UNIT8 LEARNERS WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD) AND LEARNERS AUTISM
Key Unit Competence: Explain the characteristics of learners with autism
and ADHD and use appropriate approaches to
teach them
INTRODUCTORY ACTIVITY
Kalisa is a 13-year boy and was born in rural village. In his daily activities
he had inattention to accomplish tasks and was not able to follow some
instructions because of his hyperactivity. His parents had tried to take him
to the nearest school in order to help him but his condition did not improve.
He interrupted his classmates during class activities (taking notes, talking,
throwing things, etc.). During break time he would run, jump and drive
imaginary vehicles. Even though he was overactive he was also interested in
playing music with piano or guitar and singing. His teacher had discovered
that Kalisa may be good at music and then oriented him to another teacher
who could use appropriate techniques to teach music and musical instrument
playing to Kalisa. The teacher advised his parents to take him to a specialist,
this they gladly did and Kalisa was diagnosed with ADHD (Attention Deficit
Hyperactive disorder). In three years later Kalisa was able to play the piano
and sing some songs. His parents became happy because of their child’sattainment and his parents want to support him to make album of his songs.
Question:
1. Describe Kalisa’s behaviours in her class and outside?
8.1. Learners with Attention Deficit Hyperactivity Disorder
(ADHD)
8.1.1. Definition, causes and characteristicsof Attention Deficit
Hyperactivity Disorder (ADHD)
ACTIVITY 8.1.1
Use books or other sources of information to answer the following
questions:
2. What do you understand by Attention Deficit Hyperactivity
Disorder (ADHD)?
3. According to you, what do you think as risk factors of ADHD?
4. What do you understand by the following terms?
• Inattention
• Hyperactivity
• impulsivity
Definition of Attention Deficit Hyperactivity Disorder
Attention Deficit Hyperactivity Disorder is defined as persistent pattern of
inattention and/or hyperactive impulsivity that is more frequent and severe
than is typically observed in individual at a comparable level of development.
In order to make clear the meaning of ADHD, there are guidelines that help
everyone to describe it but even though those criteria may seem to happen to
every person, also there is a persistent or a chronic condition for those who
have Attention Deficit Hyperactive Disorder which makes some differences. It
is believed to affect around 3 to 5 percent of children who are or before 7 years
old. It is a chronic condition that affect a million of children in the world and
often continues in adulthood. It a combination of persistent problem such as
sustaining attention, hyperactivity and impulse behaviours.
Causes of Attention Deficit Hyperactivity Disorder (ADHD)
The exact cause of ADHD is not well known but researchers explore possible
possibilities including neurological foundations, hereditary and environmental
conditions.
Neurological foundation: using the neuroimaging technology,
researchers found that some parts of brain appear to exhibit
abnormalities in persons with ADHD. The front lobes are one part
of the brain in charge of executive functions such as self-regulation,
working memory, inner speech. The basal ganglia are responsible in
controlling and coordination of motor behaviour. Attention Deficit
Hyperactive Disorder results from dysfunction of neurotransmitter ofdopamine in the region of the brain that control activity and attention.
Hereditary factors: There is strong evidence of the role of heredity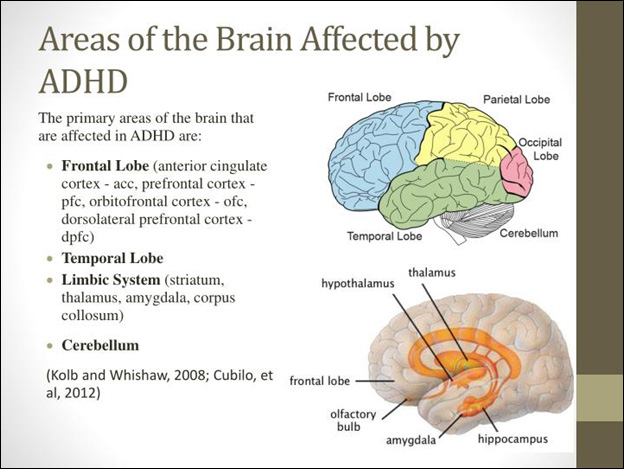
in contributing to ADHD. Family studies revealed that a child who
has ADHD is more likely to have a parent who exhibit ADHD (Barkley,
2006). Also, the investigating of monozygotic (identical) and dizygotic
(fraternal) twins have consistently found a high concordance of ADHD
in identical twins that in fraternal twins.
