Topic outline
UNIT 1 LEARNERS WITH VISUAL IMPAIRMENT
Key Unit Competence: Trace characteristics of learners with visual
difficulties and teaching approaches.INTRODUCTORY ACTIVITY
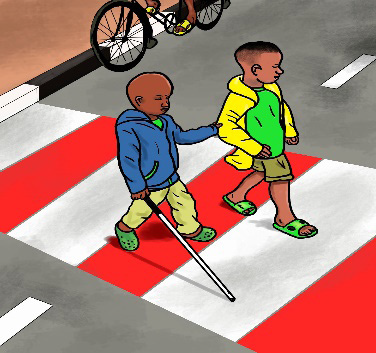
If you meet someone working in the street, wearing sun glasses, using white cane:
–What comes in your mind?
–What kind of disability do you think that person may have?–What are characteristics or traits that made you think the person has a disability?
1.1. Definition, causes and characteristics of Visual Impairment
ACTIVITY 1.1.
–What do you understand by the term” Visual Impairment”?
–What do you think can cause Visual Impairment?
–What could be indicators of someone having Visual Impairment?
1.1.1. Definition of Visual Impairment
The term “Visual difficulties or Visual Impairment” is used to describe any
kind of vision loss, whether total or partial. Visual Impairment is an umbrella
term that encompasses all types of vision losses). Visual difficulty can be:
• Any abnormality or problem in vision
• Any factor that can cause one to see less
• Inability of the eye or brain or both to visualize things in the normal
way.
1.1.2. The causes of Visual Impairment
• Parental problems: Poor nutrition of pregnant mothers, eating foods
that contain insufficient energy, proteins, vitamins and mineral salts;
alcohol use, smoking or strong drug-taking; cultural practices where
women are not allowed to eat some nutritious foods; premature births
resulting in babies being born with premature retina.
• Birth problems: Inappropriate use of tools to deliver the baby; difficult
during birth like anoxia (absence of oxygen in the brain) which can
cause brain damage.
• Malnutrition of the child from birth: Lack of a balanced diet, especially
insufficient vitamin A, which can cause night blindness or dry eyes.
• Injuries: Accidents which may affect different parts of the eye; brain
damage due to injuries/disease; e.g. cerebral palsy; chemicals/poison
in water, air and food, plus the use of traditional herbs; pregnant
mothers exposed to dangerous chemicals at work; poor hygiene related
to poverty and ignorance.
• Diseases/conditions: meningitis; cerebral malaria; glaucoma; cataract.
• Old age: As people grow old, they tend to become susceptible to some
diseases such as cataract, long-sightedness.
• Heredity: Genetic/parental diseases, diabetes, allergy.
1.1.3. The characteristics of Visual Impairment
Generally, learners with visual difficulties are characterized by different
behaviors including:
• Problems reading the notes from the chalkboard or scanning
information quickly
• Distortion of perception: i.e. what is being seen and perceived
• Problems in maintaining and changing focus at near and far distances
• Visual discomfort and fatigue.
However, it is very important and beneficial to identify a child with Visual
Impairment at early age for early intervention.
The following are characteristics of Visual Impairment during infancy and early
childhood:
During infancy:
• Lack of eye contact
• No blinking to bright light
• Do not look at his/her hands
• Do not visually follow moving objects in front of his/her face
• Slow response to voiceless toys or parents’ faces; respond only to sound
• No imitation of others’ expressions and actions
• Do not actively reach out for his/her favourite toys
• Fear of gross motor activities, such as crawling
During early childhood:
• Often keep his/her head down; lack eye contact with others
• Limited facial expression and body language
• Tend to hold objects very close to the eyes when looking at them
• Abnormal responses to bright light (gazing at light excessively or trying
to avoid it)
• Often bump into objects or fall over, and get confused with directions
• Search for his/her way using hands
• May press on eyeballs with fingers• Jerky movements of the eyeballs
SELF-ASSESSMENT 1.1
1. What is Visual Impairment?
2. Explain 3 causes of Visual Impairment3. Identify 5 characteristics of Visual Impairment
1.2. Classification and strategies of accommodating learners
with Visual Impairment in an inclusive class
ACTIVITY 1.2
1. How could we categorise Visual Impairment?
2. Which strategies do you think we should use to effectively
accommodate learners with visual disabilities in class?
1.2.1.Classification of Visual Impairment
Visual Impairment can be classified into three levels:
a. Mild Visual Impairment:
–– Can read relatively larger characters
–– No difficulty in identifying shapes, colours and brightness contrasts
b. Moderate Visual Impairment:
–– Can tell shapes and colours of objects and can distinguish between
brightness and darkness
–– Can only read characters with larger size and broader strokes
c. Severe Visual Impairment:
–– Can only distinguish more obvious changes in brightness and darkness
–– May not see anything (completely blind)
1.2.2. Strategies of accommodating learners with visual disabilities
in class
Many learners are visually impaired, but are fortunate enough to have the
impairment corrected by glasses and other optic aids. However, for some with
severe difficulties that cannot be corrected, such learners can only learn with
alternative and adapted assistance.
A learner with moderate visual difficulties can perform visual tasks almost like
a sighted learner, with the use of special aids and lighting. A learner with severe
visual difficulties may need extra time and energy to perform visual tasks,
even with visual aids. A learner with a profound Visual Impairment will find it
difficult to perform gross visual tasks, and detailed tasks virtually impossible.
Below are some examples of strategies to address their learning needs:
• Sitting arrangements: For learners with some vision, it is important
that they sit in a position in the classroom where they can see on the
board as clearly as possible. It may also be important for them not to sit
directly in very bright light (such as right next to a window), or in very
dark places (such as corners furthest from the window).
However, it is essential to ask the learner where they feel most
comfortable in the classroom, where they feel they can see the board
and their books most clearly, and thus where they feel they will learn
best. It is the teacher’s job to facilitate learner with VI to move and sit
in the ‘best’ location; but it is not necessarily always the teacher’s job
to decide, on their own, where that location should be.
• Organizing the classroom: When a learner with Visual Impairment
starts in a new classroom, the teacher and/or other children should
help to orient them to where the main facilities and obstacles are, and
where to find the learning materials they will need on a daily basis
(books, pens, etc). Teachers should ensure that they tell children about
any changes to the layout of the classroom (e.g. desks or cupboards that
have moved; or other new obstacles that have arrived). The teacher or
other learners should guide children with Visual Impairment to learn
these changes. Teachers and sighted learners should learn to avoid
leaving doors and drawers ajar (leave open) or leaving bags on the
floor in aisles between desks. They should take the habit of tucking
their chairs under their tables/desks when not being used, to minimize
the number of obstacles in the room.
The classroom instructions and regulations could be “Brailled”, that is,
Braille labels could be placed throughout the room, including in places
where there are written signs, and on the various pieces of furniture.
This will help children with Visual Impairment to navigate around
the room and find key objects or equipment needed during lessons. It
will help them practice reading Braille (if they are new to it), and give
sighted children a chance to start learning Braille.
• Effective communication
Communication techniques include the following:
–– Teachers should speak to the class when they enter and leave the room,
so that learners with Visual Impairment know what is happening.
–– Teachers should use auditory or tactile signals, and not just visual
signals. For instance, if the teacher normally puts a finger on his or her
lips to signal “please be quiet”, she could consider changing this signal
to involve first a hand clap.
If a teacher or sighted learners wants to attract the attention of a learner
with a Visual Impairment, they should say the learner’s name. If they
want to end a conversation or move away from a group that is talking,
they should tell the learner with Visual Impairment that they need to go,
not simply walk away.
–– The sighted learners in class should say their names before they start
speaking (e.g. when giving an answer to a question asked by the teacher)
so that children with Visual Impairment know who is speaking. This
may be particularly important at the start of new school year, when
children don’t know their classmates’ voices so well.
–– Teachers and sighted children in the school/class should learn how to
guide a child with a Visual Impairment. To be a guide they should first
identify themselves and offer to guide the child. If the child agrees, the
guide should offer their arm to the child’s hand. The guide needs to
tell the child with Visual Impairmentwhen there are steps up or down,
whether a door is to their left or right, and warn them of possible
hazards.
–– Teachers and sighted learners could learn how to use the concept of a
clock face to describe directions for children with Visual Impairment.
For instance, “it’s at 2 o’clock” would mean the direction the child needs
to move in is in front of them and slightly to the right. They should also
give clear directional instructions, such as “straight ahead”, “forward”
and “right”, and avoid saying, for instance “it is over there”. If there
are any notices on the walls (e.g. notifying children about changes to
the timetable, about a special event at the school, or about rewards
for achievement or behavior) the teacher should ensure that these are
read aloud when they are put on the wall.
• Pairing children: A sighted learner could volunteer to read out loud
to a learner with Visual Impairment. This could help both of them: the
learner with Visual Impairmentis able to access the reading materials,
and the sighted learner can revise the materials through reading it
again, which may be useful is he/she is experiencing some difficulties
with learning the content. When pairing learners, it’s important for
teachers to remember that learners with Visual Impairmentcan andshould help other learners, and not just be the recipients of help.
SELF-ASSESSMENT 1.2
1. Identify 3 categories of Visual Impairment
2. Explain 3 strategies of accommodating learners with VisualImpairment in class
SKILLS LAB
1. Visit one classroom in a nearby primary school, observe
all learners during lesson time, identify those with Visual
Impairment. Classify those learners into 3 categories of Visual
Impairment. Then advise the teacher on teaching approaches or
other reasonable accommodations he/ she should adopt in order
to meet the learning needs of learners with Visual Impairment inthe classroom.
END OF UNIT ASSESSMENT
1. Define Visual Impairment?
2. Give 3 causes of Visual Impairment?
3. Explain the three classification of Visual Impairment?
4. Give 3 characteristics of an infant with Visual Impairment?
5. How can you recognise that a child has Visual Impairment?
6. In the classroom, how can you identify a learner with Visual
Impairment?
7. In your own words, explain how you can accommodate a learnerwith Visual Impairment in the classroom?
UNIT 2 LEARNERS WITH HEARING IMPAIRMENT
Key Unit Competence: Apply suitable teaching methods, techniques and
strategies to address the needs of learners with
hearing difficultiesINTRODUCTORY ACTIVITY
Umutesi is a 7 years old girl who has just started Primary 1. She has a
hearing loss resulting from repeated and severe ear infections throughout
her early childhood. Her hearing loss is considered hard-of-hearing because
she has some residual hearing and uses hearing aids. Umutesi’s language
and speech skills are delayed because she could not hear adequately since
early childhood. Umutesi is being assisted by an audiologist who ensures
that her devices are in good working conditions, and she uses the devices in
her schooling.
1. What was the cause of hearing loss in Umutesi’s case?
2. Discuss challenges or barriers Umutesi may face in school?
3. What teachers can do to remove barriers Umutesi might face in her
learning process.
2.1. Definition, cause, and characteristics of Hearing Impairment
ACTIVITY 2.1.
–– How would you define Hearing Impairment?
–– What could be the causes of Hearing Impairment?
–– What could be the symptoms of a learner with Hearing
Impairment?
2.1.1. Definition of hearing difficulties
Hearing Impairment signifies full or partial loss of the ability to detect or
discriminate sounds due to an abnormality associated with the physiology,
anatomy, or function of the ear. Hearing Impairment is an inability to hear well
or not hearing at all.
According to WHO census, (20 March 2019) Around 466 million people
worldwide have hearing loss and 34 million of these are children. It is estimated
that by 2050 over 900 million people will have disabling hearing loss.
2.1.2. Causes of Hearing Impairment and deafness
The main causes of Hearing Impairment include:
• Hereditary factors: This is hearing loss or deafness that is inherited
from parents or relatives
• Prenatal factors:An expectant mother can be exposed to many different
kinds of infection during pregnancy, such as rubella and influenza. Some
of these infections are more damaging to the developing embryo than
others. One of the most serious infections is rubella. Other infections
contracted by the mother such as syphilis, may also cause Hearing
Impairment in the developing embryo. Certain drugs such as quinine
taken during pregnancy may also cause Hearing Impairment in a child.
