UNIT 1 MEDICATIONS FOR PAIN, FEVER, SEIZURES AND INFLAMATION
Key Unit competence:
Provide appropriate medications for pain, fever, inflammation, and seizures.
Introductory activity 1.0
Observe the images above and respond to the following questions:
1. What do you observe from the images above?2. What do you think people on the images above are doing or experiencing?
1.1. Overview on pathophysiology of fever
Learning Activity 1.1
1. Ill patients can express different symptoms in their illness status which arefound during nursing assessement and managed with different medications
2. Patient on image A started complaining of health condition, and the
bassessment’s data have shown a high fever of 38.5oc. different medications
were selected for the management of the case (Image C & B). Using librarytextbooks, describe the physiology of fever.
CONTENT SUMMARY
Thermoregulation is interceded by the hypothalamus. Peripheral thermoreceptors
located in different body parts as skin, abdominal organs, as well as central
thermoreceptors found in the spinal cord and other central locations offer the
hypothalamus with information about skin and core temperatures. If these
temperatures are abnormally high, the hypothalamus responds by triggering or
heat loss mechanisms. While, when the temperatures are abnormally low thehypothalamus responds by triggering heat production, heat conservation.
Body temperature is determined by the balance between heat production by tissues,
particularly the liver and muscles, and heat loss from the periphery. Normally, the
hypothalamic thermoregulatory center maintains the internal temperature between
37° and 38° C. Fever results when something raises the hypothalamic set point,
triggering vasoconstriction and shunting of blood from the periphery to decrease
heat loss; sometimes shivering, which increases heat production, is induced. These
processes continue until the temperature of the blood bathing the hypothalamus
reaches the new set point. Resetting the hypothalamic set point downward for
example, when antipyretic drugs are given, initiates heat loss through sweating
and vasodilation. The capacity to generate a fever is reduced in certain patients likealcoholics, the very old, the very young.
Pyrogens are substances that cause fever. Exogenous pyrogens are usually
microbes or their products. The best studied are the lipopolysaccharides of gramnegative
bacteria, commonly called endotoxins and Staphylococcus aureus toxin,
which cause toxic shock syndrome. Fever is the result of exogenous pyrogens
that induce release of endogenous pyrogens, such as interleukin-1 (IL-1), tumor
necrosis factor-alpha (TNF-alpha), and IL-6 and other cytokines, which then trigger
cytokine receptors, or of exogenous pyrogens that directly trigger Toll-like receptors.Prostaglandin E2 synthesis appears to play a critical role.
Fever is a natural defense mechanism for neutralizing foreigner organisms. High
body temperature or fever destroys and kills many species of bacteria; but when it
remain high it destroy even some normal cells of human body. Medications used totreat fever are known as antipyretics
Fever is diagnosed by measuring body temperature using thermomether , The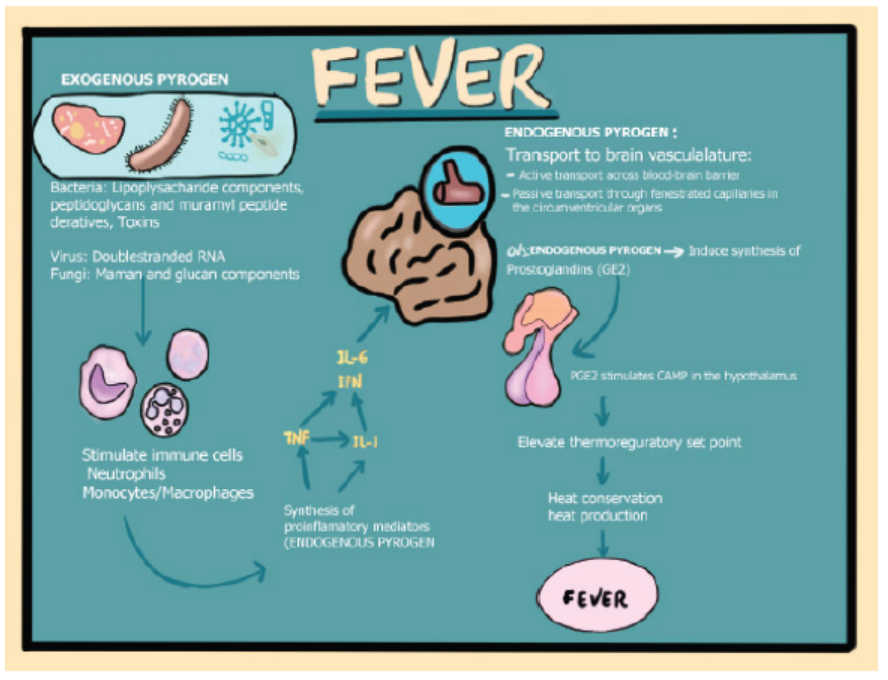
use of thermometer to measure body temperature is the most accurate way of
diagnosing fever. Sites for fever mesearument include oral,axillary,tympanic,analdepending on available materials, age, status and preferance of the patient.
A nurse should consider as fever the temperture above 37.50c, if the thermometer
is not available touching the skin is an other alternative even though,it is less
acurate and can expose to any other health related problems such as infection
desease transmission. This is especially the case if you’re self-diagnosing. When
using touch to diagnose a fever in someone else, touch your own skin first, then
touch the other person to compare the two temperatures. If the other person is a
lot hotter than you, they may have a fever. You can also try pinching the skin on the
back of your hand to check for signs of dehydration. If the skin doesn’t snap backquickly, you might be dehydrated. Dehydration may be a sign of a fever.
Self assessment 1.1
Complete the following sentences:
1. When the body’s temperature is very low, the hypothalamus responds
by……….
2. When the body temperature is very high, the hypothalamus responds by……….
1.2 Medications for fever
Learning Activity 1.2
A 20 years old female patient went to the health facility because she was worried
about the high fever, shivering, sweating. She was experiencing the symptoms
since yesterday. After admission, they found that her axillary body temperature
is 39.0oc, and directly she received two tablets that she swallowed immediately
before other intervention that were proposed.
Using Library textbooks, respond to the following questions
1. What is an antipyretic drug?
2. Describe the mechanism of action of Paracetamol?3. Identify the forms of Paracetamol.
CONTENT SUMMARY
Fever is treated by different medications including Acetaminophen or Paracetamol
which is a commonly used antipyretic. It is classified in antipyretic analgesic drugs.
Paracetamol is a chief of group of medication used to reduce fever by direct action
at the level of the hypothalamus and dilation of peripheral blood vessels, whichenables sweating and dissipation of heat.
Acetaminophen has the equal efficacy to reduce fever as ibuprofen, and aspirin,
however this aspirin and ibuprofen have anti-inflammatory properties that is why
acetaminophen is used as the primary therapeutic usefulness for the treatment
of fever in patients. Acetaminophen is rapidly engrossed from the gastrointestinal
tract, attainment peak levels in 0.5 to 2 hours. It is extensively metabolized in theliver and excreted in the urine, with a half-life of about 2 hours.
Caution should be used in patients with hepatic or renal impairment could restrict
with metabolism and excretion of the drug. Acetaminophen crosses the placenta
and goes into breast milk; it should be used vigilantly during gestation or lactationbecause of its potential adverse effects on the fetus or neonate.
The dosage of paracetamol depends on age and the level of fever. In Adults and
adolescents, 500mg to 1000 mg every 6 to 8 hours per day the maximum is 4000 mg
in 24 hours. Whereas for paediatric clients it is 10-15 mg/kg 4-6hrly. Paracetamol is
available in many forms. Acetaminophen is available as tablets, caplets, solutions,suppositories and injectable. It is a Pregnancy category B drug.

Adverse effects associated with acetaminophen use include headache, hemolytic
anemia, renal dysfunction, skin rash, and fever. Hepatotoxicity is a potentially fatal
adverse effects that is usually associated with chronic use and overdose and is
related to direct toxic effects on the liver. The dose that could prove toxic varies
with the age of the patient, other drugs that the patient might be taking, and the
underlying hepatic function of that patient. When overdose occurs, acetylcysteinecan be used as an antidote. Life support measures may also be necessary.
Self assessment 1.2
1. Identify at least 3 medications used to manage fever
2. What is the correct dosage of paracetamol in children?
A. 10mg/kg every 6hours
B. 10mg to 15mg/kg
C. 10mg to 20mg/kg
D. 10mg to 15mg /kg every 4 to 6 hrs.
3. Choose all correct answers: The adverse effects of paracetamol are
A. Headache,
B. Kidney dysfunction
C. Bleeding
D. Skin rashE. Pruritis
1.3. Overview on pathophysiology of pain
Learning Activity 1.3
These patients above are expressing the same health problem at different sites.
Use library textbooks and internet to respond to the following question.
a) What is pain?
b) How can the pain be assessed?
CONTENT SUMMARY
Pain is a displeasing sensory and emotional experience related to real or potential
tissue impairment. It arises with many disorders, diagnostic tests, and treatments.
It incapacitates and distresses more people than any single disease. It is the most
common reason for consultation in health care facilities. Sensory experience of
pain depends on the interaction between the nervous system and the environment.
The processing of noxious stimuli and the resulting perception of pain implicate the
peripheral and central nervous systems.
Among the nerve mechanisms and structures involved in the transmission of pain
perceptions to and from the area of the brain that interprets pain are nociceptors, or
pain receptors, and chemical mediators.
Nociceptors are receptors that are preferentially sensitive to a noxious stimulus.
Nociceptors are also called pain receptors; Nociceptors are part of complex
multidirectional pathways. These nerve fibers branch very near their origin in the
skin and send fibers to local blood vessels, mast cells, hair follicles, and sweat
glands. When these fibers are stimulated, histamine is released from the mast cells,
causing vasodilation. Nociceptors answer to high-intensity mechanical, thermal,and chemical stimuli.
Some receptors respond to only one type of stimuli; others, called polymodal
nociceptors, respond to all three sorts of stimuli. These highly specialized neurons
transfer the mechanical, thermal, or chemical stimulus into electrical action or
action potentials. The cutaneous fibers located more centrally further branch and
communicate with the paravertebral sympathetic chain of the nervous system
and with large internal organs. As a result of the connections among these nerve
fibers, pain is often accompanied by vasomotor, autonomic, and visceral effects.
In a patient with severe acute pain, for example, gastrointestinal peristalsis maydecrease or stop.
Physiologically, pain occurs when sensory nerve endings called nociceptors (also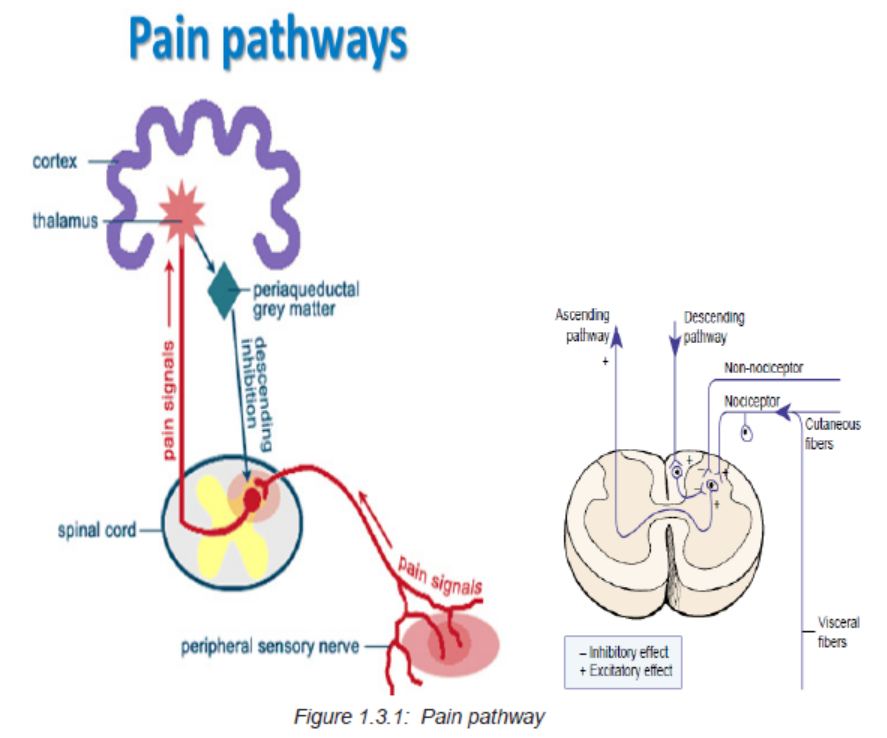
referred to as pain receptors) come into contact with a painful or noxious stimulus.
