CLINICAL SITE EVALUATION FORM
Associate Nurse program
Clinical Site’s Name: ………………………………………………………………
Service / Ward: ………………………………… senior ……………………..…
Program… trimester
Period: From …………………./…../………to ……../…../…………
Grading scale: 5= excellent 4= very satisfied 3=satisfied 2= dissatisfied
1= very dissatisfied
Indicate your rating of the clinical site by placing a tick (√) to the right number as
indicated below: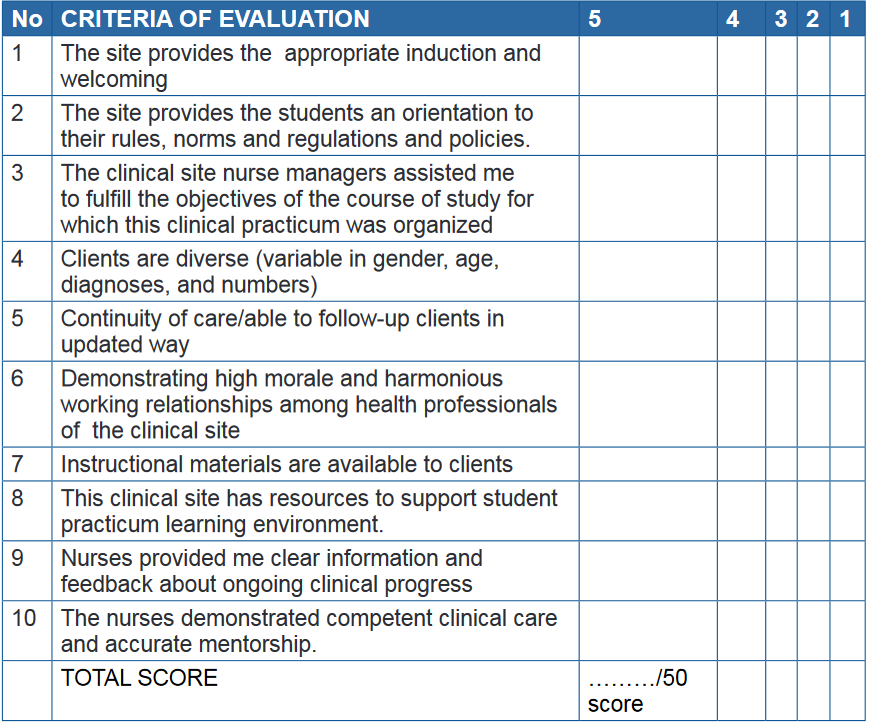
GENERAL COMMENTS:
THE BEST FEATURES OF THE SERVICE:
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………
I WOULD LIKE TO SEE THE FOLLOWING CHANGES:
………………………………………………………………………………………………
………………………………………………………………………………………………
………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………
Associate Nurse program
Student’s Name: …………………………………………………………………...…
Clinical Site’s Name: …………………………………………………………………
Service / Ward: …………………………………Senior ……….……………..……...
Trimester ………………………………………………
Clinical placement Period: From ...………………./…../20…to ……../…../20………