• Peri-natal factors: Hearing Impairment may occur just before, during
or just after birth due to the lack of oxygen (anoxia).
• Post-natal factors: Infectious diseases such as meningitis, measles and
mumps can lead to Hearing Impairment, this can be during childhood
or later in life. Discharge from ears is mainly as a result of chronic
ear infections which may lead to hearing loss. In certain cases, this
condition can also lead to serious and life-threatening complications,
such as brain abscess and meningitis. Use of some drugs such as antimalaria
drugs and certain antibiotic can damage the inner ear. Injuries
to the skull are particularly serious as they may rupture the ear drum,
dislocate the ossicles or affect the inner ear. Other causes that may lead
to Hearing Impairment are exposure to excessive noise, old age and
presences of foreign bodies in the external auditory canal.
2.1.3. Characteristics of learners with Hearing Impairment
Learners with Hearing Impairment generally show some specific behavioural
characteristics:
• Have difficult in hearing high pithed speech sounds such as: /s/, /f/,
/z/, /t/, /k/, /t f/
• Have difficult in understanding directions
• Rely more on visual information processing
• Have difficult in group discussions
• Do not develop speech spontaneously
• May not participate in useful conversation with others
• Have inappropriate rhythm in speech and have poor articulation
• Have a feeling of inferiority and may withdraw from the hearing
community if misunderstand
• May become aggressive or impulsive if not given appropriate support
by the hearing
• Ask repetition of what has been said
• Cups the ear in the direction of sounds
SELF-ASSESSMENT 2.1
1. What is Hearing Impairment?
2. Give 5 characteristics of a learners with Hearing Impairment
3. Explain the causes of Hearing Impairment and deafness (in yourown words)
2.2. Classification and strategies to teach learners with
Hearing Impairment
ACTIVITY 2.2.
– What is the classification of Hearing Impairment?
– Explain the strategies of teaching learners with Hearing
Impairment
2.2.1. Classification of Hearing Impairment
Hearing loss can be classified according to:
• Severity
• Age of onset
• Part of the ear affected
a. Classification according to severity:
Some learners may only have slight or severe hearing loss. There are five major
categories of hearing loss:
1. Learners with slight hearing loss: These are learners who can follow
normal conversation if there is no noise in the room but would need a
preferential seating arrangement while facing the speaker. They may
also have difficulty hearing faint or distant speech.
2. Learners with mild hearing loss: Learners in this category may
understand a conversation only at a distance of about one meter
when the room is very quiet. They may miss as much as 50% of class
discussion if voices are faint and may exhibit limited vocabulary and
speech anomaly. In some cases, a child with mild hearing loss may not
be able to make certain speech sounds that are high pitched such as /s/
and /f/. Usually his/her main problem is that he/she mal-articulates or
omits some sounds.
3. Learners with moderate hearing loss: These learners may have
difficulties hearing in all situations and:
• Can only follow loud conversation;
• Are deficient in language use and comprehension;
• Are likely to have defective speech
• Have limited vocabulary
• Need the use of hearing aid and in some cases, speech training
4. Learners with severe hearing loss: These learners may hear loud
voices about 30 cm from ear. They may be able to identify environmental
sounds and discriminate vowels but not all consonants.
5. Learners with profound hearing loss: These learners may hear some
loud sounds but are aware of vibrations more than tonal pattern .They rely
on vision rather that hearing as the primary avenue of communication.
They need hearing aids and sign language.
b. Classification according to age of onset
According to age of onset, Hearing Impairment is categorized into two: These
are:
Pre-lingual deafness: This refers to Hearing Impairment occurring prior to
the age of two or before speech development.
Post-lingual deafness: This refers to Hearing Impairment occurring at any age
after speech has fully developed.
c. Classification according to the part of the ear affected
Before discussing this, we need to look at the anatomy of the ear. Functionally
the ear is divide into three main parts. These are the outer ear, the middle andthe inner ear as shown in figure below.
There are four types of hearing loss according to the part of the ear affected.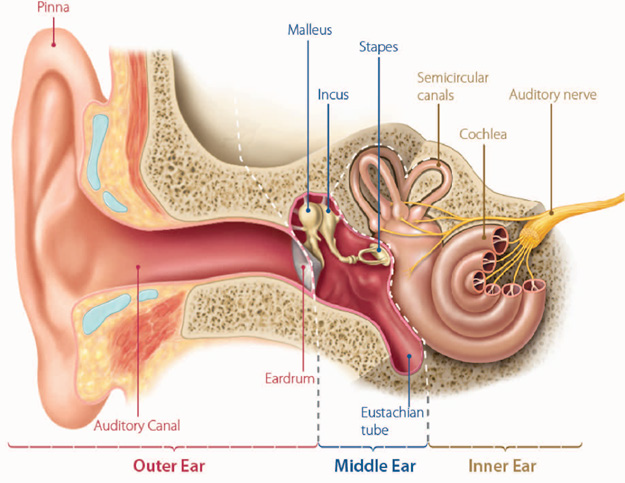
These are:
• Conductive
• Sensory-neural
• Mixed
• Auditory Neuropathy Spectrum Disorder
Conductive hearing loss: This is when the damage or infection is either in
the outer or the middle parts of the ear. This may result in mild or moderate
hearing loss. Those with this type of hearing loss have residual hearing
left and can hear and understand spoken language with the help of suitable
hearing aids.
Sensori-neural hearing loss: This is when the damage is in the inner ear.
This may result in severe or profound hearing loss little residual hearing
left. Children with this type of hearing loss usually do not acquire and use
spoken language.
Mixed hearing loss: This refers to a combination of both conductive and
sensori-neural hearing loss this means that both the outer middle ear and
the inner ear are affected at the same time. It should be noted that learners
with Hearing Impairment can either be hard of hearing or deaf. Hard of
hearing persons are able to use their hearing ability either with or without
use of hearing aids. Speech and language skills are normally developed
through the auditory channel. Deaf persons have a hearing loss that does
not enable them to use hearing ability to understand speech even with the
use of hearing aid. Such a learner uses vision as the primary modality for
learning and communication.
Auditory Neuropathy Spectrum Disorder: Hearing loss that occurs when
sound enters the ear normally, but because of damage to the inner ear or the
hearing nerve, sound isn’t organized in a way that the brain can understand.
2.2.2. Strategies to teach learners with Hearing Impairment
– Organize the classroom so that all the children are sitting in a U shape.
This way the children can see each other, which will make it easier for
children with Hearing Impairment to use sign language, read lips and
understand mimics, thereby making it possible to participate more
actively in discussions and classroom activities.
– Spend some time giving face-to-face instruction, since group situations
can be quite challenging for children with Hearing Impairment.
– Look at the child (with Hearing Impairment) while speaking to her/
him.
– Speak slowly and clearly, but not too loud.
– Use short, simple, and clear sentences.
– Be consistent in the use of language.
– Use clear mimics and gestures.
– Ask the child (if s/he has an oral language) to repeat what s/he has
understood.
– Write down key words from the information given during the class and
give it to the child at the end of every day.
– Work together with an audiologist (if available) to teach and
encourage the child to use her/his residual hearing to the maximum
extent possible, even if the preferred means of communication is sign
language.
– Reduce all unnecessary noise, as multiple sources of sound will make it
more difficult for the child to use her/his residual hearing. This is also
important if the child is using a hearing aid.
– If some of the classrooms in the school are noisier than others (e.g.
noise from busy roads, airports or factories), the school should be
flexible and move any classes with children with Hearing Impairment
(as well as classes with children with Visual Impairment or other
disabilities) to less noisy rooms.
– Be flexible with time, as most of the children with Hearing Impairment
(both deaf and hard of hearing) will struggle to understand everything
that goes on in the classroom (as a result of their hearing loss).
– Focus more on content than on grammar when assessing the writing of
children who primarily use sign language for communication. Because
the grammar of sign languages is very different from written languages
– Please take into consideration that:
– Facial hair (e.g. beards and moustaches) worn by male teachers may
obscure leap reading and facial expressions.
– Face covering – veils covering eyes, eyebrows, nose, mouth and cheeks
(worn by some teachers and fellow learners), may obscure leap reading
and facial expressions.
The majority of children who are deaf (profound hearing loss) are born to hearing
parents. The school should therefore attempt to provide instruction for parents on
the implications of deafness within the family.
A learner who is hard of hearing may also need more time to learn than other learners,
as s/he will not always be able to hear the teacher’s voice and what other children
talk about in the classroom. Therefore, much of the information given duringthe lessons will be lost.
SELF-ASSESSMENT 2.2
1. What is Hearing Impairment
2. Hearing Impairment can be classified according to 3 elements.
What are these elements?
3. What are the four types of hearing loss according to the part of
the ear affected?
4. What are the five major categories of hearing loss
5. Give 5 strategies to teach learners with Hearing Impairment
SKILLS LAB
Visit one classroom in a nearby primary school, observe all learners
during lesson and break time. Identify those who might have Hearing
Impairment. Based on 5 major categories of Hearing Impairment, assess
these learners and classify them into 5 categories. Advise the teacher on
teaching approaches or other reasonable accommodations to adopt in
order to meet the learning needs of learners with Hearing Impairment
in the classroom.
END OF UNIT ASSESSMENT
1. What is Hearing Impairment?
2. Give 5 characteristics of a learners with Hearing Impairment
3. Classify hearing loss according to severity, age of onset, and part
of the ear affected4. What are the five major categories of Hearing Impairment?
UNIT 3 LEARNERS WITH DEAF-BLINDNESS
Key Unit Competence: Explain the characteristics of leaners whith deafblind
disability and use appropriate approaches
to teach them.
INTRODUCTORY ACTIVITY
The case of Kawera
Kawera is 8 years old girl who is studying in primary 2. Since she was born, she
had hearing difficulties and total blindness. It is suspected that her problem
is from her grandfather who had the same difficulties like Kawera but also
her mother is a well-known alcohol abuser. She faces many difficulties in her
life. She cannot communicate, move around easily and these affect the way
she interact with the community.Kawera has recently been able to join the
school. However, due to her condition the school recruited the new teacher
who will assist Kawera in her school activities. The school has also engaged
health practitioners who come once in a while to check on Kawera’s life. They
work to prevent the severity of her impairment and provide the intervention
needed. Kawera is now progressing well in her education.
Tasks:
1. What was the cause of deaf-blind in Kawera’s case?
2. What are challenges Kawera face in school?
3. What did school do to remove some barriers for Kawera?
3.1. Definition and causes of deaf blind disability
ACTIVITY 3.1.
1. How would you define the term” deaf-blindness “?2. What do you think could cause deaf blindness ?
Deaf-blindness is a combination of sight and Hearing Impairment that affects
how you communicate, access information and get around.The deafblind doesnot necessarily mean to be totally deaf or totally blind.

Learner with deaf blind disability being thought using tactile method
Most of children who are deaf-blind also have additional
physical, medical and/or cognitive problems. People are
considered to be deaf-blind when the combination of their
hearing and vision loss causes such severe communication,
other developmental and educational needs that they
require significant and unique adaptations in their educational
programs.
Causes of deaf blind disability
There are four primary causes of vision and hearing loss:
Genetic factors: (Hereditary/Chromosomal Disorders): are inherited
from parents, for example, Usher syndrome (is a condition characterized
by partial or total hearing loss and vision that worsen overt time) is
caused by eye disease called retinitis pigmentosa, this syndrome is
present from birth with effects appearing gradually over the years.
Prenatal factors: Those are some complications before birth. It
also includes chronic maternal illnesses, viral/bacterial diseases, or
harmful chemicals (Teratogens).
Complications at birth: There are many congenital complications that
may be one of causes of disability.