The resulting nerve impulse travels from the sensory nerve ending to the spinal
cord, where the impulse is rapidly shunted to the brain via nerve tracts in the spinal
cord and brainstem. The brain processes the pain sensation and quickly responds
with a motor response in an attempt to cease the action causing the pain.
Pain can be caused by a mechanical, chemical or inflammatory, or thermal
mechanism. Pain of mechanical origin can be caused by acute trauma, injury,or overuse. It may be constant, variable, or intermittent in nature and is affected
by movement and position. Pain of chemical or inflammatory origin is associated
with arthritis and other inflammatory disorders. It is often constant but responds to
positioning, therapy, rest, and gentle movement. Pain of thermal origin is the resultof excessive heat or cold.
If an acute pain sensation is intense enough, it can cause system-wide responses:
increased alertness; focused attention; the suppression of feeding, sleep, and
reproduction; and increased vascular tone, respiration, and blood sugar levels. If
pain persists or becomes chronic it can even change the circuitry in the central
nervous system. Medications are usually a part of the management regimen forchemical or inflammatory pain.
Table 1.3.1: Factors influencing pain perception
Factors influencing the pain response include past experiences to pain, anxiety,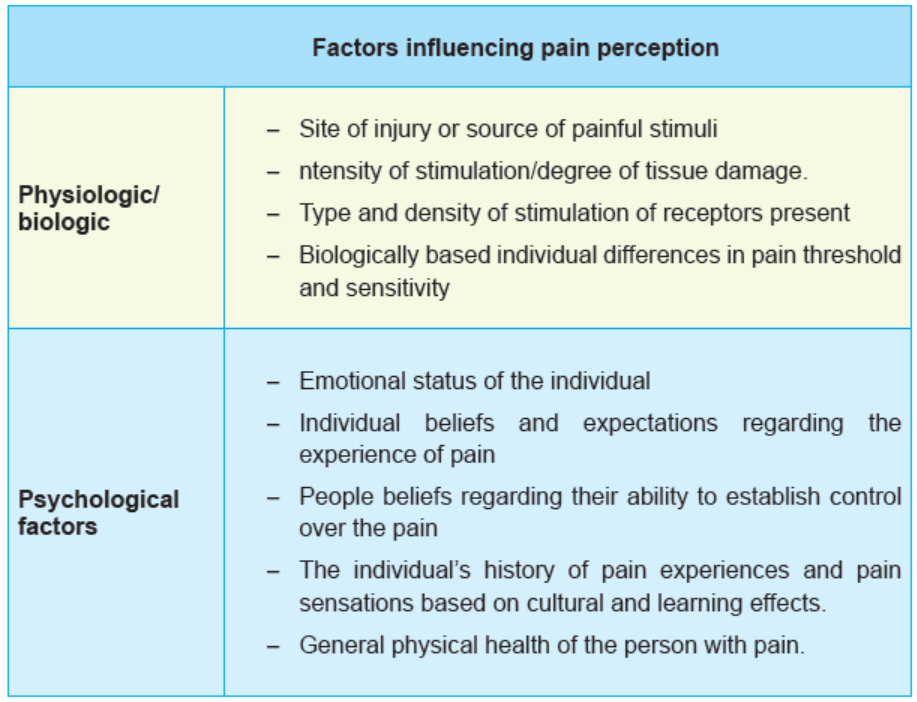
culture, age, gender, and expectations about pain relief. These factors may increase
or decrease the person’s perception of pain, upswing or reduced tolerance for pain,and affect the responses to pain.
Types of Pain
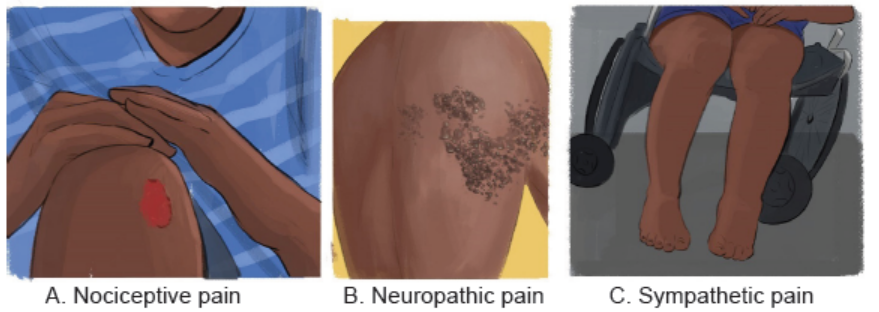
Figure 1.3.2: Types of Pain
Types of pain include nociceptive pain or Physiological pain (figure A) which is a
stimulation of sensory receptors for body and feels like aching, throbbing and sharp
such us stubbing of toe or case of damage or disease. It can be Superficial when
Skin and mucous membranes are involved, deep somatic when Muscles and joints
are involved or visceral when Organs are involved.
Neuropathic pain (figure B) is an abnormal reaction to stimuli caused by damaged
nerves. It can occur as a result of injury or infection. It can also flare up any
time without an obvious pain inducing event or factor. It is mostly a burning pain.
Sympathetic pain (figure C) is due to damage to sympathetic nerves. It is a bburning
pain with vasomotor instability and most of the time it is associated with rregional
sympathetic blocks.
The pain assessment begins by observing the patient carefully; noting the
patient’s overall posture and presence or absence of overt pain behaviors and
asking the person to describe, in his or her own words, the specifics of the pain
the words used to define the pain may ppoint toward the etiologic. The features
to consider in a whole pain assessment are the intensity, timing, location, quality,
personal meaning, aggravating and alleviating factors, and pain behaviors. Pain isa subjective phenomenon.
The highly subjective nature of pain Contests its assessment and management for
every health care provider. The report of pain is a social deal; thus, assessment
and management of pain require a good rapport with the person in hurt. In pain
assessment, the health care provider reviews the patient’s report of the pain and
other factors that may impact pain as well as the person’s response to pain liberation
strategies. Documentation of the pain level as graded on a pain scale becomes part
of the patient’s medical record, as does a record of the pain relief obtained frominterventions.
Pain assessment includes defining what level of pain relief the acutely ill patient,
believes is needed to recover quickly or improve utility, or what level of relief thechronically or terminally ill patient requires to maintain wellbeing.
Many scales were designed to assess the extent of pain at different levels. The
most commonly used scale is numeric scale that uses number to rate pain forpeople aged 9years and above.
By numerical scale, the patient rate verbally his/her client from 0 to 10 depending
of his/her feeling of pain then the health care provider classify to no pain, mild pain,
moderate pain, severe pain depending on the number the client has indicated andconsidering the figure below.
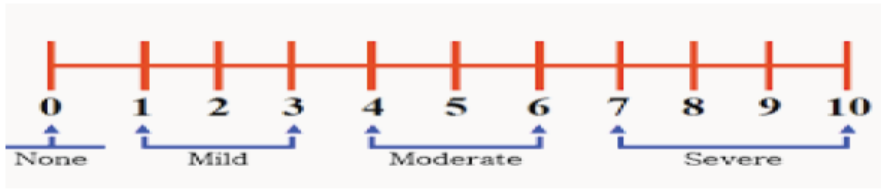
Figure 1.3.3: Numerical scale
Self assessment 1.3
1. Identify different types of pain
2. Using a pain scale, a patient who scored 6/10 is considered having (which
level of pain)?
3. Respond by True or false
1. The pain is disagreeable sensory and emotional experience related
only to diseases.
2. The pain is subjective in nature.3. Pain medications always cause heavy sedation
1.4 Medication for pain management
Learning Activity 1.4
A patient was operated yesterday. He declares that the site of incision hurts very
much. He did not sleep well the last night; he is crying in his bed.
Using library textbooks, respond to the following question
1. Identify classes of analgesics. Give an example for each class
2. What are the indications of morphine?3. List the contraindication of tramadol
Analgesia is defined as insensibility of pain. Medications used to relive pain are
analgesic or painkiller. Analgesics are classified as Opioid analgesics (strong opioid
and weak opioid) and non-opioid analgesics that include salicylates (example
aspirin), non-steroidal ant inflammatory drugs like ibuprofen and acetaminophen.Strong opioid analgesic includes morphine.
It is indicated to relieve acute or chronic moderate to severe and to complement
general, local, or regional anesthesia. It Binds with and activates opioid receptors
in brain and spinal cord to produce analgesia effect. Morphine has a half-life of 1.5to 2 hours, metabolized in the liver, excreted in the urine and bile
All forms of morphine are contraindicated in case of asthma, hypersensitivity
to morphine or its components, labor with premature delivery and respiratory
depression or upper airway obstruction. Some side effects may arise when
morphine is administered for example light-headedness, dizziness, sedation,
Nausea, vomiting, dry mouth, constipation, ureteral spasm, respiratory depression,
apnea, circulatory depression, respiratory arrest, shock, cardiac arrest. Morphineis available in various forms like capsules, Tablets, Oral Solution, Syrup, infusion.

Figure 1.5: Forms of morphine
The dosage of morphine varies considering the form, intensity of pain, route
of administration, indications and age of the patient. Tablets of morphine are
administered as initial dose of 15 to 30 mg orally every 4 hours as needed to manage
pain. For oral solution initial dose is 10 to 20 ml orally every 4 hours as needed.
For maintenance dose individually titrate to a dose that provides an appropriatebalance between pain management and opioid-related adverse reactions.
It is important to note that oral solution is available in 3 concentrations 2 mg/mL,
4 mg/mL, and 20 mg/mL; reserve use of 20 mg/mL concentration for patients who
are opioid-tolerant. For the parenteral use, intravenous dosage is 0.1 mg to 0.2
mg/kg via slow IV injection every 4 hours, intramuscular administration is 10 mg
IM every 4 hours alternatively, 2 to 10 mg IV as needed to manage pain (based on
70 kg adult). The dose of morphine is adjusted for pediatric patients .morphine isclassified in pregnancy category c.
Tramadol is among the commonly used weak opioid. It is used to relieve moderate
pain. It binds to the receptors and inhibits the reuptake of norepinephrine and
serotonin this enhance tramadol analgesic effect. In adults and adolescents over
age 16, it is administered 50 to 100 mg every 4 to 6 hr. as needed to manage pain
without exceeding 400mg daily. It is reduced in hepatic and renal conditions. Themaximum for patient aged 75 and above is reduced to 300 mg daily.
