitisd. Asthma
6. ……………is inflammation of the bronchioles usually caused by an acute
viral
a. Asthma
b. Bronchitis
c. Pneumoniad. Bronchiolitis
7. Which of the following is correct regarding bronchiolitis?
a. It is more common in the summer months.
b. Parainfluenza virus is the commonest cause.
c. The disease is most common in children aged 2-4 months.d. Wheezing is a highly specific symptom for bronchiolitis
8. The following are known to cause bronchiolitis in infants EXCEPT:
a. Para influenza
b. Chlamydia
c. Mycoplasmad. Streptococcus pneumonia
9. Symptoms included in a written asthma action plan that would prompt
the use of reliever therapies include all of the following EXCEPT
a. Chest tightness
b. Hemoptysis
c. Wheezingd. Persistent Cough
10. What is a common symptom of asthma?
a. Wheezing
b. Full breaths
c. Snoringd. Crackles
11. What is the cure for asthma?
a. There is no cure of asthma
b. It depends on the patient
c. It depends the drugs administeredd. It depends the triggers
12. In providing patient education, which of the following has been shown to
result in emergency care utilization?
a. Teaching about the pathophysiology of asthma
b. Teaching self-management skills
c. Teaching inhaler techniqued. Teaching about the pharmacology of the drugs
13. Asthma is characteristically defined by the following triad:
a. Airway inflammation
b. Airway hyper-responsiveness
c. Reversible airflow obstructiond. Reversible airflow constriction
14. Normal pulse oximeter readings usually range from:
a. 95 to 100 percent
b. 90 to 95 percent
c. 85 to 90 percentd. 80 to 85 percent
a. Which of the following statement about Salmeterol is not true?
a. It acts by relaxing muscles in the airways to improve breathing
b. It is a short-acting selective β2 agonist
c. Salmeterol inhalation is used to prevent asthma attacks
d. Salmeterol inhalation is used to treat COPD including emphysema andchronic bronchitis
15. ……………is a bronchodilator that relaxes muscles in the airways and
increases air flow to the lungs.
a. Ventolin (albuterol)
b. Beclomethasone dipropionate (Qvar)
c. Budesonide (Pulmicort)d. Budesonide/Formoterol (Symbicort)
16. These are Anti-inflammatory medications reduce swelling and mucus
production in the airways EXCEPT
a. Beclomethasone dipropionate (Qvar)
b. Budesonide (Pulmicort)
c. Budesonide/Formoterol (Symbicortd. Theophylline
17. Side effects of beta 2-agonists include EXCEPT:
a. Increased heart rate.
b. Upset stomach (rare).
c. Trouble sleeping (rare).d. Increased appetite.
18. Bronchodilators are the most effective treatment for asthma (True or Fal
se)
19. Cough can be the only presenting complaint in patients with asthma (
True or False)
20. Asthma is a chronic respiratory disease (True or False)
21. People with reduced immunity tend to suffer from a more severe form of
pneumonia (True or False)
22. The cough in bacterial pneumonia is a dry type of cough (True or False)
23. Pneumonia can be prevented by vaccination (True or False)
Section B: Short Answer Questions
1. Define asthma and its clinical features.
2. How to diagnose pneumonia?
3. Explain the pathophysiology of asthma.
4. What is treatment plan of patient with bronchiolitis?5. What is treatment plan of pneumonia?