Postnatal injuries and/or illnesses: Those are some factors of
after birth that may contribute to become a deafblind including age
related illnesses for hearing and vision, diabetic retinopathy which
is complications of diabetes where the cells lining the back of eye aredamaged, brain damage due to the wide range of conditions.
SELF-ASSESSMENT 3.1
1. Briefly, discuss the meaning of deafblind?
2. What are the four factors of deafblind disability?
3. Explain the following factors:
• Postnatal factors;
• Genetic factor
3.2. Characteristics and Types of deafblind disability
ACTIVITY 3.2.
1. If deafblindness affect persons of different age, how can you
describe a deafblindness?
2. If you have seen a person with deafblindness in your environment,
what are challenges do you think they face in daily life activity?
Deaf blindness can affect people of all ages (children, adults and elders). For
adults, it develops gradually and the person themselves may not realise their
vision and/or hearing is getting worse.
Characteristics of deafblind disability may include:
• Needing to turn up the volume on the television or radio
• Difficulty following a conversation
• Not hearing noises such as a knock at the door
• Asking others to speak loudly, slowly and more clearly
• Needing to hold books or newspapers very close, or sitting close to the
television• Difficulty moving around unfamiliar places.
Types of deafblind disability
People with deaf-blindness may fall into three groups:
• People with residual sight but who are completely deaf
• People with residual hearing who are completely blind
• People without residual sight or hearing.
Residual sight or hearing is often not sufficient for a person to be totally
dependent on it. Deaf-blind learners without any residual sight or hearing need
more support than those with residual sight or hearing.
It is not easy for a sighted and hearing person to understand what it is like to
be deaf-blind.
Key difficulties experienced by deaf-blind people include:
Finding out information: Deafblind have challenges of finding
out information that help them participate in the daily life of their
community, such as the meaning behind facial expressions or the shape
of objects that cannot be reached, or the sound of an approaching
vehicle.
Communicating with others: Deaf-blind people are unlikely to meet
many people who can communicate with them straight away. They use
one or more ways of communications including sign language etc.
Movement: Deafblind people can neither see nor hear. Therefore
most of the time they do not want to move around avoiding obstacles,
planning routes or climbing stairs.
SELF-ASSESSMENT 3.2
1. What are three types of deafblind people.
2. How does deafblind disability develop in adult people?3. What characterize a deafblind person?
3.3. Teaching approaches for learners with deafblind disability
ACTIVITY 3.3.
1. How do you think we should help persons with deaf blindness?
Most deafblind people still have some hearing and/or vision at different level
of disabilities. The level of care and support they need will depend on severity
of their hearing and vision problems. Learners, who are deafblind since their
birth, will need the early childhood interventions. Early intervention should
be to stimulate the awareness of their immediate environment and to create
interest in the external world. They need to be deliberately encouraged and
introduced into the world through one-on-one communicative interaction. Sign
language is the most obvious choice of communicative skills that can aid the
communication and can be very effective in developmentally capable individuals
with dual sensory impairment. However, learners who are deafblind can only
be included in regular classrooms if their cases are either mild or moderate,
the severe deafblind are placed in special places and supported with the help ofmulti-disciplinary team.
Teaching approaches for deafblind learners

Here are some strategies that maybe used when teaching deafblind learners
1. Making contact: Cued communication can be used to provide meaningful
information through a combination of approaches, tangible object cues,
touch cues and tactile signs/gestures.
2. Build relationship/ provide feedback: The partner should be
consistent in the way they approach the learner while making a physical
contact.
3. Interrupted routines: It is one strategy where communication partner
interrupts the learners’ established routines to see/observe how she /he
responds. The partner may use this interruption to initiate a conversation
or to teach a sign related to the interrupted activity.
4. Choice making: This is to help the learner to use cognitive skills,
communication, motor skills and social skills. This help him/her to avoid
imposed decisions to them for others people.
5. Establishing routines: Use a simple and communication techniques
especially in teaching daily living activities to establish a predictable
routine from which further communication is developed.
6. Acknowledging communications efforts: The learner’s effort to
initiate a conversation must be encouraged.
7. Using tactile cues: Refers to three dimensions’ tangibles objects that
can be manipulated easily and possess tangible qualities such as shape,
textile, consistency. These are real objects, miniatures objects, or partialobject that are fixed on the cards.
The individual abilities and needs of deaf blind children must be assessed
in order to make an individual plan.
The individual plan also should focus on to: preserve and maximise
any remaining sensory functions the person has, teach alternative
communication methods such as tangible object cues, touch cues and
tactile signs/gestures, help the person retain as much independence as possible,
for example training to use a long cane or guide dog or through the provision of
a communicator guide, for young children, ensure their educational needs are
met.
There are different ways of communication for deafblind such as:
Clear speech: Speaking clearly is one of the most effective and common
ways of communicating with deafblind people who have some remaining
vision and hearing
Deafblind manual alphabet: A tactile form of communication where words
are spelt into the deafblind person’s hand using set positions and movements.
Block alphabet: A simple tactile form of communication where a word is
spelt out in capital letters that are drawn into the deafblind person’s palm
Hands-on signing: An adapted version of British Sign Language
(BSL) where the deafblind person feels what’s being signed by placing their
hands-on top of the signer’s hand
Visual frame signing: An adapted version of BSL where the signs are
adapted to be signed in a smaller space to match the position and size of a
deafblind person’s remaining sight
Braille: A system that uses a series of raised dots to represent letters or
groups of letters.
Moon: Similar to Braille, but uses raised, adapted capital letters that are
simpler to feel.SELF-ASSESSMENT 3.3
1. Explain how you can communicate with a learner with deaf
blindness using the following methods?
a. Braille b. Block alphabet2. What is the difficult of deafblind in every day ?
SKILLS LAB
1. Visit a special school and identify a child suspected to have
deafblind disability. Spend around three hours with the child.
Write down all the characteristics of the child with deafblind
disability and suggest strategies you could use to help that child
improve his/her studies.
END OF UNIT ASSESSMENT
1. Explain the deafbliness ?
2. Explain the different types of deafblindness
3. Discuss the difficulties of deafblind people in everyday life.4. Identify ways of communication with deafblind learners
UNIT4 LEARNERS WITH PHYSICAL DISABILITIES AND OTHER HEALTH IMPAIREMENTS
Key Unit Competence: Apply suitable teaching methods, techniques
and strategies to address the needs of learners
with Physical Disabilities and Other Health
Impairments
INTRODUCTORY ACTIVITY
Shumbusho is an amazing young boy who has exceeded most of the expectations
of those who made assumptions based on his “labels” and therefore had lowered
expectation for him. Fortunately, he did no live down to their expectations.
Shumbusho has Duchenne Muscular Dystrophy, a form of Muscular Dystrophy
which is genetically inherited disorders characterized by progressive muscle
weakness and degeneration of skeletal muscles which control movement. At age
two, Shumbusho was still unable to walk. At age six, Shumbusho had difficulty
rising from a sitting or lying position. At primary school, he could not run the same
distance as his peers, he would fall frequently and had unusual fatigue. By age 12,
Shumbusho was using a wheelchair because his muscles in the shoulders, arms, back
and legs were very weak. Shumbusho was a very bright learner despite his physical
conditions. He has been blessed by many wonderful headteachers, teachers, aids
and therapists who gave so much of themselves for his benefits. I hope that they
will someday realize the impact that each one of them has had, individually and
collectively on Shumbusho and through him on the community as a whole. Because
of muscles weakness, Shumbusho had to be given an extra time to complete his
assignments and homework. The school infrastructures were designed to facilitate
Shumbusho’s movement. The school sometimes invite a physiotherapy who
worked to help Shumbusho with his muscles strengths. Shumbusho had to be given
adapted activities in Physical Education and Sport and in mathematics. Teachers
were always happy to provide remedial teaching any time Shumbusho would miss
the class. Due to the support he received Shumbusho passed the national exams
successfully and was admitted to the best secondary school in Rwanda. Shumbusho
is an inspiration, and a wonderful example of what can be a child with disabilities if
provided with appropriate support and services.
1. Discuss what characterized Shumbusho as a young boy who wanted to
excel academically?
2. Many people came in to help Shumbusho reach his potentials, whowere these people?
4.1. Definition of Physical Disabilities and other Health
Impairments
ACTIVITY 4.1
1. You have probably met persons with Physical Disabilities. What
do you understand by Physical Disabilities?
2. You certainly know people who have chronic Health Impairments.How would you explain the term” Health Impairment”?
4.1.1. Definition of Physical Disability
A Physical Disability is the long-term loss or impairment of part of the body’s
physical function. It can involve difficulties with walking and mobility, sitting
and standing, use of your hands and arms, sight, hearing, speech, breathing,
bladder control, muscle control, sleeping, fits and seizures or chronic tiredness.
4.1.2. Definition of Health Impairments
Health Impairment means having limited strength, vitality or alertness including
a heightened alertness to environmental stimulus, that results in limited
alertness with respect to the education environment that is due to chronic or
acute health problems such as asthma, Epilepsy etc, and that adversely affects
a child’s educational performance.
SELF-ASSESSMENT 4.1
1. Physical Disabilitycan involve difficulties with many aspects of
life. What do you think are areas that are affected by the Physical
Disability?2. What Health Impairment means to you?
4.2. Categories of Physical Disability and Health Impairment
ACTIVITY 4.2
1. Discuss different physical and health problems you may have
noticed among persons in your community?
Physical Disability and Health Impairment can be categories into three broad
categories:
1. Musculo skeletal or Orthopaedic impairment
2. Neuro Musculo Disability
3. Chronic Health Impairment
1. Musculo skeletal impairment or orthopaedic impairment
It is defined as the inability to carry out distinctive activities associated with
movements of the body parts due to muscular or bony deformities, diseases or
degeneration. The disabilities grouped under musculo skeletal disability are:
• Loss or Deformity of Limbs or amputation
• Osteogensis Imperfecta or brittle bones
• Muscular Dystrophy
2. Neuro Musculo Disability
It is defined as the inability to perform controlled movements of affected body
parts due to diseases, degeneration or disorder of the nervous system. The
categories are:
• Cerebral Palsy
• Spina Bifida
• Poliomyelitis
• Multiple Sclerosis
• Poliomyelitis
3. Chronic Health Impairment
Chronic Health Impairments limit strength, vitality or alertness and may
adversely affect the learner’ educational development. Learners with chronic
Health Impairment are extremely limited in their activities and require
intensive medical and educational help. The side effects of medications can
have a significant impact on memory, attention, strength, endurance and energy
levels.
Some of the chronic health problems include:
• Asthma
• Cancer
• HIV and AIDS
• Heart condition
• Rheumatic fever
• Tuberculosis• Leukemia
SELF-ASSESSMENT 4.2
1. What is the difference between Musculo skeletal impairment and
Neuro Musculo Disability? Give three example of each category
2. What do you understand by Chronic Health Impairment? give
three example of Health problem.
3. What Health Impairment means to you?
4.3. Causes of Physical Disability and other Health Impairment
ACTIVITY 4.3
1. Discuss different physical and health problems you may have
noticed among persons in your community?
The etiology or cause of physical and health disabilities varies greatly
according to specific diseases or disorder. Some of the most common etiologies
resulting in physical and health disabilities are genetic and chromosomal
defects, teratogenic causes, prematurity and complications of pregnancy and
acquired causes. On the other hand, the exact cause of some physical and health
disabilities are unknown.
4.3.1. Chromosomal and Genetic causes
Among the most common causes of physical and health disabilities are hereditary
conditions resulting from defects in one or both parent’s chromosomes or
genes. Several genetic defects are believed to contribute to a range of physical
and health disabilities such as muscular dystrophy.