Tramadol should not be used for patient with history of addictions. Tramadol is
contraindicated for persons with alcohol intoxication; excessive use of centralacting
analgesics, hypnotics, opioids, or other psychotropic drugs; hypersensitivity
to tramadol or its components. Tramadol is a pregnancy category C drug. Tramadolis available in different forms: capsules (a), tablet (b), caplets(c) and injectable(d).
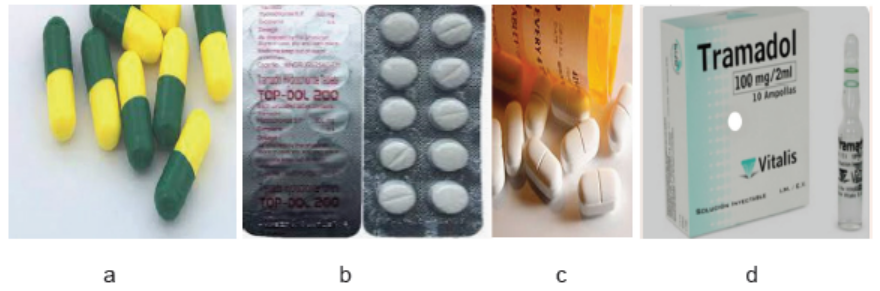
Figure 1.6: Forms of tramadol
Adjuvant drugs can be used to enhance the effects of pain medications, treat
concurrent symptoms, and provide analgesia for other types of pain. Adjuvant
analgesics are particularly useful when evidence of decreased opioid responsivenessis present
Self assessment 1.4
1. Choose the correct answer:
Medications used to treat pain include:
A. Amoxicillin, paracetamol, tramadol
B. Paracetamol, morphine, erythromycin
C. Morphine, ibuprofen, diclofenac
D. Amoxicillin, Ibuprofen, tramadol
2. What are the contraindications for morphine administration?
A. Malaria
B. Asthma,
C. Respiratory depression
D. B and C
3. Which one among the following pain killers is a weak opioid?
A. Paracetamol
B. Tramadol
C. AspirinD. Ibuprofen
1.5 World health organization (WHO) pain management ladder
Learning Activity 1.5
Using library text books and internet search respond to the following questions,
and note the findings
1. According to WHO Ladder, what are the levels of pain?2. Explain how each level is managed?
CONTENT SUMMARY
The optimal pain control is multimodal and individualized. This does not contradict
the value of the generalized WHO pain ladder, but clinicians should feel free to
modify it, as needed, for individual patients, reflecting modern pain practice. The use
of the pain ladder offers effective and cost-effective pain relief for patients suffering
from chronic pain. The WHO pain ladder describes pain in terms of intensity and
recommends that analgesics be prescribed starting at Step 1 using non opioid
analgesics, such as acetaminophen or non-steroidal anti-inflammatory drugs such
as ibuprofen If the pain persists or worsens, the clinician prescribes pain relievers
from Step 2, described as “weak opioids,” such us tramadol with or without a
non-opioid. At this point, if pain persists or worsens, the patient is administered a
“strong opioid,” at Step 3. Thus, pain therapy is based on pain intensity and patients
progress through the steps one by one, from lowest to highest, until pain relief isobtained.
Figure 1.7: WHO Ladder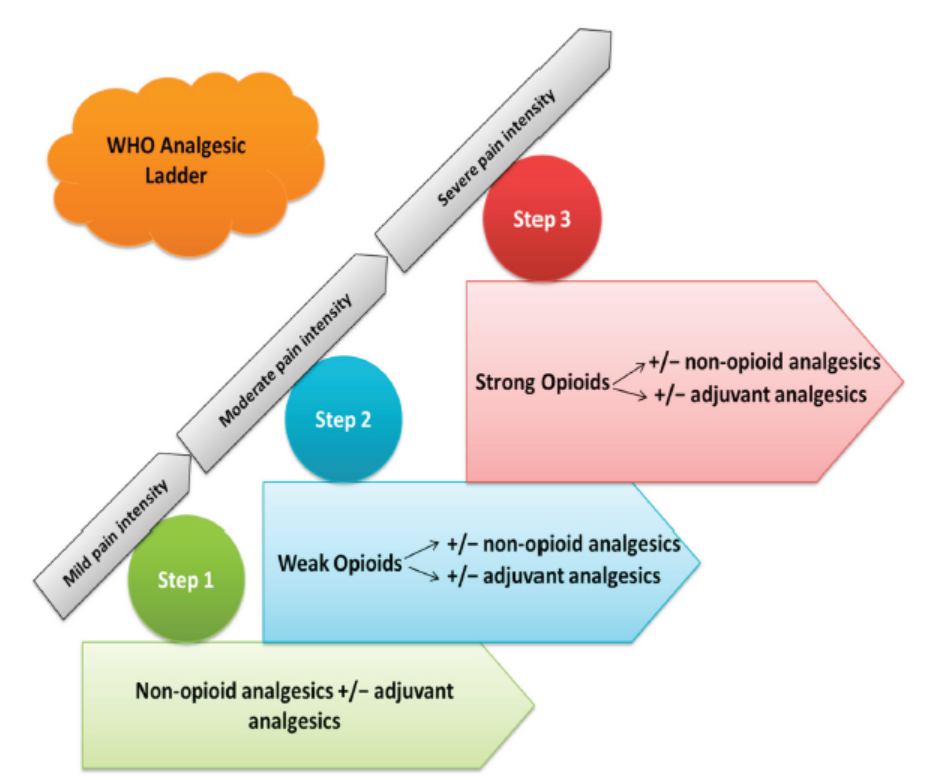
Reference: https://www.mdpi.com/1648-9144/55/9/584/htm
Myths about Pain
There are many barriers and myths regarding use of pain management medications
and on overall pain management that can result in negative patient outcomes. Even
if some myths are a part of the subculture of different medical disciplines, mistakenbeliefs are universal throughout the healthcare system.
Some persons believe that the healthcare providers do an adequate job of providing
adequate pain control. There is myth that pain medications always lead to addictionthis belief prevent some clients and health care provider to use painkillers frequently.
There is belief that Pain medications always cause heavy sedation, some clients
and professional refuse to administer prescribed dose thinking that there may be
sedation. Again, there is belief that some kinds of pain cannot be relieved. These
affect the client physically, emotionally when health care providers do not givepainkillers thinking that the pain may not be relieved.
Pain and suffering are character-building. Same people assume that in same
conditions of pain can empower the person with pain in personal resistance on
different life challenges thought pain does not affect how the person pursue theexternal life challenges.
Narcotic analgesics in older patients should be avoided. This is not true, older
person respond well on the effect of narcotic drugs if it has been administered withconsiderations for each patient specificity.
Self assessment 1.5
1. Which one among the following pain killers is a weak opioid?
A. Paracetamol
B. Tramadol
C. Aspirin
D. Ibuprofen
2. Which drug combination is true about the management of moderate pain
according to WHO pain management ladder
A. Paracetamol +Buscopan
B. Tramadol+ Buscopan
C. Morphine+ Paracetamol
D. Ibuprofen + Paracetamo3. Why do we need to use adjuvant with painkillers in pain management?
1.6. Anaesthetics
Learning Activity 1.6
Read the following case study and respond to the questions asked at the end.
Mr N.A was running on the road as usual sport as he used to do in the morning,
accidentally he falls down and a piece of glass severely cut him on the forearm.
A s you were around you approached him and advise him to directly to the health
facility, arriving there, the nurse said that Mr NA will need to be sutured. You
heard that she will give an injection of anaesthetics of the site of injury before
suturing.
Using library textbooks, respond to the following questions
1. What is an anaesthetic drug?
2. Why is it important to provide anaesthetic before suturing a wound?3. Enumerate categories of anaesthetics
Anesthetic is a drug used to cause complete or partial loss of sensation. It is called
local anesthesia when it blocks nerve preventing depolarization of nerve membranes,
blocking the transmission of pain stimuli and, in some cases, motor activity and it
is general when it causes induction of loss of consciousness, amnesia (loss of
memory), analgesia and loss of reflexes to allow surgical procedure performance.
Induction is the time from the beginning of anesthesia until achievement of surgical
anesthesia. Use of anesthetic agents suspends the sensation in parts of the body
they exist.
The anesthetics can be subdivided into general and local anesthetics, depending
on their site of action. General anesthetics are central nervous system (CNS)
depressants used to produce loss of pain sensation and consciousness. Sedatives
are agents given prior to induction of an anesthetic agent if indicated it leads on loss
of conscious and muscle relaxation to easier other procedures such us intubation.
Typically, the experience is smooth one and the patient has no recall of the events.
3 Stages of sedation
a) Minimal Sedation, the minimal sedation level is a drug-induced state during
which the patient can respond normally to verbal commands. Cognitive
function and coordination may be impaired, but respiratory and cardiovascularfunctions are not affected.
b) Moderate sedation is a form of anesthesia that may be produced intravenously.
It is defined as a depressed level of consciousness that does not impair the
patient’s ability to maintain a patent airway. And to respond appropriately tophysical stimulation and verbal command.
c) Deep Sedation is a drug-induced state during which a patient cannot be
easily aroused but can respond purposefully after repeated stimulation The
difference between deep sedation and anesthesia is that the anesthetized
patient is not arousal. Deep sedation and anesthesia are achieved when an
anesthetic agent is inhaled or administered intravenously.
Local anesthesia is the injection or application of a solution containing the local
anesthetic into/to the tissues at the planned incision site. Often it is combined with
a local regional block by injecting the nerves immediately supplying the area. Theadvantages of local anesthesia are as follows:
– It is simple, economical, and no expensive.
– Equipment needed is minimal.
– Postoperative recovery is brief.
– Undesirable effects of general anesthesia are avoided.– It is ideal for short and superficial surgical procedures.
Local anesthesia is often administered in combination with epinephrine. Epinephrine
constricts blood vessels, which prevents rapid absorption of the anesthetic agent
and thus prolongs its local action. Rapid absorption of the anesthetic agent into the
bloodstream, which could cause seizures, is also prevented. Local anesthesia isthe anesthesia of choice in any surgical procedure in which it can be used.
However, contraindications include high preoperative levels of anxiety, because
surgery with local anesthesia may increase anxiety. A patient who requests general
anesthesia rarely does well under local anesthesia. For some surgical procedures,
local anesthesia is impractical because of the number of injections and the amount
of anesthetic that would be required. The skin is prepared as for any surgical
procedure, and a small gauge needle is used to inject a modest amount of theanesthetic into the skin layers.