Environment factors: Virous pre-, peri-, postnatal traumas are
also implicated as contributing to Attention Deficit Hyperactive
Disorder (ADHD). Some example of environmental factors includes
maternal smoking and alcohol abuse, lead poisoning, low birth
weight and prematurity. There are other many environmental
factors that researchers found to be typical examples but with
poor scientific support such as too much/little sugar, badparenting, too much television, food addictive/colouring, yeast.
Characteristics of learners with Attention Deficit Hyperactivity
Disorder (ADHD)
Attention Deficit Hyperactivity Disorder is the chronic nature of characteristic
and their duration that often lead to impaired functioning in activities of daily
living. ADHD has three subtypes:
ADHD with inattentive type, inattention indicates that child might have
attention span, or difficulties of sustaining his or her attention for more
than a brief period of time.
ADHD with predominantly hyperactive-impulsive type, Hyperactivity
is a condition in which a child is easily excitable or over-active.
Impulsivity is the inability to think first before resorting to an action.
ADHD with combined inattentive and hyperactive-impulse types.
ADHD has criteria for each of those subtypes. Six of these following symptoms
may lead to confirm an ADHD if these symptoms last for 6 months to a degree
that is maladaptive and inconsistent with developmental level.
Characteristics of learners ADHD by each subtype
Characteristics of Inattention
• Often fail to give close attention to details or makes careless mistake in
schoolwork, work or other activities.
• Have difficulties of sustaining attention in tasks or play activities.
• Often does not seem to listen when spoken to directly.
• Does not follow through on instructions and fails to finish school work,
chores, duties in the workplace (not due to oppositional behaviour or
failure to understand instructions)
• Often avoid, dislike, or is reluctant to engage in tasks that require
sustained mental efforts (school work and home work)
• Often loose things necessary for tasks or activities (e. g: toys, school
assignments, pencils, books, or tools)
• Is often easily distracted by extraneous stimuli.
• Is often forgetful in daily living
Characteristics of learners Hyperactivities
• Often fidgets with hands or feet or squirms in seat
• Often leave seats in classroom or in other situations in which remains
seated is expected
• Often runs about, claims excessively in situation in which it is
inappropriate
• Often has difficult in playing or engaging in leisure activities quietly
• Talk excessively
Characteristics of learners Impulsivity
• Often blurts out answers before questions have been completed
• Often has difficult of awaiting turn
• Often interrupts or intrudes on others (e. g: butts into conversation or
games).
The symptoms must be present in before 7 age. Clear evidence must also
be present in the two or more setting (social, academic and occupationalfunctioning...).
SELF-ASSESSMENT 8.1.1
1. Discuss the following term: Inattention, hyperactivity and
impulsivity.
2. What are subtypes of ADHD learners?
3. Discuss the characteristics of children with ADHD.
4. Discuss the meaning of ADHD
5. What is the range of children from which are affected by ADHD?
8.1.2. Teaching and learning approaches for learners with ADHD
ACTIVITY 8.1.2
1. According to you, how can you teach learners with ADHD?
This is an important issue for many classroom teachers and parents who have
children with ADHD. Most people with ADHD experience significant difficulties
in school while attention and impulse control are prerequisites for success.
Most of children with ADHD respond to a structured and predictable learning
environment where rules and expectations are clearly stated and understood,
consequences are predetermined, reinforcement is delivered immediately.
Environment modifications alone are not the key to success. Educational
researches believe multimodal interventions, or concurrent treatment, are
generally more effective for individuals with ADHD than any one strategy.