4.3.2. Teratogenic causes
Many physical and health disabilities are caused by teratogenic agents that affect
the developing fetus. Teratogens are outside causes, such as infections, drugs,
chemicals or environmental agents, that can produce fetal abnormalities. The
fetus is also at risk of developing physical and health disabilities when exposed
to certain drugs, chemicals or environmental agents. Maternal abuse of alcohol,
for example, has been linked to a range of physical, cognitive, and behavioral
abnormalities that can result in lifelong damage. Serious fetal abnormalities
can also occur as a result of prescription medications taken for maternal illnessor disease (for example, certain antibiotics and seizure medications).
4.3.3. Prematurity and complications of pregnancy
Infants are usually born at approximately 40 weeks of gestation. An infant
born before 37 weeks is considered premature. Infants who are premature
and born with very low birth weights (less than 1.5 Kg) are at risk of having
disabilities. The infant can develop neurological problems resulting in cerebral
palsy, epilepsy etc.
In some instances, babies that are born on time and with average weight
encounter complications during the perinatal period. The most common
cause of brain injury during the perinatal period is asphyxia – A decrease of
oxygen in the blood. Among infants who survive an episode of asphyxia, several
disabilities may occur such as cerebral palsy, epilepsy etc.
4.3.4. Acquired causes
Many physical and health disabilities are acquired after birth by infants,
children and adults. These acquired causes include trauma, environment toxins
and disease. For examples falls, accident are causes of amputation and othertraumatic brain injury.
SELF-ASSESSMENT 4.3
1. With clear examples, explain how teratogenic agents can cause
physical and health disability?
2. What is asphyxia and how it is a leading cause of Physical
Disability?
4.4. Characteristics of Physical Disability and other Health
Impairment
ACTIVITY 4.4
1. What are indicators of a person with amputation and
poliomyelitis?
The specific characteristics of an individual who has a physical or health
disability will depend on the specific disease, its severity, and individual factors.
Two individuals with identical diagnoses may be quite different in terms of
their capabilities. Also, it is important to remember that students who have
severe physical disabilities (even individuals who are unable to walk, talk or
feed themselves) may have normal or gifted intelligence. No one should judge a
person’s intellectual ability based on physical appearance.
Let us discuss however on characteristics of the most commonly found Physical
Disability in the school age population.
4.4.1 Learners with amputation
An amputation is the removal of a
body extremity, most often referring
to the loss of an arm, leg, fingers, or
toe. The removal is often done through
surgery in response to a trauma,
disease or infection. In addition
to removing diseased tissues, the
amputation of limb may also relieve
pain. A congenital amputation occurs
at birth and is the term used whensomeone is born without a limb.

Students with amputation
4.4.2 Learners with Muscular Dystrophy
Muscular Dystrophy is a genetic(inherited) condition that gradually causes the
muscles to weaken. It often affects a particular group of muscles, before moving
on to the other muscles. If muscular dystrophy begins to affect the heart or the
muscles used for breathing, it becomes life- threatening.
A child with muscular Dystrophy may display the following observable
characteristics:
• Tendency to tire quickly
• Postural changes due
to progressive muscle
weakness
• Waddling gait with legs far
apart
• Walking on tip toes
• Tendency to lose finemanual dexterity

Equinovarus deformity
• Trouble walking and maintaining balance
• Poor posture with a protruding abdomen and a sway back
• Equinovarus deformity of the feet
• Increasing difficulty in rising from the floor• Lack of motivation because of limitation
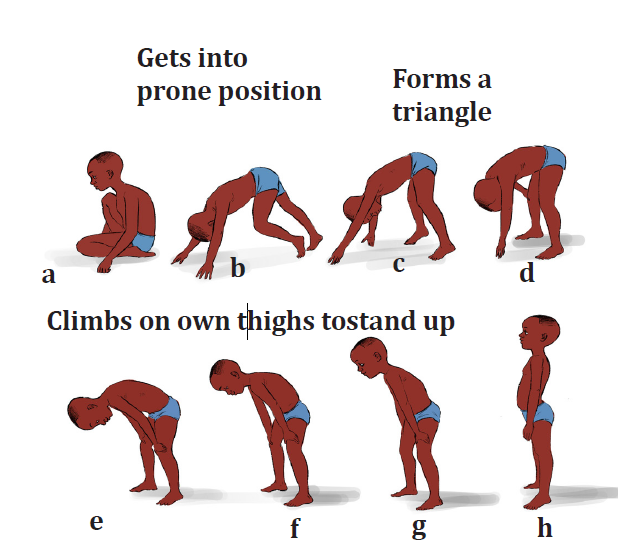
Difficulty in rising from the floor
Posture change
4.4.3. Learners with Cerebral Palsy
Cerebral means” concerning the brain” and palsy means “paralyses or the
inability to move. Therefore, cerebral palsy is a disorder of the brain that occurs
as a result of brain damage or lack of development in the part of the brain
controlling movement and posture.
The following are key signs that you may notice in children with Cerebral Palsy:
• Abnormal perception and
sensation
• Delayed or lack of speech
control
• Different walking patterns
• Difficulty with gross and fine
motor skills
• Involuntary movement and
lack of coordination
Learners with Cerebral Palsy
• Lack of muscle control, muscle tightness or spasm
• Poor posture and spastic movements
4.4.4. Learners with Epilepsy
Epilepsy is currently defined as a tendency to have recurrent seizures (sometimes
called fits). A seizure is caused by a sudden burst of excess electrical activity
in the brain, caving a temporary disruption in the normal message passing
between brain cells. The disruption results in the brain’s message becoming
halted or mixed up.
Learners who are epileptic display the following behaviours during a seizure
attach:
• Confusion and difficulty walking
• Loss of consciousness
• Convulsion
• Drooling• Eyelid fluttering and rolling up
• Falling down, staring and stiffening
After the convulsions, you may observe the
following:
• Difficulty talking
• Sleeping
• Exhaustion
• Thirst
• Weakness• Urge to urinate/ defecate

A girl after convulsions
4.4.5. Learners with Spina Bifida
Spina bifida is a birth defect that involves the incomplete development of the
spinal cord or its coverings. The term Spina bifida comes from Latin and literally
means split or open spine. Spina bifida occurs at the end of the first month
of pregnancy when the two sides of the embryo’s spine fail to join together,
leaving an open area. In some cases, the spinal cord or other membranes may
push through this opening in the back. The condition is usually detected before
a baby is born and treated right away. The symptoms of spina bifida vary from
person to person, depending on the type and level of involvement. However,
learners with Spina Bifida may have the following characteristics:
• Closed neural tube
defects
• Have problems with
bowel and bladder
control
• Fluid-filled sac visible
on the back protruding
from the spinal canal
• Spinal cord tissue is
usually exposed• Muscle weakness
Fluid -filled sac on the bac
• Paralysis
• Incontinence
• Poor short term memory
• Easily distracted
• Poor attention
4.4.6. Learners with Poliomyelitis
Poliomyelitis (Polio) is a highly infections viral disease, which mainly affects
young children. The virus is transmitted through contaminated food and water,
and multiplies in the intestine from where it can invade the nervous system.
Many infected people have no symptoms, but do excrete the virus in their
faeces, hence transmitting infection to others.Characteristics of polio include:
• Degeneration of
muscles and bones
• Permanent paralysis
• Stunted growth of theaffected limb
Learners with polio
4.4.7. Learners with Asthma
Asthma is the most common pulmonary disease of chilhood and is on the
increase. Children who have asthma breathe normally until they come in
contact with a substace or situation that triggers an asthma attach such as
pollen, air pollution, a respiratory infection or exercise. When an asthma attach
is triggered , the learner has the following chracateristics:
• Wheezing
• Frequent coughing
• Shortness of breath
• Labored breathing
• Chest tightness, apin or presuure
• Feeling very tired or weak after exercising
• Trouble sleeping
4.4.8. Learners with infectious diseases
Several infectious diseases fall under the heading of other health impairements.
Some infectious diseases are readily transmittable( such as tuberculosis),
others may pose no threat in the school environment( such as AIDS).
Learners with HIV and AIDS: A great number of children around the world
are infected by the HIV every year. UNICEF, (2005) reported that at the end of
2017, about 2.6 million children lived with HIV in the world. AIDS stands for
Acquired Immunodeficiency Syndrome. It is a desease that prevent the body
from fighting infections. The Human Immunodeficiency Virus, which is known
as HIV, infects and damages parts of the body’s defenses againest infections.
HIV can be transmitted through direct contact with blood or other body fluids.
Children commonly contract HIV during fetal development in the mother’s
uterus, at the time of birth, or during breastfeeding. Not all infant born to HIV
positive mothers will have the HIV infection. However, the most common way
children contract HIV is through mother- to baby transmission.Not all children
with HIV will have symptoms, and those that do won’t have exactly the same
ones. Symptoms can vary by age. Some of the more common are:
• Being sick often with childhood illnesses such as an ear infection, a
cold, an upset stomach, or diarrhea
• Failure to reach the developmental milestones as the normal children
SELF-ASSESSMENT 4.4
1. You are asked to assist the group assessing children with
disabilities. What would be the signs that would point to the fact
that a child has:
a. Muscular Dystrophy
b. Cerebral Palsyc. Poliomyelitis
4.5. Teaching and learning approaches for learners with
Phyical Disabilities and other Health Impairements
ACTIVITY 4.5
1. How can you help a child with Cerebral Palsy?
2. Environmental aspect is very important for learners with
Physical Disabilities, how would ensure that environment is
conducive for learners with PD to learn effectively?
There are many teaching strategies you can use to ensure effective and
productive learning environments and experiences for all students, including
those with disabilities. Accessible Education is the process of designing courses
and developing a teaching style to meet the needs of people who have a variety
of backgrounds, abilities and learning styles. Just as there is no single way to
teach, people learn in a variety of ways; using different instructional methods
will help meet the needs of the greatest number of learners.
Meeting the educational needs of students with Physical Disability and other
Health Impairment requires several modifications or adaptations. These will
be discussed under the five main headings:
Attitude
One of the first considerations in the effective teaching of individuals with
physical difficulties is a positive attitude towards the learner’s potentials and
limitations, understanding of his/her difficulties and the degree of educational
limitation it causes. The following methods will help teachers to address the
educational needs of learners with Physical Disabilities and other Health
Impairments:
The teacher sets up a buddy system in class so that other learners can assist the
child with physical or Health Impairments
Speak directly to the person, not to an accompanying support person
If you are not sure what to do, ask, “Can I help?”