This produces blanching or a wheal. Additional anesthetic is then injected in the
skin until an area the length of the proposed incision is anesthetized. A larger,
longer Needle then is used to infiltrate deeper tissues with the anesthetic. Local
anaesthetics include various classes like esters examples procaine, benzocaine,
cloroprocaine, procaine, tetracaine and amides class where we find buvicaine,
lidocaine, and mepivacaine. Local anesthetics block the depolarization of nerve
membranes, preventing the transmission of pain sensations and motor stimuli(Figure B)
Local anesthetics are administered to deliver the drug directly to the desired area
and to prevent systemic absorption, which could lead to serious interruption ofnerve impulses and response
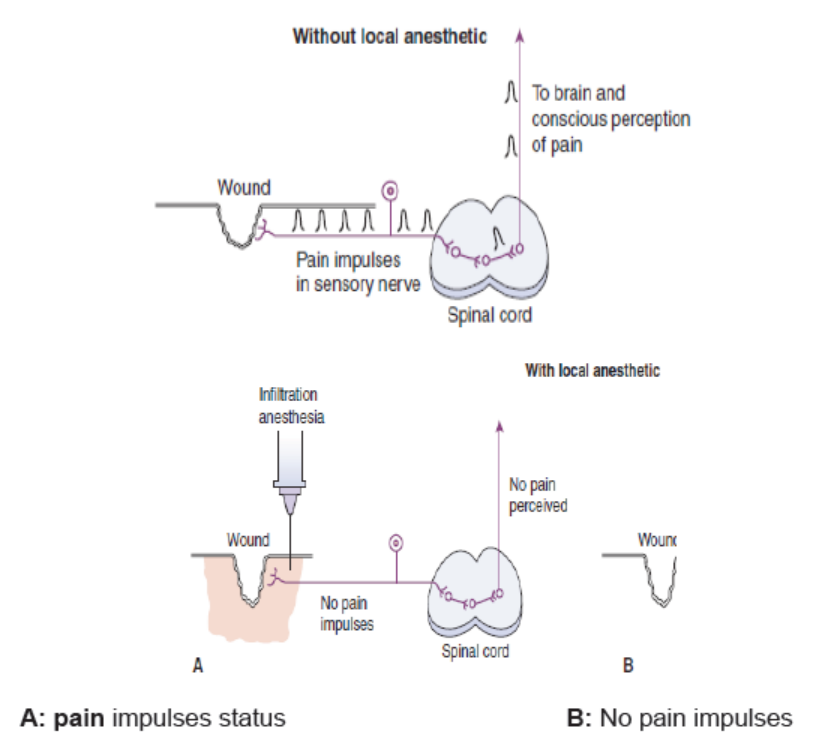
Figure 1.6.1: pain impulse transmission
Local anesthetics
Bupivacaine (marcaine), etidocaine (duranest) those anesthetics are
administered by infiltration peripheral nerve block the duration is 2–3 times longer
it is used cautiously in patients with known drug allergies or sensitivities. While
using bupivacaine should consider a period of analgesia persists after return of
sensation; therefore, need for strong analgesics.
Procaine (novocaine) is administered subcutaneously, intramuscularly,
intravenously, or spinal.it has low toxicity; inexpensive it can cause some
idiosyncrasies skin rash poor stability. There is a need to observe for reaction such
us hypotension, bradycardia, weak pulse. Usually administered with epinephrine,
causing vasoconstriction, thereby slowing absorption and prolonging nervedeadening effect
Tetracaine (pontocaine) is administered to topical infiltration nerve block it causes
topical infiltration nerve block but can cause some idiosyncrasies skin rash poor
stability, as potent as procaine usually administered with epinephrine.
Lidocaine (xylocaine) and mepivacaine (carbocaine); Lidocaine can be
administered in topical or injection, it is Rapid Longer duration of action, while
administer Lidocaine they should consider, Useful topically for cystoscopy Injected
for use in dental work and surgery, Observe for untoward reaction, drowsiness,
depressed respiration. Lidocaine is currently widely used local anaesthesia; it acts
by blocking neuronal pain impulses. It may be injected as a nerve block for spinal
and epidural anesthesia. It blocks sodium channels located within the membranesof neurons.

Figure1.6.2:Local Anesthetics
Lidocaine is available in injectable forms(A), Cream for topical use( B),spray (C) and
patches (D). Their use will depend on the client, procedure to be performed and the
desired effect. Solutions of lidocaine containing preservatives or epinephrine with
vasoconstriction effect are intended for local anesthesia only and must never begiven parenteral for dysrhythmias.
It is not advisable to apply topical lidocaine to large skin or broken areas as this
led to systemic absorption. It should not be in contact with eyes. Lidocaine is not
indicated in case of hypersensitivity to amide local anesthetics. Application or
injection of lidocaine anesthetic is also contraindicated in the presence of severe
trauma or sepsis, dysrhythmias, sinus bradycardia, and severe degrees of heart
block. Lidocaine is a pregnancy category B drug.
Local anaesthetics are generally very safe and serious problems are rare. However,
some discomfort when the injection is given, a tingling sensation as the medication
wears off, possibly some minor bruising, bleeding or soreness where the injection
was given Some people experience experience temporary side effects from a
local anesthetics, such as, dizziness, headaches, blurred vision, twitching muscles,
continuing numbness, weakness or pins and needles. In very rare cases, you could
have an allergic reaction to the local anesthetic or develop serious problems, such
as seizures or a cardiac arrest. Precautions should be taken while injecting localanesthesia.
Self assessment 1.6
1. List at least 4 advantages of using local anesthetics
2. Identify at least 5 complications of local anesthetics
3. The following are the forms of Lidocaine except
A. Tablets
B. Sprays
C. InjectableD. Cream
1.7. Overview on physiology of inflammation
Learning Activity 1.7
1. What should be the problem on those images above ?
2. What are the causes of inflammation?( Please refer to library textbooks/
internet)3. Explain the physiology of inflammation
CONTENT SUMMARY
In case the body get exposed to various stimuli like physical injury, exposure to toxic
chemicals, extreme heat, invading microorganism or cell death, it reacts by defense
mechanism called inflammation. The latter is considered nonspecific defense
mechanism as it proceds in the same way regardless of the cause that triggered
it. The main purpose of infammation is to recover the body from injury or destroy
microrganism. By neutralizing the foreign agent and removing cellular debris and
dead cells, repair of the injured area is able to proceed at a faster pace. Whether
the damage is due to pathogens, chemicals, or physical trauma, the damaged
tissue releases a number of chemical mediators that act as an alarms to notify the
surrounding area of the injury.
Chemical mediators of inflammation include histamine, leukotrienes,
bradykinin, complement, and prostaglandins. Some of these inflammatory
mediators are important targets for anti-inflammatory drugs. Signs of inflammation
include swelling, pain, warmth, and redness of the affected area. Inflammation may
be classified as acute or chronic. Acute inflammation has an immediate onset and
8 to 10 days are normally needed for the symptoms to resolve and for repair to
begin. If the body cannot contain or neutralize the damaging agent, inflammationmay continue for long periods and become chronic.
Self assessment 1.7
1. What happens to the human body when an inflammation doen’t resolve?2. What are Chemical mediators of the inflammation?
1.8 Anti-Inflammatory Drugs
Learning Activity 1.8
Use library textbooks and respond to the following questions:
1. Enumerate commonly used anti-inflammatory drugs
2. Explain the mechanism of action of Nonsteroidal anti-inflammatory drugs3. List the side effects of anti-inflammatory drugs
CONTENT SUMMARY
Anti-inflammatory agents are drugs that block the effects of the inflammation.
The inflammatory response is the body’s nonspecific response to cell injury,
resulting in pain, swelling, heat, and redness in the affected area. Anti inflammatory
drugs have antipyretic effect by blocking fever, often by direct effects on the
thermoregulatory center in the hypothalamus or by blockade of prostaglandin
mediators. Antinflammatory drugs include nonsteroidal anti-inflammatory drugs(NSAIDs), salicylates, acetic acid classes
Nonsteroidalanti-inflammatory drugs are that widely used. They act by blocking
prostaglandin synthesis and acting as anti-infl ammatory, antipyretic, and analgesic
agents. The NSAIDs are rapidly absorbed from the GI tract, reaching peak levels in
1 to 3 hours. They are metabolized in the liver and excreted in the urine. NSAIDs
cross the placenta and cross into breast milk. Therefore, they are not recommended
during pregnancy and lactation because of the potential adverse effects on the
fetus or neonate.the general side effects of NSAD include :Bleeding ,Gastric abset
and reduced kidney function . There are two main classes of antinflammatory
drugs including propionic acids and acetic acids.Among the propionic acid drug;ibuprofen is the mostly used drug to treat inflammation.
Inhibits prostaglandin synthesis by blocking Cyclooxygenase-1 and -2 receptor
sites, leading to an anti-inflammatory effect, analgesia, and antipyretic effects for
this it decreases swelling, pain, inflammation and fever. I t is indicated to relief of
the signs and symptoms of rheumatoid arthritis and osteoarthritis; relief of mild tomoderate pain; treatment of primary dysmenorrhea and fever.
Ibuprofen is available as tablets (A, B, C) either 200mg or 400mg per tablet and
oral solution (D, E) In adults, ibuprofen dose is 400 mg tid or qid with the maximum
of 1,200 mg/day and for pediatric clients the dosage is 5 - 10mg/kg 6-8hrly the
maximum being 30mg/kg/day. Ibuprofen has a half-life of 1.8 to 2.5 hours. It is
metabolized in the liver and excreted in the urine.The commonly adverse effect
of ibuprofen includes headache, dizziness, somnolence, fatigue, rash, nausea,
dyspepsia, bleeding, drug-induced peptic ulcer, constipation. Ibuprofen is apregnancy category C before the first 30weeks of gestation and D from 30 weeks.

Figure 1.8.1 Iburpfen forms
Diclofenac and indomethacin are acetic acid derivative Nonsteroidal anti
inflammatory drugs. Diclofenac is a phenylacetic acid derivative while indomethacin
is an indoleacetic acid derivative. Diclofenac is Analgesic, anti-inflammatory
that acts by blocking the activity of cyclooxygenase, the enzyme needed to
synthesize prostaglandins, which mediate inflammatory response and cause
local pain, swelling, and vasodilation. By blocking cyclooxygenase and inhibiting
prostaglandins, Diclofenac reduces inflammatory symptoms. This mechanism also
relieves pain because prostaglandins promote pain transmission from periphery tospinal cord.
Diclofenac is indicated for the treatment of acute and chronic pain associated with
inflammatory conditions in adults. In adults, diclofenac is prescribed as 50 mg t.i.d.,
p.r.n or bid–qid with the maximum of 200 mg per day, 100 mg for first dose only. The
half-life is 2hours. The dose is reduced, if needed, for elderly patients and those
with serious renal dysfunction. For injectable, the dosage is 2mg/kg/day resulting
approximately in 1ampoule bid the half-life being 1.15 hours for suppositories
100mg bid is prescribed and the half is 3 to 6 hours. Patches for topical application,
one patch is applied bid to the most painful area 12 hours.