Here are four main approaches that help to teach leaners with Attention Deficit
Hyperactivity Disorders
Instructional adaptations: Instructional adaptation coupled with
modification of the learning environment are powerful tools that can
help people to sustain attention while cultivating a climate that fosters
learning and encourage the child to control his/her behaviour. Teachers
should know individual differences and learning styles of children who
exhibit impairment that limit a major life activity like learning. Lerner
and Lowenthal (1993) provided some suggestions for teachers:
• Place the youngster in the least distracting location in the class (in
front of the class, away from doors, windows, air conditions, etc.
• Surround the students with good role models,
• Maintain a low pupil- teacher ratio whenever through the use of aids
and volunteers.
• Avoid unnecessary changes in schedules and monitor transitions
because the child with DAHD often has difficult copping with changes.
• Maintain eye contact with the student when giving verbal instructions
• Combine verbal and tactile cues with verbal instructions.
• Make a list that help the student organize tasks.
• Adapt break assignment into small chunks
• Ensure that the student has recorded homework assignment
• If the child has difficult staying in one place at school, alternate sitting
with standing and activities that requires moving around during the
day.
• Provide activities that requires active participation such as talking
through problems or acting out the steps.
• Use learning aids such as computers, calculators, tape records, and
programmed learning materials
• Provide student opportunities to demonstrate strengths at school.
Behavioural interventions:This approach helps to determine the
purpose of or function that a particular behaviour serves and how to
discourage or motivate. Once a good assessment is done the goal is
to construct interventions that modify the antecedent or triggering
behaviours and/or the consequences that are reinforcing and
maintaining the undesirable performance.
Home - school communication:It is essential for all pupils but
especially for those who have ADHD, it is an important ingredient
in promoting their success at school, the partnership must be
ongoing, reciprocal, mutually respect, and student centred. Parents
are encouraged to participate actively in their children’s plans and
collaborate with the multidisciplinary team. Teacher-parents may use
strategies work best for them.
Medication, and counselling represent some of available
intervention options for individual with ADHD. Some medication
like psychostimulants may play an important role in the treatment of
behaviours of ADHD. It is good to use this medication in conjunction
with educational and behavioural interventions. Teacher should
not recommend to parent that their son or daughter needs to be on
medication but only child’s health care professional can make such
a determination. Medication represent one part of the total package
and should not be seen as the panacea for ADHD. Instructional
and environmental accommodation should always be the first
intervention tactic used to assist pupils with Attention DeficitHyperactive Disorder,
SELF-ASSESSMENT 8.1.2
1. Describe one method that helps schools and parents to teach
learners with ADHD.
2. Discuss the instruction adaptational methods of teaching learners
with ADHD that should be used by teachers.
8.2. Learners with autism
8.2.1. Definition, causes and characteristics of Autism
ACTIVITY 8.2.1
Use books or other sources of information to answer the following
questions:
1. How do you understand Autism?
2. According to your mindset, what do you think are causes of
autism?
3. What will push you say that achild has autism?
Definition of Autism
Autism is a complex neurobiological disorder of development that lasts through
a person’s lifetime. Autism onset is between 0-5 years, and is three times more
likely to affect males than females. Autism Spectrum Disorder (ASD) affect
three area of deficiencies (also called triad of impairment) of development such
as communication development, social relatedness, and behaviours.
Brief introduction about Autism
People with autism have problems with social interactions and communication,
so they may have trouble of having conversation with others, they may not look
at in the eye. They may sometimes have behaviours that they have to or that
they do ever over and ever, like not being able to listen until their pencils are
lined up or saying the same sentences again and again. They may frap their
arms to tell you they are happy or they may hurt themselves to tell you they are
not.
The term Autism was first used by the Leo Kanner in 1943. Kanner described
eleven children with inability to relate themselves in ordinary way to people
and situations. Kanner used the term Autistic which means to “escape from
reality”, to describe the condition. Prior to Kanner’s work, autists people were
given many labels including: childhood schizophrenia, feebleminded, ideots,
imbeciles, mentally retarded.
Kanner believed that those children come to the world with innate to form the
usual, biological effective contact with people, just as other children come into
the world with the innate physical or intellectual handicap. He described those
children as having an excellent rote memory, delays in the acquisition of speech
and language (including pronouns reveal, echolalia, and extreme literalness
and obsessive desire for the maintenance of sameness. People use to confuse
Schizophrenia and Autism. Schizophrenia is a mental illness characterized by
strange speech and abnormal behaviour and a decreased ability to understand
reality.