Encourage students to tell you about any accessibility concerns
Incorporate into lessons/ and or wall hanging, examples of role models who
have Physical Disability
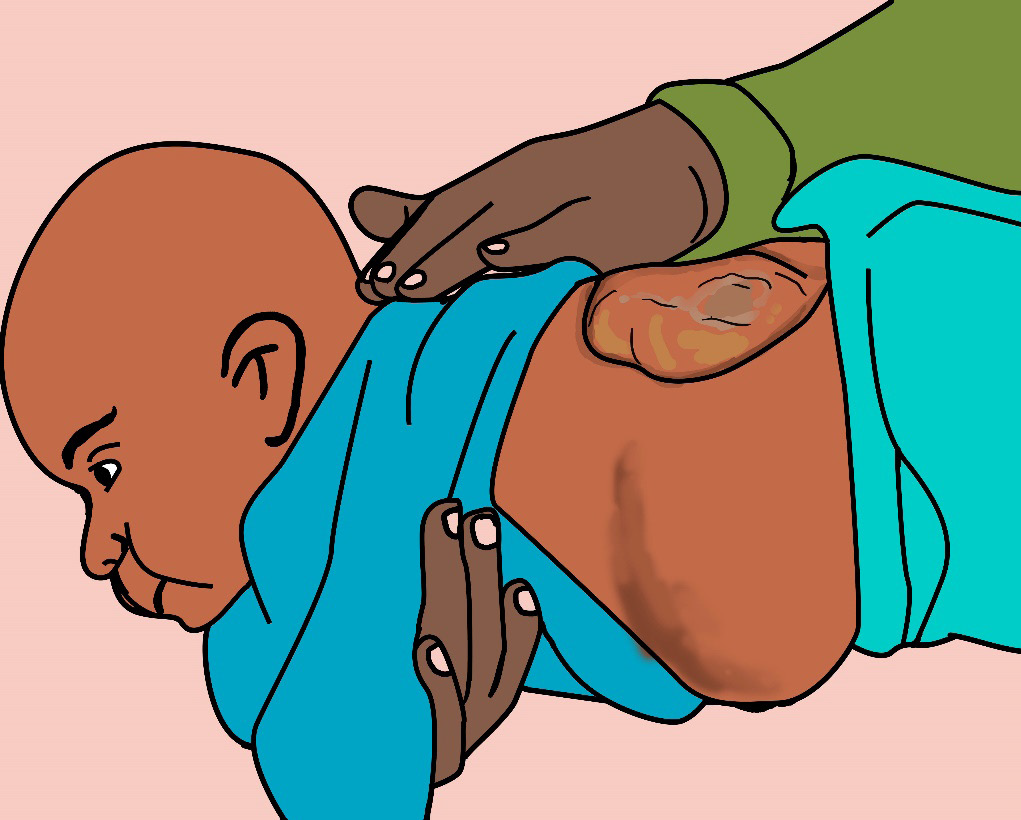
If the learner has a seizure attack, ensure the following:
• Remain calm to avoid emotional reactions from the learners
• Never try to restrain the learner because nothing can be done to stop a
seizure once it has begun
• Do not interfere with the movement in any way
• Talk to other teachers and learners to assure them that the condition
is not contagious
• Move the learner into horizontal position. Loosen his/ her collar, tilt
his/ her head sideways for release of saliva and place something soft
under the head
• After the learner has get full consciousness, let him/ her rest
Environmental arrangement
Construction of ramps to all areas to enhance accessibility to all facilities
Widening of the doors to enable movement of children on wheelchairs and
those using crutches
Avoid overcrowding the room so that there is ease in movement around.
Ensure the door handles are easy to manage and are low
Ensure the chairs, tables, beds and toilets are adapted to the learners’ heights
Clear the area around the learner so that no injury from hard objects occurs
Participation
Be aware that students with upper-body weakness or paralysis may be unable
to raise their hand. Make eye contact to include the student in classroom
discussions
Try to be considerate if the student with a Physical Disability is coming from
a long distance place; it may take the student longer to reach the school/
classroom
Have students with communication difficulties (as is the case with cerebral
palsy) use an alternative way of presentation in place of oral reporting
If writing is difficult, let the learner use a tape recorder, where one is available
or get a note taker
If a visit or trip is planned to somewhere outside the school, plan well in
advance to ensure that accessibility challenges on the journey and at the
destination can be tackled.
Plan activities at accessible locations so that all students can participate or,
as a last resort, substitute an alternative activity with the same learning outcomes
Consider alternative activities/exercises that can be used with less difficulty
for the learner, but has the same or similar learning objectives
Arrange for syllabus coverage for learners with Health Impairments since
they may miss class when their conditions are exacerbated.
Use appropriate learning, teaching aids and adapted physical education and
sport equipment
Refers the child (especially those with CP) for appropriate professional support
like: Speech therapist, physiotherapist, occupational therapists, guidance
and counselling specialist.
Assistive devices and technology
Provide assistive and compensatory devices such as wheelchairs, braces,
calipers, special boots depending on the challenges to enable the child
undertake school tasks
Consider an assistive device as an extension of the person’s personal space
Encourage learners who use crutches or other assistive devices to keep them
within easy reach. Make a suitable space available in the classroom near the
learners
Assignment and tests
Allow scheduled breaks during lectures, tests and exams
Allow more time for the learner to finish his/her work.
Provide different accommodations during exams. For example, provide
separate venue, provide extend time for learners with Cerebral Palsy or
Muscular Dystrophy, provide a scribe to those who are unable to write their
answers.
If appropriate, let the learner use computers during the exam (when the learner
has been using it in the instruction)
Where appropriate, give completely oral tests or completely written tests,
whichever suits the learner’s needs
Adapt some questions in exam without lowering the learning objectives. For
example, the teacher may ask a question: Which is the capital of Rwanda?
For a learner with severe cerebral palsy who is unable to talk or has difficulty
in writing, the teacher may reformulate the question and ask: The capital of
Rwanda is: a) Bujumbura, b) Kigali, c) Kampala
SELF-ASSESSMENT 4.5
1. Briefly explain which teaching strategies you would use to helplearners with Physical Disabilities.
SKILLS LAB
1. Visit a school that accommodate learners with Physical
Disabilities & OHI. Spend some hours in school. With reference
to the following points, prepare three pages’ document to advise
teachers and school in general how to effectively include learners
with Physical Disabilities:
• Categories of learners with Physical Disabilities
• School environment (open space, facilities, playground)
• Classroom environment (seating arrangement, teaching
methodologies)
• Attitude of teachers, peers and Learners with PD & OHI
themselves
END OF UNIT ASSESSMENT
1. What are the strategies needed to be put in place to support
learners with Physical and Health Impairments in school?
2. What would you do if a learner has a seizure attack in your class?
3. What are the common causes of Physical Disability?
4. Discuss how Asthma and HIV and AIDS may impact on learners
learning and development?
5. How may you identify children with Muscular Dystrophy in yourschool?
UNIT 5 LEARNERS WITH SPECIFIC LEARNING DIFFICULTIES
Key Unit Competence: Describe the characteristics of learners with
Learning Difficulties and use appropriate
methods to teach them
INTRODUCTORY ACTIVITY
Uwera had a very successful nursery and primary school experience until
primary three. In primary three things got a bit more difficult. Lack of
organization and her lack of ability to do written work began to destroy
her confidence and academic success. She was always the last in the class.
She had difficulties in mathematics and reading. She was unable to read
a text that a learner in primary two could read so easily. She was afraid of
mathematics and could hardly do a simple mathematical exercise. She never
brought assignments home, frequently did the wrong homework if she did
it at all and forgot to turn in completed homework. Her text books and note
books were all in a mess and her desk was always a muddle. Uwera was
however a sociable girl, beautiful and had very good computer skills, was
good in music and gymnastics. Her class teacher decided to call her parents
over her poor academic performance. Her parents revealed that Uwera was
born prematurely and her mother had complicated delivery. The mother
also revealed that Uwera experienced anoxia immediately after birth. After
her parents visit to the school, the teacher decided to change the way he was
teaching Uwera. He would allow Uwera to use the computer in all academic
assignments since she was good at using a computer. The teacher would
give Uwera remedial teaching after class to make sure she understood the
lesson. The gymnast teacher decided to nurture her talents. SinceUwera was
good at singing the teacher used songs to teach Uwera some mathematical
and reading concepts. Uwera recently represented Rwanda in singing and
dancing competition that took place in the USA. She represented Rwanda in
many other competitions as a gymnast and has received global recognition.
Uwera is an inspiration to many, an example of what a learner can be and do
if teachers are ready to support him/her. May God bless good teachers.
1. Uwera experienced difficulties in some academic areas. In which
areas Uwera had problems?
2. Explain what the teacher did to help Uwera popular/star3. What were the causes of Uwera’s shortcoming in academics?
5.1. Definition of Specific Learning Disabilities
ACTIVITY 5.1
1. You may have noticed that a learner may have difficulties in
reading, spelling but very bright in mathematics. How would you
explain this? What type of special educational needs does the
learner have?
2. How do we call learners who struggle academically, yet are very
smart?
Learners with Learning Disabilities have always been in our classrooms, but
teachers have often failed to identify these pupils and recognise their special
needs. These learners have been called names including” slow learners, hard to
teach, daydreamers, lazy, abaswa” etc.
Learning disabilities are neurologically-based processing problems. These
processing problems can interfere with learning basic skills such as reading,
writing and/or math. They can also interfere with higher level skills such as
organization, time planning, abstract reasoning, long or short-term memory
and attention. It is important to realize that learning disabilities can affect an
individual’s life beyond academics and can impact relationships with family,
friends and at the workplace.
The Individuals with Disabilities Education Act (IDEA) defines a specific learning
disability as “a disorder in one or more of the basic psychological processes
involved in understanding or in using language, spoken or written, that may
manifest itself in the imperfect ability to listen, think, speak, read, write, spell,
or to do mathematical calculations.”
However, as IDEA’s definition notes, “Specific Learning Disability does not
include learning problems that are primarily the result of visual, hearing, or
motor disabilities; of intellectual disability; of emotional disturbance; or of
environmental, cultural, or economic disadvantage.” This clause helps to
distinguish learning disabilities from the other disability categories.
SELF-ASSESSMENT 5.1
1. Explain the term” Specific Learning Disability”
2. Learning Disabilities are neurologically-based processing
problems. These processing problems can interfere with learningbasic skills. Which basic skills may be affected by this condition?
5.2. Types of Learning Disabilities
ACTIVITY 5.2
1. With reference to the definition of learning disabilities, which are
the areas that a learner with learning disabilities may struggle
with?
Learning Disabilities” is an “umbrella” term describing a number of other
specific learning disabilities. These specific learning disabilities include:
Dyslexia
A specific learning disability that affects reading and related language-based
processing skills. The severity can differ in each individual but can affect
reading fluency, decoding, reading comprehension, recall, writing, spelling, and
sometimes speech and can exist along with other related disorders. Dyslexia is
sometimes referred to as a Language-Based Learning Disability.
Dyscalculia
A specific learning disability that
affects a person’s ability to understand
numbers and learn math facts.
Individuals with this type of LD may
also have poor comprehension of
math symbols, may struggle with
memorizing and organizing numbers,
have difficulty telling time, or havetrouble with counting.
Dyspraxia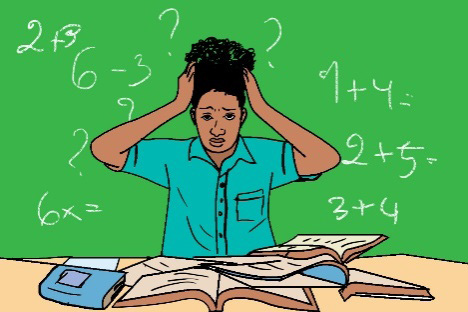
A disorder that is characterized by difficulty in muscle control, which causes
movement problems and coordination, language and speech, and can affect
learning. Although not a learning disability, dyspraxia often exists along with
dyslexia, dyscalculia or ADHD.
Dysgraphia
A specific learning disability that affects a person’s handwriting ability and fine
motor skills. Problems may include illegible handwriting, inconsistent spacing,
poor spatial planning on paper, poor spelling, and difficulty composing writingas well as thinking and writing at the same time.
Dysphasia, or aphasia
This is a type of speech disorder in which one has an impairment in the ability to
express speech, writing, signs, or has impairment in comprehension of spoken
word or language.
SELF-ASSESSMENT 5.2
1. Explain the various types of learning disabilities.
2. With an example, explain what dyslexia means?
5.3. Causes of Learning Disabilities
ACTIVITY 5.3
1. You now know what learning disabilities mean. What do youthink are the causes of learning disabilities?
Despite intense research activity over the year, pinpointing the precise cause
of learning disabilities has remained an elusive goal. In the varsity majority
of instances, the cause of a person’s learning disability remains unknown.
Just as there are many different types of learning disabilities, there appears
to be multiple etiological possibilities. Investigators suggest four basic
categories to explain the etiology of learning disabilities: Acquired trauma,
genetic/ hereditary influences, biochemical abnormalities and environmental
possibilities.
5.3.1. Acquired trauma
The medical literature uses the term acquired trauma when describing injury
or damage to the Central Nervous System(CNS) that originates from outside
the person and results in learning disorders. Depending on when the damage
occurs the trauma is identified as prenatal (before birth), perinatal (during
birth) or postnatal (after birth) These conditions have been linked to learning
problems in children. One example of an acquired trauma that may manifest
itself pre, peri or postnatal is brain injury, but a number of other factors have
also been implicated as possible causes of learning disabilities.