Diclofenac is contraindicated for persons with active GI bleeding or ulcers; asthma
attacks, rhinitis, or urticarial from aspirin or other NSAIDs, hypersensitivity to
diclofenac or NSAIDs; treatment of perioperative pain after coronary artery bypass
grafting. It is a Pregnancy category B drug. Indomethacin Relief of moderate to
severe pain in PO 25 to 50 mg b.i.d. to q.i.d., increased by 25 or 50 mg daily every
week, if needed the maximum being 200 mg daily. Diclofenac comes as an oral
capsule (A, B), oral tablet (C), injectable (D, E) topical gel(G), suppository(H),
transdermal patch (I), topical solution, and powder packets for oral solution (Figure
1.8.2)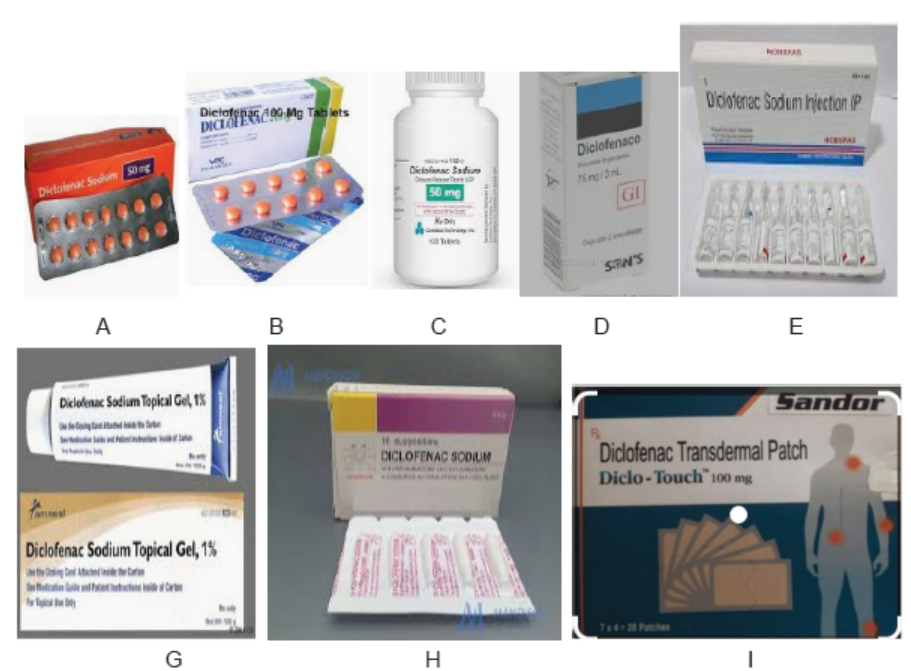
Figure 1.8.2: Diclofenac forms
Salicylates are salicylic acid compounds used as anti-infl ammatory, antipyretic,
and analgesic agents.They inhibit the synthesis of prostaglandin, which is an
important prostaglandin mediator of pyrogens at the thermoregulatory center
of the hypothalamus.They are most popular and oldest anti-inflamamtory drugs
with antipyretic and analgesic properties. They are generallyavailable without
prescription and are relatively nontoxic when used as directed. Salicylates are
readily absorbed directly from the stomach, reaching peak levels within 5 to 30
minutes. They are metabolized in the liver and excreted in the urine. The half-lifeof 15 minutes to 12 hours, depending on thesalicylate.
Salicylates cross the placenta and enter breast milk; they are not indicated for
use during pregnancy or lactation because of the potential adverse effects on the
neonate and associated bleeding risks for the mother.S alicylates should not be used
by people with known allergy to salicylates or other nonsteroidal anti-inflammatory
drugs and those with active bleeding. It is the same for patients presenting nasal
polyps, those hostory of asthma, chiken pox or influenza,surgery or othe invasive
procedures within 1 week as this may lead to bleeding . They are not used by
pregnant and lactating mothers and persons with reanl impairement.
The adverse effects associated with salicylates results from its direct
effects on the stomach and these include nausea, dyspepsia, heartburn,
epigastric discomfort or its effect on clotting. When administered at higher
levels, a salicysm syndrome arises with dizziness,ringing in ears,difficult in
breathing,nausea,vomiting,diarrhea and mental confusion. Salicylate toxicity also
occur when a dose of 20to 25g in adults or 4gin children is administered and the
signs include hyperpnea,tachypnea,hemorrage,excitement,confusion, pumonary
edemaconvulsion, tetany,acidosis,fever,cardiovascular,renal and respiratory
collapse.
Aspirin is the most commonly used salicylate. At lower level, it affects platelet
aggregation by inhibiting the synthesis of thromboxane A2, a potent vasoconstrictor
that normally increases platelet aggregation and blood clot formation. At higher
levels, aspirin inhibits the synthesis of prostacyclin, a vasodilator that inhibits
platelet aggregation.Salicylates are indicated for the treatment of mild to moderate
pain, fever, and numerous inflammatory conditions, including rheumatoid arthritis
and osteoarthritis.
Aspirin inhibits the synthesis of prostaglandins by blocking the effects of pyrogens
at the hypothalamus and inhibiting platelet aggregation by blocking thromboxane
A2. The management of mild to moderate pain, fever, inflammatory conditions;
reduction of risk of transient ischemic attack or stroke and reduction of risk
of myocardial infarction. The half-life of aspirin is 15 minutes to 12 hours.It is
metabolized in the liver and excreted in the urine. pirin is available in oral tablet of75mg,100mg and 500mg.
In adults the dose is 350–650 mg every 4 h with the maximum of 4 gr per day. For
children ages 2 to 14, 10 to 15 mg/kg/dose every 4 hr, p.r.n., up to 80 mg/kg daily.
Pregnancy category: D. The adverse effects of aspirin include nausea, vomiting,heartburn, epigastric discomfort, occult blood loss, dizziness, tinnitus, acidosis.

Figure 1.8.3: Aspirin forms
Self assessment 1.8
Read carefully the text
You are working as nurse at RUBONA health center and you receive 2 clients
in consultation room. The client’s name is Mr. H aged 34 years old a man, who
complains the swelling on the left leg after has been bitten by a wood 3days
ago, while he was cutting a tree in his farm. He has joint pain for 1 week has no
fracture but the site is very hot and pain full with swelling. He has no history of
other diseases.
The second client is Miss N. aged 19 years old, who complains pelvic pain with
prostration but has normal vital signs. While you are taking history, she tells
you that she is on her first day of menstruation and she started feeling the pain
soon before menses start. Data obtained from the assessment and physical
examination revealed no any other problems noticed except the tenderness in
hypogastric region.
You are requested to manage these 2 patients’ problems.
1. Which problem does Mr. H has? Discuss how the problems of Mr. H should
be managed?
2. A. Discuss how the problems of Miss N can be treated?B. Is there any drug to avoid if yes why?
1.9 Medications for common cold and rhinitis
Learning Activity 1.9
Using library textbooks and internet, take note and respond to the following
questions.
1. What are the group of medication for common cold management?
Give an example of each group.2. Describe the mechanism of action of anti-histamines drugs.
CONTENT SUMMARY
The treatment of common cold consists of antihistamines, anti-inflammatories
and decongestant drugs. The signs and symptoms of allergic rhinitis resemble
those of the common cold. They include tearing eyes, sneezing, nasal congestion,
postnasal drip, and itching of the throat. The Goal of treating rhinitis aims at
preventing its occurance and relieve the present symptoms.The drugs used to treatrhinitis are categorized into two groups.
The Preventers which drugs used as prophylaxis include antihistamines,intranasal corticosteroids, and mast cell stabilizers.

Figure 1.9.1. Histamine action and body’s reactions
The Relievers are used to provide immediate, though temporary, relief for acute
allergy symptoms once they have occurred. Relievers include the oral and
intranasal decongestants, usually drugs from the sympathomimetic class. In
addition to treating allergic rhinitis with drugs, nurses should help patients identify
sources of the allergies and recommend appropriate interventions. These may
include removing pets from the home environment, cleaning moldy surfaces, using
microfilters on air conditioning units, and cleaning dust mites out of bedding, carpet,
or couches.
The histamine receptors responsible for allergic symptoms are called H1 receptors.
The other major histamine receptor, H2, is found in the gastric mucosa and is
responsible for peptic ulcers .Antihistamines are drugs that selectively block
histamine from reaching its H1 receptors, there by alleviating allergic symptoms.
Because the term antihistamine is nonspecific and does not indicate which of the
two histamine receptors are affected, H1-receptor antagonist is a more accurate
name.
In clinical practice, as well as in this text, the two terms are used interchangeably.
The most frequent therapeutic use of antihistamines is for the treatment of
allergies. These medications provide symptomatic relief from the characteristic
sneezing, runny nose, and itching of the eyes, nose, and throat of allergic rhinitis.
Antihistamines are often combined with decongestants and antitussives in OTC cold
and sinus medicines. The viruses that cause common cold cause inflammation of
the upper respiratory tract, by initiating the release of histamineand prostaglandins.
The inflamation leads to the increase engorgement of mucous membranes by blood
leading to tissue swelling and an increase in mucous production consequently, sinus
pain, nasal congestion, runny nose,sneezing,watery eyes,scratching the throat and
headache. In some people the eustachian tube’s outlet is blocked and the ear
becomme stuffed and painfull and more likely this results in otitis media.Rhinitis
is an inflammation of nasal cavity. This condition occurs when the upper airways
respond to a specifi c antigen like dust,pollen. The inflammatory response cause
sneezing,nasal congestion, stuffness and waterly eyes. While the treatment of the
treatment of rhinitis is antihistamines.
Antihistamines are drugs that block the release or action of histamine, a chemical
released during inflammation that increases secretions and narrows airways
in antihistamines drugs. Antihistamines are found in multiple out of the counter
preparations that are designed to relieve respiratory symptoms and to treat
allergies. When choosing an antihistamine, the individual patient’s reaction to the
drug is usually the governing factor.
Because first-generation antihistamines have greater anticholinergic effects with
resultant drowsiness, a person who needs to be alert should be given one of the
second-generation, less-sedating antihistamines. Because of their out of the counter
availability, these drugs are often misused to treat colds and influenza. Those
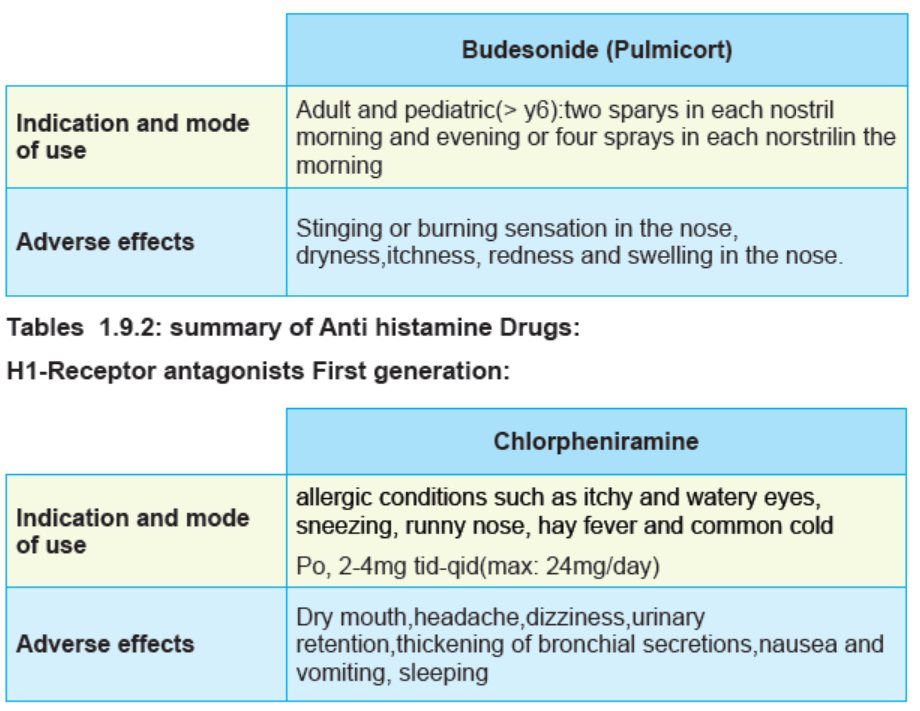
drug include the following: brompheniramine, carbinoxamine, chlorpheniramine,
clemastine, cyclizine, cyproheptadine, dexchlorpheniramine, dimenhydrinate,
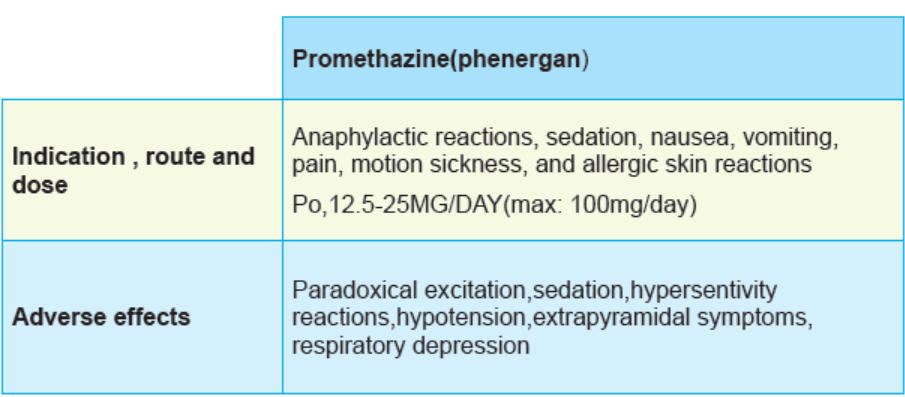
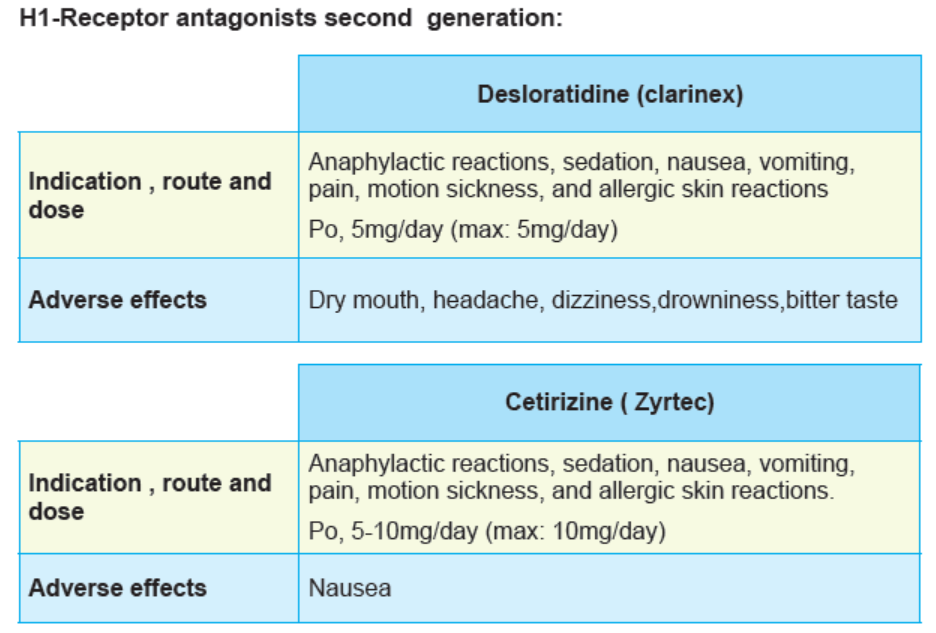
diphenhydramine, promethazine, triprolidine these are in the first Generation.