Kanner (1943) differentiated both disorders in three areas:
• An extreme aloneness from the beginning of the life
• An attachment to objects
• Powerful desire for aloneness and sameness
For Kanner, Autism is inability to relate to themselves, it starts as extreme
autistic aloneness, whenever possible, disregards, ignores, shuts out at anything
that comes to the child from outside.
According to Diagnostic and Manual of Mental Disorders of American Psychiatric
Association (2000), there are five specific autism diagnoses under pervasive
developmental disorders (PDD) such as:
Autistic disorder: it is a disorder which is characterized by deficit
in reciprocal social communication, deficits in communication and
language, restricted and repetitive behaviours and interests.
Asperger disorders: it is known as milder form of autism. The major
characteristic of this disorders is a lack of interest in social relationships
or difficulties in forming a relationship with others. According to
Ozonoff and Rogers, 2003, The language is not impaired and there is no
impairment in cognitive functions
Rett disorder: it is a condition found only in girls. Children who receive
diagnosis usually show typical growth up to 5 or 6 months of age. They
begin to use their interest in other over time.
Childhood disintegrative disorders: it continues a period of typical
growth in the child followed by loss of developmental skills, which
eventually ends in severe cognitive deficits and others abilities.
Pervasive not otherwise specified
Pervasive Developmental Disorder (PDD) refers to a group of
disorders which are characterized by delays in the development of
socialization and communication skills.
Causes of Autism
We know that there is no one cause of autism. Researchers believe that genetic
and non-biological factors may influence the risk of having autism.
Genetic factors:
Researchers believe that autism tends to run in families. Changes in certain
genes increase the risk that a child will develop autism. If a parent carries one
or more of these gene changes, they may get passed to a child (even if the parent
does not have autism). Other times, these genetic changes arise spontaneously
in an early embryo or the sperm and/or egg that combine to create the embryo.
Current knowledge regarding ASD mostly comes from family and twins’ studies.
Environmental risk factors
Researchers believe that certain environmental influences may further
increase or reduce autism risk in people who are genetically predisposed to
the disorder. Importantly, the increase or decrease in risk appears to be small
for any one of these risk factors. Exposure to environmental toxins, such as
maternal exposure to memory during pregnancy, excessive use of antibiotics in
children, household and environmental pesticides.
The characteristics of Autist
Autism is looked through three criteria including impairment in communication,
impairment in the use of non-verbal behaviours, restricted and stereotyped
patterns of behaviours, interests and activities. The abnormal functioning in at
least one of social interaction and language, with onset prior to age 3 can define
autism but not limited to that.
a. Qualitative impairment in social interaction, as manifested by at least two
of the following:
• Marked impairment in the use of multiple nonverbal behaviours such
as eye to eye gaze, facial expression, body postures and gestures to
regulate social interactions.
• Failure to develop peer relationships appropriate to developmental
level.
• Lack of spontaneous seeking to share enjoyment, interests, or
achievement with other people (lack of showing, bringing, or pointing
out objects of interest.
• Lack of social or emotional reciprocity.
b. Qualitative impairment in communication as manifested by at least one
of the following:
• Delay or total lack of the development of spoken language (not
accompanied by not to attempt to compensate through alternative
modes of communication such as gestures or mime)
• Individual with adequate speech, married impairment in the ability to
initiate or sustain a conversation with others
• Stereotyped and repetitive use of language or idiosyncratic language.
• Lack of varied, spontaneous make-believed play or social imitative play
appropriate to developmental level.
c. Restrictive repetitive and stereotyped patterns of interests, and activities
as manifested by at least one of the following:
• Encompassing preoccupation with one or more stereotyped and
restricted patterns of interest that is abnormal either in intensity of
focus.
• Apparently inflexible adherence to specific, non-functional routines or
rituals.
• Stereotyped and repetitive motor mannerism hands of fingers flappingor twisting, or complex whole-body movement).