• Prenatal causes
Smoking
Illicit drugs
Use of alcohol
• Peri natal causes
Prolonged labour and difficult delivery
Anoxia
Prematurity/low birth weight
Trauma caused by medical instruments such as forceps
• Postnatal causes
Strokes
Concussions
Meningitis/ encephalitis
High fever
Head injury resulting from falls or accidents
5.3.2. Genetic Hereditary influences
Are learning disabilities hereditary? Researchers investigating this question
believe that some learning problems are indeed inherited. For example, reading
and spelling deficits are substantially inherited.
5.3.3. Biochemical abnormalities
This refers to the presence of certain chemical substances in our bodies. This
could be due to the inability of the body to metabolize certain vitamins, artificial
colouring and flavours used in some foods.
5.3.4. Environmental possibilities
Environmental factors that may cause SLD include:
• Nutrition: Severe malnutrition at an early age can affect the central
nervous system hence affect the learning and development of the child.
Food additives such as food colourings, flavours and preservatives used
in juices and foods may affect the brain of a developing foetus, hence
resulting into learning disability.
• Health: Diseases such as cerebral malaria, meningitis, mumps,
encephalitis and measles may affect the brain growth and developmentof a learner hence results into learning difficulties after recovery.
SELF-ASSESSMENT 5.3
1. Discuss how environmental factors can trigger learning
disabilities2. What are other causes of learning disabilities?
5.4. Characteristics of learners with Learning Disabilities
ACTIVITY 5.4
1. You now know the categories of learning disabilities, what are
the characteristics of:
• Learners with Dyslexia
• Learners with Dysgraphia
Characteristics of learners with Dyslexia
• Reads slowly and with difficulty
• Experiences decoding errors, especially with the order of letters
• Shows wide disparity between listening comprehension and reading
comprehension of some text
• Has trouble with spelling
• May have difficulty with handwriting
• Exhibits difficulty recalling known words
• Has difficulty with written language
• May experience difficulty with math computations
• Decoding real words is better than nonsense words
• Substitutes one small sight word for another: a, I, he, the, there, was
Characteristics of learners with Dyscalculia
• Shows difficulty understanding concepts of place value, and quantity,
number lines, positive and negative value, carrying and borrowing
• Has difficulty understanding and doing word problems
• Has difficulty sequencing information or events
• Exhibits difficulty using steps involved in math operations
• Shows difficulty understanding fractions
• Is challenged making change and handling money
• Displays difficulty recognizing patterns when adding, subtracting,
multiplying, or dividing
• Has difficulty putting language to math processes
• Has difficulty understanding concepts related to time such as days,
weeks, months, seasons, quarters, etc.
• Exhibits difficulty organizing problems on the page, keeping numbers
lined up, following through on long division problems
Characteristics of learners with Dysgraphia
• May have illegible printing and cursive writing (despite appropriate
time and attention given the task)
• Shows inconsistencies: mixtures of print and cursive, upper and lower
case, or irregular sizes, shapes or slant of letters
• Has unfinished words or letters, omitted words
• Inconsistent spacing between words and letters
• Exhibits strange wrist, body or paper position
• Has difficulty pre-visualizing letter formation
• Copying or writing is slow or laboured
• Shows poor spatial planning on paper
• Has cramped or unusual grip/may complain of sore hand
• Has great difficulty thinking and writing at the same time (taking notes,
creative writing.)
Characteristics of learners with Dyspraxia
• Exhibits poor balance; may appear clumsy; may frequently stumble
• Shows difficulty with motor planning
• Demonstrates inability to coordinate both sides of the body
• Has poor hand-eye coordination
• Exhibits weakness in the ability to organize self and belongings
• Shows possible sensitivity to touch
• May be distressed by loud noises or constant noises like the ticking of
a clock or someone tapping a pencil
• May break things or choose toys that do not require skilled manipulation
• Has difficulty with fine motor tasks such as colouring between the
lines, putting puzzles together; cutting accurately or pasting neatly
• Irritated by scratchy, rough, tight or heavy clothing
Characteristics of learners with Dysphasia, or Aphasia
• Difficulty remembering words
• Difficulty naming objects or people
• Difficulty speaking in complete sentences
• Difficulty speaking in any fashion
• Difficulty reading or writing
• Difficulty expressing thoughts and feelings
• Difficulty understanding spoken language
• Using incorrect or jumbled words
• Using words in the wrong order
SELF-ASSESSMENT 5.4
1. What are the characteristics of learners with the following
conditions?
• Dyspraxia
• Dysphasia, or Aphasia2. What signs or symptoms that a learner with dyslexia may display?
5.5. Teaching and learning approaches for learners with
Learning Disabilities
ACTIVITY 5.5
1. What strategies would you use to support learners who have writing
difficulties?
5.5.1. Teaching and learning approaches for learners with dyslexia
• Provide a quiet area for activities like reading, answering
comprehension questions
• Read aloud to learners regularly
• Mnemonics can help with spelling difficult words the learner always
struggles with (such as Big Elephants Can’t Always Use Small Exits to
remember the spelling of “because”).
• New concepts and vocabulary should be introduced gradually
• Use books with large print and big spaces between lines
• Provide meaningful reading materials such as dictionaries, categorized
list of words
• Dyslectic learners struggle with copying notes from the black board,
provide printed notes or assign someone to help her/ him with note
taking
• Let the child read aloud (oral reading). If the child makes mistakes,
they can be easily identified by the teacher and corrected
• Read as a group (choral reading). Here the children get both auditory
and visual stimulation to correct themselves.
• Use of colours also helps in providing some useful hints to children
who have problems with reading. For example, if the child confuses b
and d, b could be coloured with green and d with red
• Allow the use of a laptop or any other computer for in-class essays
• Use multi-sensory teaching methods
• Teach students to use logic rather than rote memory
• Present material in small units
5.5.2. Teaching and learning approaches for learners with dyscalculia
• Allow use of fingers and scratch paper
• Use diagrams and draw math concepts
• Provide peer assistance
• Use concrete material such as buttons, straws, seeds, pebbles and
beads to teach children how to count
• Use a lot of visual aids to teach simple mathematical operations and
concepts
• Concepts such as time and money should be linked to day to day events.
Use of meaningful vocabulary which includes phrases as tomorrow, in
five minutes, as soon as possible will help the child in increasing his/
her awareness about concepts related to time.
• Give smaller number of problems to these children. These children can
also be given some extra time to complete maths assignment.
• Suggest use of coloured pencils to differentiate problems
• Work with manipulatives
• Draw pictures of word problems
• Use mnemonic devices to learn steps of a math concept
• Use rhythm and music to teach math facts and to set steps to a beat
• Schedule computer time for the student for drill and practice
5.5.3. Teaching and learning approaches for learners withDysgraphia
• Provide sufficient time for writing activities
• Provide notes or outlines to reduce the amount of writing required
• Encourage the children to write more in a non-threatening environment.
This helps the children to gain confidence over themselves.
• Match the posture, pencil grip and position of the paper when a child
is writing.
• Have students form letters using clay
• Peers with good writing could also become models for those learners,
who manifest problems with writing.
• Suggest use of word processor
• Avoid chastising student for sloppy, careless work
• Use oral exams whenever necessary
• Allow use of tape recorder for lectures where necessary
• Allow the use of a note taker
• Reduce copying aspects of work
• Suggest use of pencil grips and /or specially designed writing aids
• Provide alternatives to written assignments (video-taped reports,
audio-taped reports)
5.5.4. Teaching and learning approaches for learners with Dyspraxia
• Pre-set students for touch with verbal prompts, “I’m going to touch
your right hand.”
• Avoid touching from behind or getting too close and make sure peers
are aware of this
• Provide a quiet place, without auditory or visual distractions, for
testing, silent reading or work that requires great concentration
• Warn the student when bells will ring or if a fire drill is scheduled
• Whisper when working one to one with the child
• Allow parents to provide earplugs or sterile waxes for noisy events
such as assemblies
• Make sure the parent knows about what is observed about the learner
in the classroom
• Refer student for occupational therapy or sensory integration training
• Be cognizant of light and light sources that may be irritating to child
• Use manipulatives, but make sure they are in learners’ field of vision
and don’t force student to touch them
5.5.5. Teaching and learning approaches for learners with Dysphasia,
or Aphasia
• Ensure that students have the opportunity for a quite environment.
• Teacher should communicate slowly, clearly, and repetitively using
gestures and pictures.
• Teacher should simplify sentence structure and reduce the rate of
speech
• Encourage student to be as independent as possible.
• Allow students as much time as needed without interruption to express
verbally.
• Provide word choice boards, vocabulary flashcards, and pictorial
representations.
• Explicitly teach semantics and syntax concepts.
• Present information using multiple modalities.
• Allow student to use many forms of expression such as writing,
drawing, choices, gestures, or yes/no responses.
• Allow students the opportunity to prepare anything that will be shared
in class.
• Allow alternative option to oral presentations such as visual
presentation or recording.
Examples:
In the classroom a teacher could allow a student with aphasia to submit a
verbal presentation by using a power point with written explanations for what
students would be verbalizing.
During testing student may be able to take alternative test in which they will be
able to express language in any way that works best for them. This could be all
verbally, in drawings, or in another form.
5.5.6. General interventions for learners with Learning Disabilities
• Show, demonstrate and model
• Utilize multi-sensory learning
• Avoid distractible surroundings
• Break information down into smaller units
• Allow plenty of time to these children to work upon a task as they have
poor time management skills
• These children need to do a task many times before they can master it
• Utilize peer tutoring and cooperative learning. In peer tutoring, allow
the child with a learning disability to be a tutor also
• Make information as concrete as possible
• Read test materials to the student
• Find out how the student learn best and utilize the learning channel
• Remember that ‘Individualization’ does not always mean a student
has to be taught one to one, it simply means the programme should be
tailored to the student’s needs and capabilities
• Praise and encouragement are the key words in channelizing the effortstowards these children’ s learning in the right direction
SELF-ASSESSMENT 5.5
1. How would you help a learner with dyscalculia in your classroom?
2. What strategies would you use to help a learner with aphasia
improve his/ her academic works?
SKILLS LAB
Visit a nearest school, identify a child with SLD, write a two-page document
on strategies you can use to help that child.
END OF UNIT ASSESSMENT
3. What is a Specific Learning Disability?
4. How can you identify a learner with the following conditions?
• Dyslexia
• Dysgraphia
• Dyscalculia
5. In groups, discuss the specific learning disability you may havenoticed with learners and how you helped them
UNIT6 LEARNERS WITH COMMUNICATION DIFFICULTIES: (SPEECH AND LANGUAGE DIFFICULTIES)
Key Unit Competence: Identify the characteristics of learners with speech
and language difficulties and use appropriate
approaches to teach them
INTRODUCTORY ACTIVITY
Adam was a typical child at birth. He looked normal. At birth he was 4.1kg,
very healthy and went through all developmental milestones at normal
times. He crawled at six months and uttered his first word at 12 months.
His speech and language continued to develop normally. However, when it
was time to eat solid food, Adam did not want to eat any foods that were not
pureed. By the time Adam was 3 years old, he could not pronounce n, t,d, l
and s correctly. When Adam was 4 years old, he could hear what you say, but
not understand. For example, her mom would ask him to go and wash his
hands after eating, and he would ask several times” I do what?”. Her mom
would repeat, rephrase the sentences but still Adam would not understand
what her mom says. Adam did not seem to understand simple directions,
question words like why, how, sequencing, verb tense and common language
concepts. He was not acquiring language concepts that children learn
without formal teaching, and his pronunciation was not getting better. When
Adam was in primary one, the teacher noticed that he did not understand”
yes” and “no “questions and when asked simple things that he was supposed
to know at his age, he would say” I don’t know”. Adam was still a picky boy
and would eat selected food. The teacher advised the parents to take Adam
to the speech pathologist at King Faisal Hospital. Adam was diagnosed with
mild to moderate language disorder, mild articulation difficulty, low facial
muscle tone and mild degree of hearing impairment. With the help of the
teacher, parents and speech pathologist, Adam has made great progress.