Azelastine, cetirizine, desloratadine, fexofenadine, levocetirizine, loratadine
are in the second generation. Chlorpheniramine is a commonly used drug
in adults to treat simple common cold and rinitis while in moderate and chroniccases,desloratidin is prefered.

Figure 1.9.2. Anti histamine Drugs
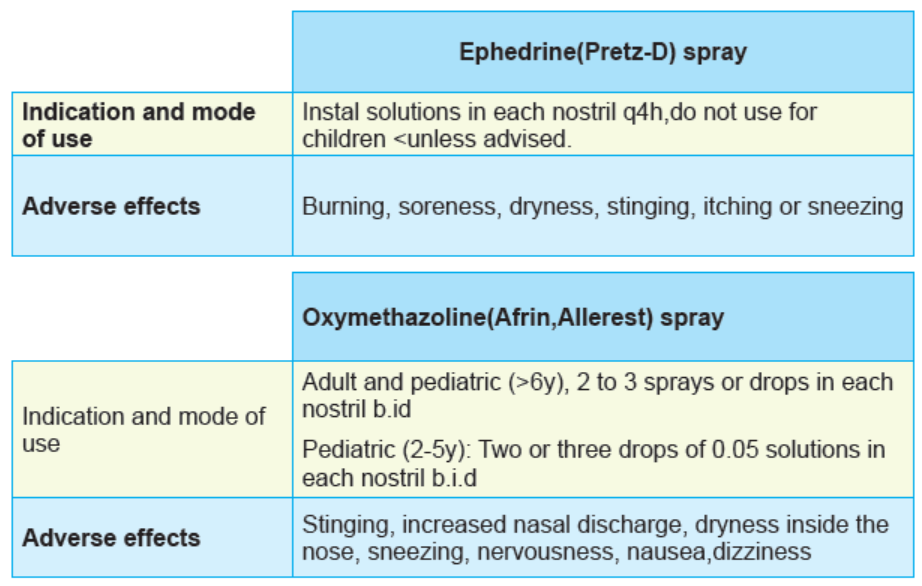
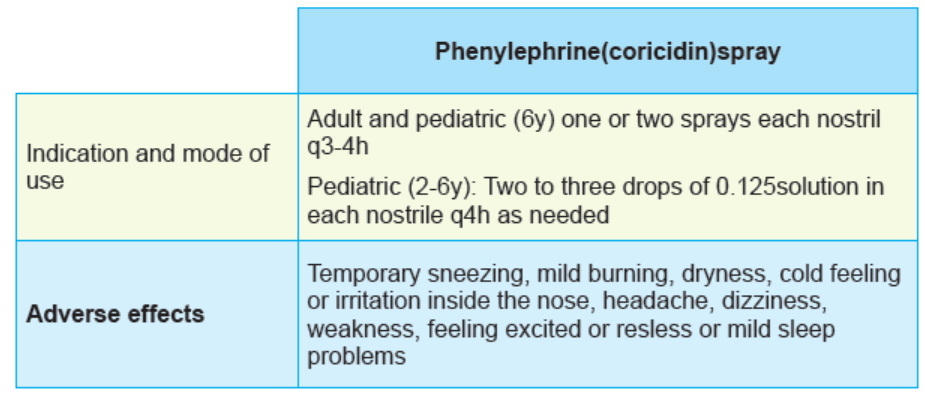
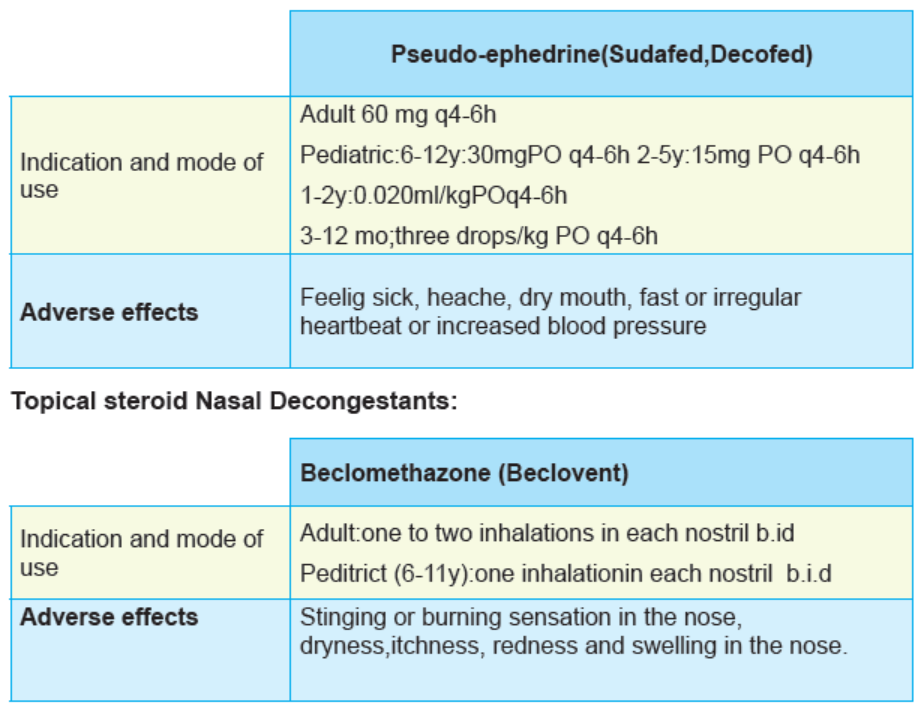
Decongestants are drugs that decrease the blood flow to the upper respiratory
tract and decrease the overproduction of secretions. Decongestants decrease
the overproduction of secretions by causing local vasoconstriction to the upper
respiratory tract .This vasoconstriction leads to a shrinking of swollen mucous
membranes and tends to open clogged nasal passages, providing relief from the
discomfort of a blocked nose and promoting drainage of secretions and improved
airflow.
An adverse effect that accompanies frequent or prolonged use of these drugs
is a rebound congestion, technically called Rhinitis medicamentosa. The
reflex reaction to vasoconstriction is a rebound vasodilation, which often
leads to prolonged overuse of decongestants.They existe topical nasol
decongestant with ephedrine as prototype,oxymetazoline,phenylephrine,oral
decongestants pseudoepinephrine,topical nasol steroid decongestants such usbeclomethasone,budesonide,dexamethasone ,flunisolide is prototype.

Figure 1.9.3. Anti Decongestant Drugs
Table1.9.1: Decongestant drugs and their indications

Self assessment 1.9
Choose the best answer
1. Which drug among the following drugs is used in the treatment of common
cold?
A. Acetaminophen
B. Tramadol
C. Chlorphenamine
D. Cimetidine
2. Among the drugs below, which one is an intranasal decongestant?
A. Promethazine
B. Beclomethasone
C. Desloratidine
D. Omeprazole
3. What is the MOST COMMON side effect of nasal decongestant?
A. Nose bleeding
B. Runny nose
C. GI upsetD. Burning sensations
1.10. Overview on pathophysiology of seizures
Learning Activity 1.9
1. Based on your observations what should be the problem expressed in pictures?
2. Using library textbooks, describe the physiology of seizures?
CONTENT SUMMARY
Seizures are uncontrolled electrical activity in the brain that may lead to symptoms
ranging from mild loss of attention to violent muscular contractions that can
lead to death. Everyone has the potential to have seizures or convulsion. The
seizures occur when there is an abnormal electrical activity in the brain. They are
also known as convulsions, but not all seizures produce convulsive behavior which
is uncontrollable muscle contractions names as atonic seizures, Where there is aloss of muscular tone or strength.
The seizures’ symptoms produced dependent on which part of the brain is
experiencing the abnormal electrical activity. Seizures are generally short
lived from 15 seconds to 15 minutes however; there is a life-threatening type
of seizure, status epilepticus, in which the seizure does not end. A diversity of
conditions and substances can Cause seizures. Common trigger causes seizures
include congenital abnormalities of the brain, illicit drug use, fever, brain tumors
and metabolic imbalances, such as high levels of glucose or sodium. The epilepsy is
known as a condition in which a person experiences repeated seizures, due to anoverall electrical disturbance in the brain.
The terms convulsion and seizure are often used interchangeably and basically
have the same meaning, each different type of seizure disorder is characterized
by a specific pattern of events as well as a different pattern of motor or sensory
manifestations Partial or focal seizures arise from a localized area in the brain andcause specific symptoms.
A partial seizure can spread to the entire brain and cause a generalized seizure.Partial seizures include simple seizures in which consciousness is not impaired.