SELF-ASSESSMENT 8.2.1
1. Define the word autism
2. Discuss three angles through which autism is seen.
3. Describe characteristics of learners with autism.
4. Provides some labels given to autistic people according to
Kanner’s work
5. For DSM IV there are four types of autism, discuss.
8.2.2. Teaching strategies for learners with Autism
ACTIVITY 8.2.2
1. From your own thought, what are some of the services that
should be given to learners with autism to help them in everyday
lives?
Early educational intervention makes a positive difference in the life of
an individual with autism. Early intervention services typically include a
structured educational and behavioural modification strategies with related
and specialized services. Those related and specialized services may include:
• Assistive technology and services
• School nursing services
• Parent counselling and training
• Nutrition services
• Artistic and cultural programs-art, music, and dance therapy
• Occupational therapy
• Speech and language therapy
Early interventions begin with the development of an individualized family
service plan (is a plan for special services for young children with developmental
delays, IFSP), which typically addresses needs in the areas of social skills,
functional skills (dressing, toilet training, self-feeding), communication,
and behaviour modification. No one program is applicable to all children
with Autism, the strength and needs of each child must be considered in thedevelopment of specific educational plan.
Techniques of a structured educational approach
Some of techniques of a structured educational approach include but not
limited to:
• Use Task Analysis: very specific, tasks in sequential order.
• Always keep your language simple and concrete.
• Teach specific social rules/skills, such as turn-taking and social
distance.
• Give fewer choices and avoid using sarcasm
• Avoid using idioms. “Put your thinking caps on”, “Open your ears”
and “Zipper your lips” will leave a learner completely mystified and
wondering how to do that.
• Give very clear choices and try not to leave choices open ended.
• Repeat instructions and checking understanding. Using short sentences
to ensure clarity of instructions.
• Providing a very clear structure and a set daily routine including time
for play.
• Providing warning of any impending change of routine, or switch ofactivity. Etc…
According to Bayat (2012) adaptations and modification of the environment and curriculum
for autist learners should be based on their sensory and behavioural needs.
Early childhood special education and inclusive classrooms will benefit
from arranging the environment based on the following guidelines:
Use of visuals in the classroom: these are the objects and pictures
that can be used in order to enhance communication with learner
with autism. Pictures are symbols that represent specific objects,
actions, concepts. Visual has become important element of a
successful interventions for children with autism in Early Childhood
Special Education and inclusive classrooms. Picture exchange
communication system is an effective method of working with
autism that enables them to communicate with peers and adults.
Specific physical arrangement of the classroom and home: The
environment should [provide messages in the regard where things
are and what to be done. Visual should be used to labels, desks,
drawers, and materials.
Cozy corner and sensory-oriented activities to support selfregulation:
Children with autism should have a cozy corner, contained
refuge that has a calming effect for children. Pillows beanbags, and
blankets should be available for children to calm down when they
are having tantrum as a result of a sensory overload.
Providing daily and weekly schedules: Children with Autism benefit
from predictable routine. In daily schedule the adults give clear
messages to children about plan of a day and what exactly willhappen through the day.
SELF-ASSESSMENT 8.2.2
1. What are some specialized services available for children with
autism?
2. Why should visuals be used in a classroom for learners with
autism?
SKILLS LAB
1. Visit a special school and identify two learners, one is suspected
to have Attention Deficit Hyperactivity Disorder and another one
suspected to have autism. Spend four hours with both children.
On three pages, describe the characteristics of each child and
suggest strategies you could use to teach both leaners and suggest
some recommendations.
END OF UNIT ASSESSMENT
1. Mention four main approaches teachers can use to teach learners
with ADHD.
2. Discuss ADHD subtypes and its characteristics
3. Discuss the interventional approaches for a learner with ADHD
4. What are the characteristics of an Autist? child ?
5. What is the role of early intervention for leaners with autism?
6. Discuss three areas which characterize learners with autism?
7. Discuss the techniques of structured educational approaches
which are used to teach learners with Autism?8. What are the guidelines for supporting the learners with autism?