He has matured socially and improved his speech and language skills. His
teacher said that Adam is a smart boy who has courage and determination to
improve on his language difficulties. He said that his future is bright.
1. Briefly explain the challenges that Adam encountered?
2. Explain the roles of different people who helped Adam in his struggle
to improve his language.
6.1. Definition and categories of Communication Difficulties:
Speech and Language Difficulties
ACTIVITY 6.1
1. What do you understand by the word” Communication”?
2. Have you ever met people who have communication difficulties?
How would you define communication difficulties?
3. What is the difference between speech and language?
Definition of communication
Communication is the process of sending and receiving messages through
verbal or nonverbal means, including speech, or oral communication;
writing and graphical representations (such as infographics, maps, and charts);
and signs, signals, and behaviour. More simply, communication is said to be
«the creation and exchange of meaning.”
Communication is a very important aspect of human life. Our lives revolve
around communication in many crucial ways. Despite its importance and
constant presence in our live, we seldom think much about communication
unless we have a problem with it. It is also the one of the most interrelated
processes people undertake. Speech and Language are two highly interrelated
components of communication. Problems in either can significantly affect a
person’s daily life.
Difference between Speech and Language
Speech is verbal communication with others. A child, when he has not learnt the
rules of a language, blurts out in monosyllables and yet his mother understands
what he means. Speech is all about sounds, and a small child learns gradually
the correct sounds that make up speech. For a kid who is still learning the rules
of a language, speech is the only way to communicate with others.
Speech is articulation of language into sounds using voice and fluency. Some
have speech problems that need attention from speech therapists. If a kid has
problems expressing him/herself, or others do not understand what he is
trying to say, it is said that he has a speech problem. It occurs because there
is no synchronization between his lip and tongue movement along with the
sounds he is trying to make. This is also the case with an adult when he suffers
from a stroke making it difficult to speak fluently.
Language
Language is a tool that allows people to communicate with each other. It consists
of words that can be joined in a meaningful manner to express an idea. Different
languages have different rules and, sometimes, people who are not native to a
language find it difficult to understand the idea behind a message. For example,
in English language, it is raining cats and dogs might sound alien to someone
whose native language is not English as he cannot think of raining cats and
dogs, but those whose first language is English know pretty well that it just
means raining hard. Language, apart from speech, can be expressed by writing
the text, which is one mode to read and understand much about a language.
While speech involves the physical motor ability to talk, language is a symbolic,
rule governed system used to convey a message. In English, the symbols can be
words, either spoken or written.
Communication Difficulties
Communication difficulties are defined as an observed disturbance in the
normal speech and language process. These may include process of listening,
speaking, reading, writing and thinking.
Communication difficulties can be classified into two:
• Speech difficulties
• Language difficulties
6.1.2. Speech difficulties
Speech difficulties refers to difficulties producing sound as well as difficulties
of voice quality and fluency. Speech involves the production and articulations of
sounds in the language. Indicators of speech difficulty may be seen in a learner
if he or she produces speech that deviates from normal speech as compared to
others. Speech difficulties in a learner may be noted when there is lack of fluency
in speech, poor pronunciation of words and problems in voice production.
There are three main types of speech difficulties, these are:
• Articulation difficulties
• Fluency difficulties
• Voice difficulties
Let us look at each of them.
6.1.1. 1. Articulation difficulties
An articulation difficulty is a speech difficulty related to problems of
pronunciation. A child with articulation difficulty may find it difficult to
articulate sounds in isolation or in sentences. The child may either:
• Pronounce the sound wrongly
• Omit it in words
• Substitute it for another or
• Add an additional sound next to it whenever it occurs in words or
sentence
There are four main types of articulation difficulties. These are:
Mal- articulating: This refers to the wrong pronunciation of words for
example/b/ whenever it occurs.
Omissions: This involves deleting or dropping certain consonants from words
by rendering speech unintelligible. For example, “boy” may be pronounced as/
oy/
Substitution: This involves substituting one-word sound with another such
as/w/ for/r/, as in “right” which is sounded as “weight” or substitution of /w/
for /l/ as in “yellow” where it is sounded as “yewo”
Additions: This is where a learner adds vowels sounds to words ending with
consonants such as” eat” may be pronounced” eati”
6.1.1.2. Fluency Difficulties
Fluency of speech is significant problem for persons with a fluency disorder.
Their speech is characterized by repeated interruptions, hesitations or
repetitions that seriously interfere with the flow of communication. Fluency
difficulty is therefore a condition where one is unable to talk in an easy
and relaxed way resulting in an unnaturally hesitant speech. For example,
stammering/ stuttering will affect the smooth flow of speech. Learner with
fluency difficulties may have:
Prolongation: A Learner who is a stammer/ stutter tend to abnormally
prolong sounds in words. For example, the word “tomato” may be pronounced
as” to…………. mato”
Repetition: This refers to when a learner who stammers repeats a sound or
syllable in words or sentences. For example,” H-h-h-h-h-e-a-a-a-a-arrived-h-hh-
h home-l-l-l-l-late”
Complete blockage: This is when a learner gets stuck during the pronunciation
of the first sound of a word. For example, for “Umushyitsi” the learner may only
sound” U”.
6.1.1.3. Voice difficulties
These are abnormalities due to the pitch, intensity and quality of one’s voice. The
following are the main voice difficulties that may be experienced by children:
• Absence of voice: Some children may not be able to produce any
sound due to problems in the vocal cords
• Hoarse voice: Hoarse or husky voice may be due to misuse or abuse
of the voice which strains the vocal cords. The cords may be strained
during shouting, cheering or moaning for a long time.
• Too high or too low picked voice: We vary the pitch of voice in
order to produce pitch with relevant tone and intonation to convey
the intended meaning. Some children use too high or too low pitch or
monotonous voice which interferes with meaning.
• Too loud or too soft voice: We vary the intensity of our voice when
we are speaking depending on the situation and context. For example,
we tend to raise our voice when we are speaking to somebody at a
distance, when addressing a large crowd or when emphasizing a point.
We whisper when telling a secret and we tend to talk in low tones when
distressed and shout when excited. Learners with voice difficulties
may be unable to vary their voices.
6.1.2. Language difficulties
There are two main types of language difficulties. These are:
• Receptive Language difficulties
• Expressive language difficulties
6.1.2.1. Receptive Language difficulties
Learners with receptive language difficulties may not be able to perceive or
comprehend spoken or written language due to inability to:
• Assign meaning to words they hear or read because they have not
formed the concepts of the objects and event, they describe
• Understand different parts of language such as nouns, verbs, adjectives
and plurals
• Interpret intonation and stress patterns in utterances
• Understand different sentences because they have not mastered how
they are formed
• Hear or read due to sensory difficulties
• Retain and recall words read or heard before responding accordingly
6.1.2.2. Expressive Language difficulties
Expressive language involves conceptualization of message, symbolization and
memorizing the messages, use of intonation and stress, general use of language,
use of senses, use of speech and use of voice and generally use of the body. You
may find that learners have difficulties in some or most of these areas. Learners
with expressive language difficulties have problems in:
• The use of symbols: Some learners have difficulties with mastering
the use of the linguistics symbols such as sounds, letters or signs that
convey meaning in language
• Memory problems: Memory problems may occur when a learner is not
able to retain words already acquired for later life, recall the sequence
of sounds and letters in words and sentences.
• Problems with the use of appropriate intonation and stress: Some
learners use flat and monotonous voices, which lack proper intonation
and stress. As a result, they are unable to convey the intended meaningof a given utterance.
SELF-ASSESSMENT 6.1
1. Explain the term” Communication difficulties”
2. Describe the two components of communication
3. Describe the two main types of language difficulties?
6.2. Causes and characteristics of Communication Difficulties:
Speech and Language Difficulties
ACTIVITY 6.2
1. Do you attribute children’s language development to a natural
process or do you think environment plays a role in the
development of language in children?
2. Think about the learner you have met with and suspected to
be having communication difficulties. List some characteristics
which suggest that one has a communication difficulty?
Causes of language difficulties are different from those of speech difficulties.
6.2.1. Causes of speech difficulties
Main causes of speech difficulties include:
• Structural defects affecting the organs of speech. For example, cleft
palate or cleft lip
• Psychomotor difficulties such as difficulty in activating the organs of
speech to move and control their movement in order to produce a
particular sound. For example, a patient with paralysis may not be able
to move the tongue or lips to produce a sound
• Delayed language development as a result of delayed growth and
development hence lagging behind their peers
• Hearing Impairments is a major cause of articulation difficulties.
6.2.2. Causes of language difficulties
Main cause of language difficulties is brain damage or deficits affecting the
areas of the brain dealing with language. This may lead to the following:
• Memory deficits
• Encoding and decoding difficulties
• Problems related to vocabulary acquisition and sentence construction
• Attention deficits
• Inability to associate the message received through the sense and what
they symbolize or with previous experience.
Characteristics of learners with communication difficulties
Learners with communication difficulties may display the following
characteristics:
• May experience problems learning subject content that demand oral or written
language
• Too low or too high pitch
• Not taking part in conversations
• May tend to speak in isolated words and short sentences
• Difficulty putting words together to make sentences
• Using unintelligible speech
• Not responding to voices or everyday sounds
• Stammering or stuttering
• Speaking too fast• Substituting, omitting, distorting or adding speech sounds
SELF-ASSESSMENT 6.2
1. Discuss the causes of speech difficulties?
2. Elaborate on different triggers of language difficulties?
3. Discuss the characteristics of learners with Speech and Language
difficulties
6.3. Teaching and learning approaches for learners with
communication difficulties: Speech and Language impairment
ACTIVITY 6.3
1. What do you think parents and teachers should do to help a child
with communication difficulties?
The role played by the parents and teachers in the development of the child’s
communication is central in the child’s language development. However, it is
important to note that the foundation of the child’s language begins at home
and is later supplemented by teachers as soon as the child enters school.
The following are approaches that teachers and parents might use to help
learners with communications difficulties:
• Interact with the child right from birth and throughout childhood in
order to establish a bond which is the corner stone of communication
• Encourage the child’s siblings and peers to involve him/ her in their
activities
• Engage the child in all activities that are done by his or her age mates
• Exposing the child through visits to social functions, places of interest
friends and relatives
• Refer the learner to education assessment centre for assessment and
early intervention
• Refer them to other professionals such as speech therapists, Ear, Nose
&Throat(ENT) specialist, occupational therapist and physiotherapists.• Engage Sign Language interpreters in case of a child who is deaf
SELF-ASSESSMENT 6.3
1. Explain the role played by both teachers and parents in the
communication development of the child?
2. Which other ways may teachers use to support learners with
communication difficulties
SKILLS LAB
1. Visit a nursery school and identify a child expected to have
communication difficulties. Spend three hours with the child.
Write down all the characteristics of the child and suggest
strategies you could use to help that child improve her/ his
language and speech.
END OF UNIT ASSESSMENT
1. What are some of the language difficulties observed in children?
2. Discuss the three broad categories of speech difficulties and give
an example of each
3. Discuss the role that teachers may play to support learners withCD?
UNIT 7 LEARNERS WITH DOWN SYNDROME
Key Unit Competence: Explain the characteristics of leaners with Down
syndrome and use appropriate methods to teach
themINTRODUCTORY ACTIVITY
Observe those pictures and respond to the following questions:
1. What are common physical features do the children on the pictures
have?
2. At your school, surrounding areas or in your community, have you
seen or met someone with the same physical features? If yes what
other characteristics have you observed about that person (in regard
to his/her intellectual abilities, speech or communication skills, social
skills, etc)
7.1. Definition, causes and types of Down syndrome
ACTIVITY 7.1
– What is the Definition of Down syndrome?