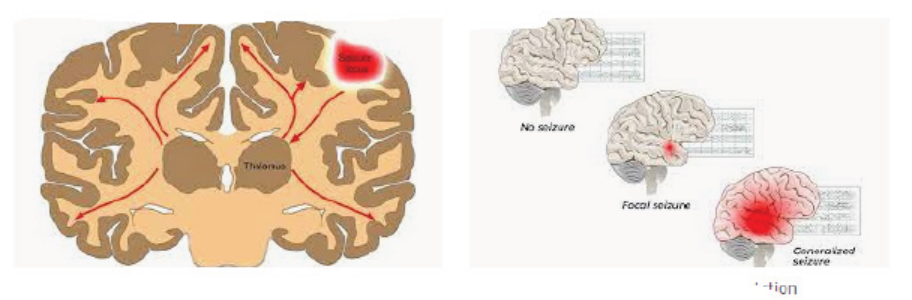
Figure 1.10.1 seizures transmission
Psychomotor seizures occur most often in children 3 years of age through
adolescence. The individual may experience an aura with perceptual alterations,
such as hallucinations or a strong sense of fear. Repeated coordinated but
inappropriate movements, such as clutching, kicking, picking at clothes, walkingin circles, and licking are characteristic. Generalized seizures include absence,
myoclonic, and tonic–clonics. Manifestations of a generalized tonic–clonic seizure
include alternate contraction (tonic phase) and relaxation of muscles, a loss of
consciousness, and abnormal behavior.
Myoclonic seizures involve sudden, forceful contractions involving the musculature
of the trunk, neck, and extremities. Absence seizures, previously referred to as
petit mal seizures, are seizures characterized by a brief loss of consciousness
during which physical activity ceases. The seizures typically last a few seconds,occur many times per day, and may go unnoticed by others.
Classification of seizures
If patients have a lower tolerance to environmental triggers; seizures may occur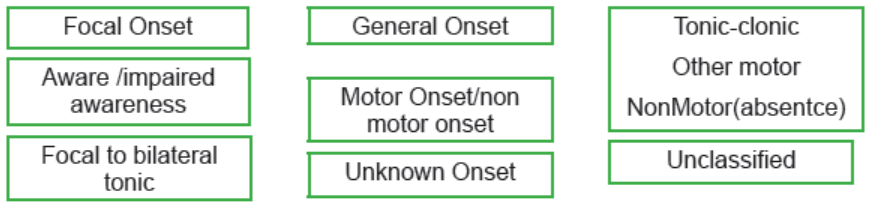
when they are sleep deprived, are exposed to strobe or flickering lights, or have a
fluid and electrolyte imbalance. Seizure disorders occur throughout the life span.
Those who experience seizures, about half will experience their first seizure before
age 10. Seizure in pregnant woman requires special education to either prevent
conception or to safely prevent seizures during pregnancy. Seizure disorders in
the older adult are most often associated with an underlying comorbid condition.
Cerebrovascular disease, especially stroke, accounts for one third of all cases andis the most common risk factor for the development of epilepsy after age 6.
Febrile seizures are defined as seizures associated with fever in the absence of
central nervous system infection. Febrile seizures are common among children
and unusual in adults. In adults with hyperthermia above 40.5oc, nerve damage
coagulation of cell proteins leads to convulsions. The developing brain of child is
very sensitive to effects of mild to high fever that led to abnormal discharge of
electrical activity within the brain. The sudden rise in temperature seems to be
more important than the degree of temperature. The seizure may occur with the
initial onset of fever before a child’s caregiver is even aware the child is ill. Mostfebrile seizures are generalized when they involve the whole body.
In other words, the whole body may be involved and Stiffening of the entire body
Jerking of the arms and legs, complete lack of response to any stimuli, eyes
deviated, staring, rolling back, moving back and forth, tightness of the jaws and
mouth, urinary incontinence, noisy breathing, labored, slower than normal (unusualfor a child to stop breathing completely).
Although it may seem like infinity if you are observing a seizure, most of these
episodes last only 1-5 minutes. Afterward, the child is typically drowsy but usually
starts to become responsive within 15-30 minutes. Seizures may be focal when onepart of the body is involved.
Self assessment 1.10
1. Which of the following mostly triggers the seizures
A. Fever
B. Running
C. Pregnancy
D. Old age
2. What are the manifestations of Tonic- clonic seizures? Choose the correct
answer
A. Acute kidney injury
B. Abnormal bleeding
C. Loss of consciousness
D. Severe pain
3. True or False
A. The seizures occur when there is an abnormal electrical activity in the brain
B. Partial seizures can lead to generalized seizures
C. The young children are at higher risk of seizures associated with fever
because their developing brain is less sensitive to effects of mild to highfever.
1.11. Medications for seizures
Learning Activity 1.11
Use library textbooks, take note and respond to the following questions
1. What are the class of antiseizures? Give an example of medication on each
class.2. What are the common side effects of antiseizures drugs?
CONTENT SUMMARY
Medications for the management of seizure disorders are called antiseizures. Most
anti-seizures have specific uses; that is, they are of value only in the treatment
of certain types of seizure disorders. There are four categories of drugs used
as anticonvulsants: barbiturates, benzodiazepines, hydantoins, and the
succinimides, generally, anticonvulsants reduce the excitability of the neurons
(nerve cells) of the brain. When neuron excitability is decreased, seizures are
theoretically reduced in intensity and frequency of occurrence or, in some instances,
are virtually eliminated.
Barbiturates medications are the chemical derivatives of barbituric acid. These
drugs reduce neuronal excitability primarily by increasing GABA-mediated inhibition
through GABA RECEPTORS. They act on spinal cord, brainstem and the
Heightened GABAergic transmission at motor neurons in the spinal cord relaxesmuscles and suppresses ref exes:
1.11.1. Table: Phenobarbital
Benzodiazepine antiseizures drugs act by potentiating GABA binding by increasing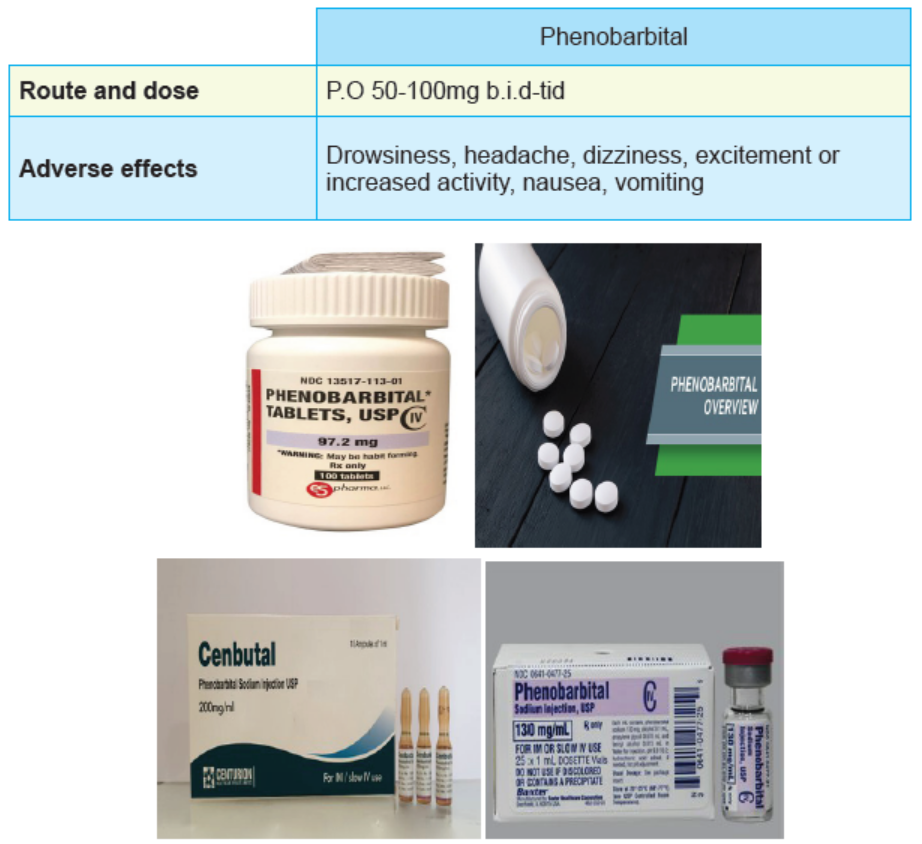
the frequency of channel opening in the presence of low GABA concentrations,
and, at GABA concentrations similar to those in synapses receptor deactivation is
slowed. Benzodiazepines drugs are not only used control seizures but also for the
treatment of anxiety, skeletal muscle spasms, and alcohol withdrawal symptoms.
Most benzodiazepines are given orally Those that can be given parenterally, such
as diazepam (Valium) and lorazepam (Ativan), should be monitored carefully owing
to their rapid onset of CNS effects, and possible respiratory depression.
Benzodiazepines are contraindicated in patients with known hypersensitivity to the
drugs. Benzodiazepines are also contraindicated in patients with acute narrowangle
glaucoma, psychosis, liver or kidney disease, and neurological disorders.
Benzodiazepines should be used cautiously during pregnancy
Adverse effects of benzodiazepines are drowsiness, ataxia, impaired judgment,
dry mouth, fatigue, visual disturbances, rebound insomnia, and development of
tolerance. Overdosage may result in CNS and respiratory depression as well
as hypotension and coma. Gradual withdrawal of these drugs is recommended.
Although the use of any of the benzodiazepines during pregnancy is likely to cause
fetal abnormalities, flurazepam is entirely contraindicated during pregnancy. As it is
category D, and in elderly or debilitated patients.
Benzodiazepines increase CNS depression with alcohol and omeprazole. They
also increase pharmacological effects if combined with cimetidine, disulfiram, or
hormonal contraceptives. The effects of benzodiazepines decrease with theophyllineand ranitidine.
Tables1.11.2. Benzodiazepine antiseizures
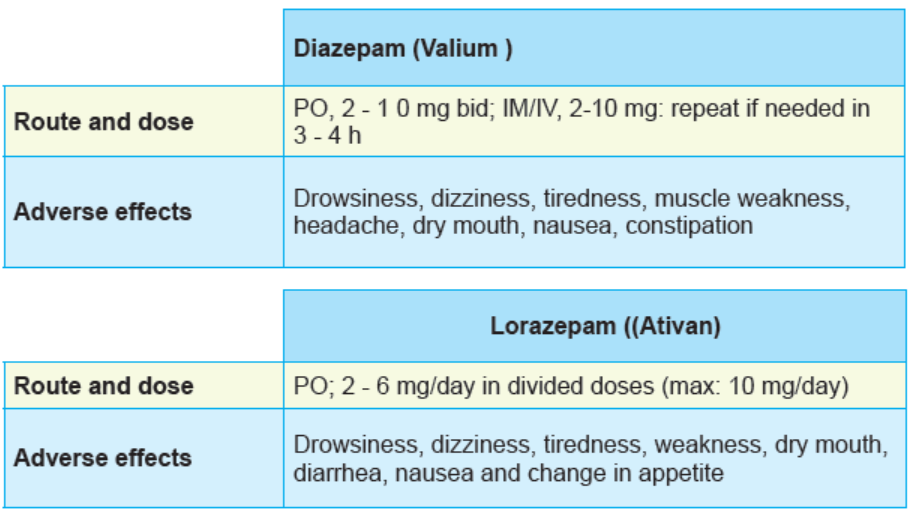

Figure 1.11.1: Benzodiazepine antiseizures
Hydantoins are a class of drugs mainly used to treat seizures (anticonvulsant or
antiepileptic drugs). They reduce seizures by targeting the sodium channel present
throughout the nerves. They act by desensitizing sodium channels in the CNS responsible
for neuronal responsiveness. This desensitization prevents the spread of disruptive electrical
charges in the brain that cause seizures.
Phenytoin is used for tonic-clonic seizures, psychomotor seizures, and seizures aft er head
trauma. Fosphenytoin is converted to phenytoin in the body and is parenterally used forcontrol of status epilepticus; it is a shortterm substitute for oral phenytoin.
Tables 1.11.3. Hydantoins Antiseizures:
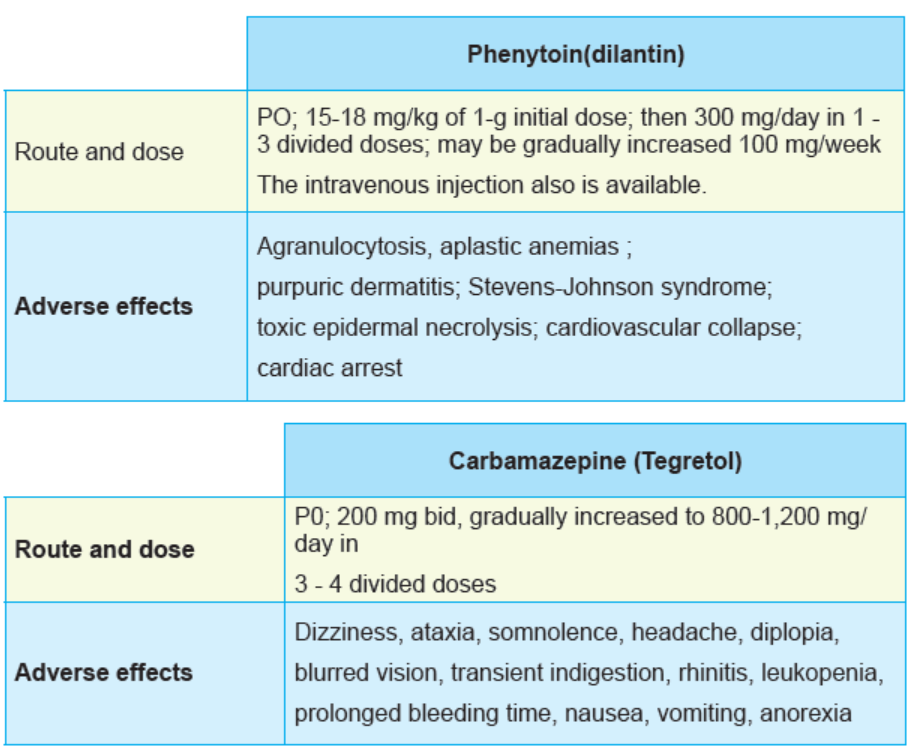
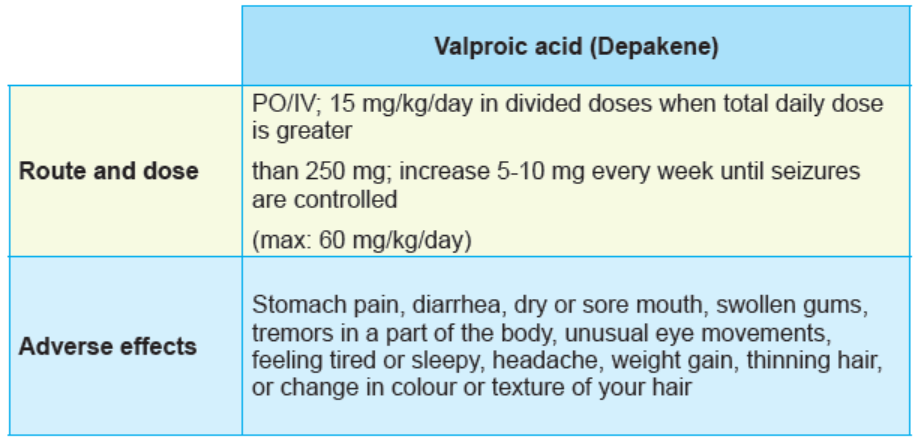


Figure 1.11.2: Form of hydantoins antiseizures
Succinimides antiseizures act by delaying the entry of calcium into neurons by
blocking calcium channels and inhibit neuronal systems. They increase the electrical
threshold. Succinimide drugs are used to control absence seizures and myoclonic seizures.They may be given in combination with other anticonvulsants.
Table 4. Succinimide antiseizures drugs:
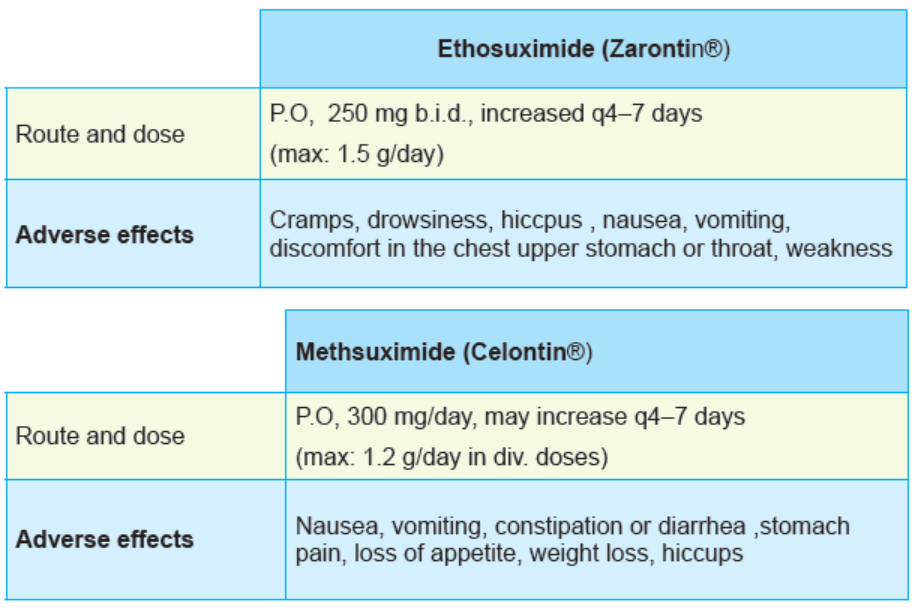

Forms of Succinimide antiseizures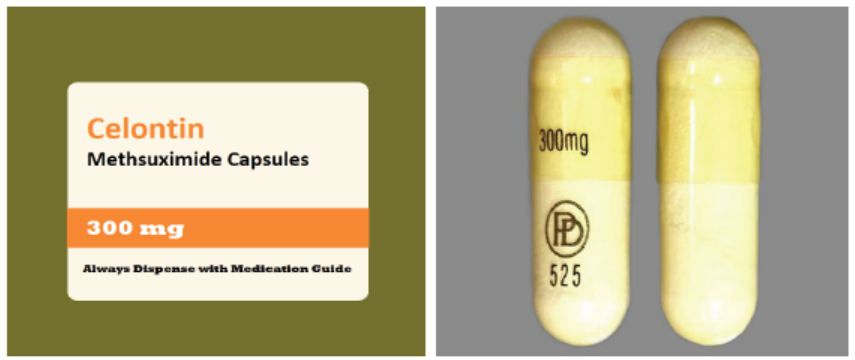
The common side effects of antiseizures drugs are: poor concentration, short
term memory loss, drowsiness, fatigue, hyperactivity, Visual problems (blurred or
double vision), speech problems, poor coordination and balance, dizziness and
unsteadiness, nausea, vomiting and weight gain or loss.
Self assessment 1.11
1. Which of the following is a barbiturate anti -seizure?
A. Diazepam
B. Carbamazepine
C. Phenobarbital
D. Valproic acid
2. Among class of antiseizures drugs act by potentiating GABA binding capacity
A. Barbiturates
B. Benzodiazepine
C. Succinimides
D. Hydantoins
3. Among class of antiseizures drugs act by delaying the entry of calcium into
neurons.
A. Barbiturates
B. Benzodiazepine
C. SuccinimidesD. Hydantoins
4. One of the following hydantoins antiseizures has a side effect of prolonging
the bleeding time. Select the best answer
A. Tegretol
B. Dilantin
C. DepakeneD. Valproic acid
1.12. End unit assessmentEnd of unit assessment1
1. Which of the following statements indicates the properties of paracetamol?
A. Paracetamol has strong anti-inflammatory effect compared to ibuprofen
or aspirin
B. Paracetamol is a commonly used antipyretic and may have an analgesic
effect
C. Paracetamol belongs to a wide class of non-steroidal anti-inflammatory
medications
D. Paracetamol may be classified in pregnancy category C drugs like
aspirin.
2. Nociceptive pain or physiological pain may be described as an abnormal
reaction to stimuli caused by damaged nerves. True or False.
3. Name three main classes of anti-inflammatory agents
Answer: nonsteroidal anti-inflammatory drugs (NSAIDs), salicylates, acetic acid
classes
4. Which of the following enzymes is blocked by ibuprofen to exert its anti
inflammatory action?
A. Cyclo-oxygenase
B. Monoamine oxidase
C. DeoxyribonucleaseD. Glucose isomerase
5. Which of the following anti-inflammatory drugs is classified among the
salicylates?
A. Diclofenac
B. Ibuprofen
C. Aspirin
D. Indocid
6. Which of the following antiseizure medications may be classified among the
barbiturates?
A. Lorazepam
B. Clonazepam
C. Carbamazepine
D. Phenobarbital
7. What are the three main classes of medications used in the management of
common cold?
A. Antihistamines, anti-inflammatories and anticonvulsant drugs .
B. Antihistamines, anti-inflammatories and decongestant drugs .
C. Antihistamines , anti-inflammatories and antiretroviral drugs .
D. Antihistamines , anti-inflammatories and antibiotic drugs .
8. What are the features of salicysm syndrome that results from the use of
higher doses of salicylates?
A. Dizziness, ringing in ears, difficult in breathing, nausea, vomiting, diarrhea
and mental confusion
B. Dizziness, ringing in ears, difficult in breathing, nausea, vomiting, high
fever and alertness
C. Alertnes, dizziness, ringing in ears, difficult in breathing, nausea,
vomiting, and tachycardia
D. Dizziness, ringing in ears, difficult in breathing, nausea, vomiting, skin
lesions and alertness
9. All of the following are the examples of local anaesthetics, EXCEPT:
A. Benzocaine,
B. Cloroprocaine
C. Tetracaine
D. Penicillin procaine
10. Antipyretic Causes decreased platelet aggregation and causes gastric ulcers
is
A. Diclofenac
B. Ibuprofen
C. Aspirin
D. Paracetamol
11. Which of these is not a purpose of inflammation?
A. Destroy the cause of inflammation
B. Isolate the cause of inflammation
C. Initiate tissue repair
D. Alert the organism of infection
12. Why most of medications for inflammation are treating at the same fever?
13. Case study: NG is a 26 years old man who presents to Remera health center
for consultation where you are working today as a nurse. The patient is
complaining of fever, headache, and chills for 2days. You took vital signs and
found that axillary temperature is 40. 90c; pulse was 70beats/min, respiration
22cycles per minutes, blood pressure 100/72 mmhg and has the pain of 6/10
on numeric scale, his weight is 65kg. Mr. NG declared that he has history of
gastritis, soon after he started shaking, finally got convulsion.
i. List all medications you will use to manage this case and give the
reasons. Indicate the specific and drug, dosageii. Which medications will you avoid to use? Why?