– What causes Down syndrome– Types of Down syndrome
7.1.1. What is Down syndrome?
Down syndrome is a condition in which a person has an extra chromosome.
Chromosomes are small “packages” of genes in the body. They determine how
a baby’s body forms during pregnancy and how the baby’s body functions
as it grows in the womb and after birth. Typically, a baby is born with 46
chromosomes. Babies with Down syndrome have an extra copy of one of these
chromosomes, chromosome 21. A medical term for having an extra copy of a
chromosome is ‘trisomy.’ Down syndrome is also referred to as Trisomy 21.
This extra copy changes how the baby’s body and brain develop, which can
cause both mental and physical challenges for the baby.
Why is Down Syndrome Referred to as a genetic condition?
The human body is made of cells; all cells contain a centre, called a nucleus, in
which genetic material is stored. This genetic material, known as genes, carries
the codes responsible for all our inherited characteristics. Genes are grouped
along rod-like structures called chromosomes. Normally, the nucleus of each
cell contains 23 pairs of chromosome, half of which are inherited from each
parent. In individuals with Down syndrome, however, the cells usually contain
47, not 46, chromosomes; the extra chromosome is the 21st. This excess genetic
material, in the form of additional genes along chromosome 21, results in Down
syndrome. The extra 21st chromosome is detected by using a procedure called
a karyotype. A karyotype is a visual display of the chromosomes grouped by
size, number and shape. Chromosomes may be studied by examining blood
or tissue cells. Individual chromosomes are identified, stained and numbered
from largest to smallest. Ninety-five percent of occurrences of Down syndrome
result from the presence of an extra (third) chromosome, a condition described
as Trisomy 21.
7.1.2. The cause of Down syndrome
Down syndrome is usually caused by an error in cell division called
nondisjunction. However, two other types of chromosomal abnormalities,
mosaicism and translocation, are also implicated in Down syndrome although
to a much lesser extent. Regardless of the type of Down syndrome a person
may have, all people with Down syndrome have an extra, critical portion of
chromosome 21 present in all or some of their cells. This additional genetic
material alters the course of development and causes the characteristics
associated with the syndrome.
Nondisjunction: Nondisjunction is a faulty cell division that results in
an embryo with three copies of chromosome 21 instead of the usual two.
Prior to or at conception, a pair of 21st chromosomes in either the sperm or
the egg fails to separate. As the embryo develops, the extra chromosome is
replicated in every cell of the body. This error in cell division is responsiblefor 95 percent of all cases of Down syndrome.
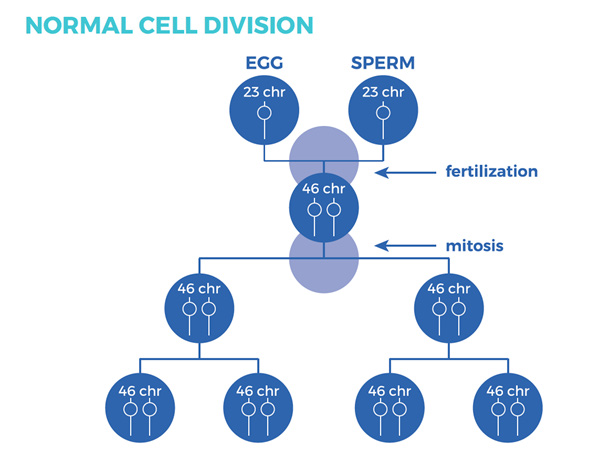
During fertilization, the 23 chromosomes from the egg and sperm combine. The resulting fertilized
egg has 46 chromosomes. During mitosis, the cell replicates itself and divides into two cellswith 46 chromosomes in each.
Nondisjunction is the failure of the pair of chromosomes to separate during meiosis, which is the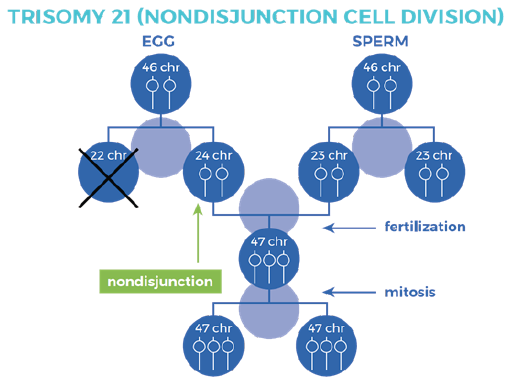
process by which egg and sperm cells replicate themselves and divide. Nondisjunction results inboth 21stchromosomes being carried to one cell and none to the other.
Note: It is not currently known why nondisjunction occurs, although researchhas shown that it increases in frequency as a woman ages.
Incidence of Down syndrome and maternal age
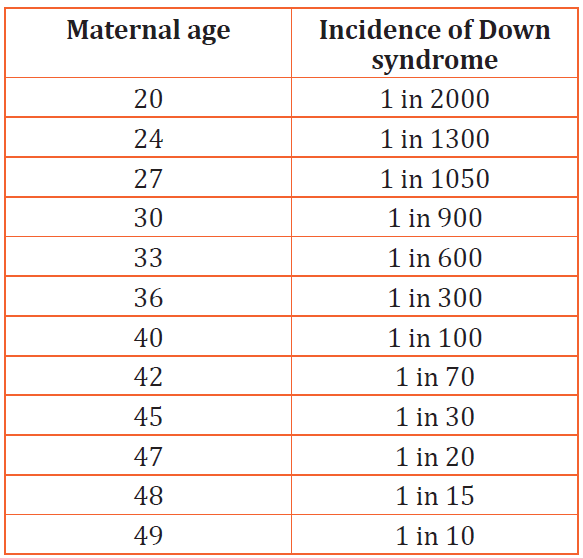
7.1.3. Types of Down syndrome
There are three types of Down syndrome. People often can’t tell the difference
between each type without looking at the chromosomes because the physical
features and behaviors are similar.
• Trisomy 21: About 95% of people with Down syndrome have Trisomy
21. With this type of Down syndrome, each cell in the body has 3
separate copies of chromosome 21 instead of the usual 2 copies.
• Translocation Down syndrome: This type accounts for a small
percentage of people with Down syndrome (about 3%). This occurs
when an extra part or a whole extra chromosome 21 is present, but it
is attached or “trans- located” to a different chromosome rather than
being a separate chromosome 21.
• Mosaic Down syndrome: This type affects about 2% of the people
with Down syndrome. Mosaic means mixture or combination. For
children with mosaic Down syndrome, some of their cells have 3
copies of chromosome 21, but other cells have the typical two copies of
chromosome 21. Children with mosaic Down syndrome may have the
same features as other children with Down syndrome. However, they
may have fewer features of the condition due to the presence of some(or many) cells with a typical number of chromosomes.
SELF-ASSESSMENT 7.1
1. What is Down syndrome?
2. In few words explain the cause of Down syndrome
3. List three types of Down syndrome
7.2. Characteristics of children with Down syndrome and
strategies to teach them
ACTIVITY 7.1
– What are characteristics of children with Down syndrome
– What are strategies to help children with Down syndrome inthe classroom
7.2.1. Characteristics of children with Down syndrome
Children with Down syndrome can be identified based on their body shape and
size, facial features, intellectual or learning ability.
a. Identifying a child with Down syndrome by body shape and size Look for low muscle tone
Babies with low muscle tone are usually described as floppy or feeling like a
“rag doll” when held. This condition is known as hypotonia. Infants usually
have flexed elbows and knees, whereas those with low muscle tone have loosely
extended joints.
• While infants with normal tone can be lifted and held from under the
armpits, babies with hypotonia typically slip from their parents’ hands
because their arms rise without resistance.
• Hypotonia results in weaker stomach muscles. Therefore, the stomach
may extend outward more than usual.
• Poor muscle control of the head (head rolling to the side or forward
and backward) is also a symptom. Look for shortened height
Children affected by Down syndrome often grow slower than other children,
and are therefore shorter in stature. Newborns with Down syndrome are
usually small, and a person with Down syndrome will most likely remain short
through adulthood. A study conducted in Sweden shows that the mean birth
length is 48 centimeters (18.9 inch) for both males and females with Down
syndrome. In comparison, the average length for those without the disability
is 51.5 cm. Look for a short and wide neck
Also look for excess fat or skin surrounding the neck. In addition, neck instability
tends to be a common issue. While neck dislocation is uncommon, it is more
likely to occur in people with Down syndrome than those without the disability.
It is necessary to be aware of a lump or pain behind the ear, a stiff neck that
doesn’t heal quickly, or changes in the way a person walks (appearing unsteadyon their feet).
Look for short and stocky appendages
This includes legs, arms, fingers, and toes. Those with Down syndrome often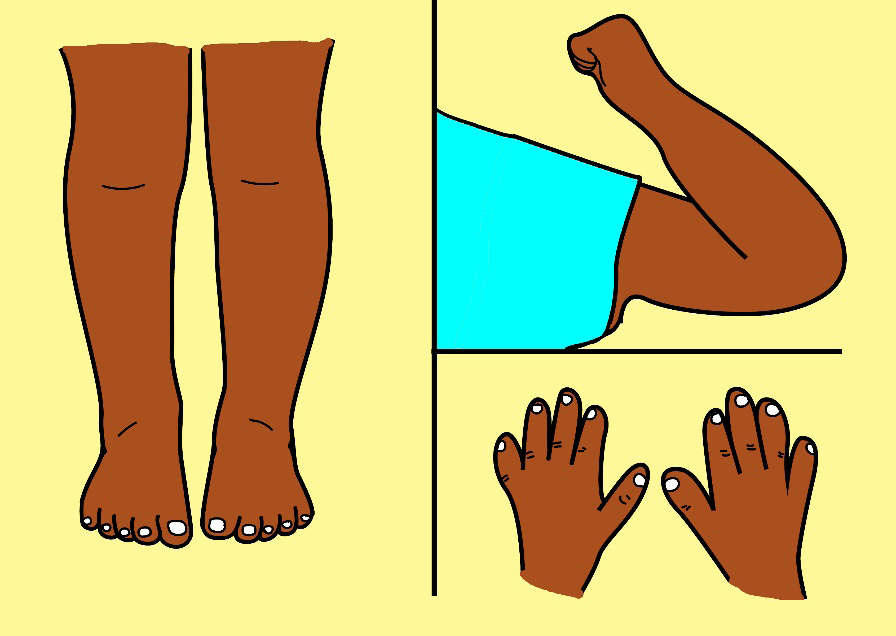
have shorter arms and legs, a shorter torso, and higher knees than those
without it.
• People with Down syndrome often have webbed toes, which is
distinguished by the fusing together of the second and third toe.
• There may also be a wide space between the big toe and second toe,
and a deep crease on the sole of the foot where this space is.
• The fifth finger (pinky) can sometimes only have 1 flexion furrow, or
place where the finger bends.
• Hyper flexibility is also a symptom. This is identifiable by joints that
seem to easily extend beyond the normal range of motion. A child with
Down syndrome may easily “do the splits,” and may be at risk of falling
over as a result.
• Having one singular crease across the palm of the hand, and a pinky
finger that curves towards the thumb are additional characteristics.
b. Identifying a child with Down syndrome by facial features Look for a small, flat nose
Many people with Down syndrome are described as having flat, rounded, wide
noses with small nasal bridges. The nasal bridge is the flat section of the nose
between the eyes. This area can be described as being “pushed in. Look for slanted eye shape
Those with Down syndrome usually exhibit round eyes that slant upwards.
While the outer corners of most eyes usually turn downward, those with Down
syndrome have eyes that turn upward (almond-shaped). Look for small ears
People with Down syndrome tend to have smaller ears that are set lower on the
head. Some may have ears whose tops fold over slightly. Look for an irregularly shaped mouth, tongue, and/or teeth
Due to low muscle tone, the mouth may appear to be turned downward and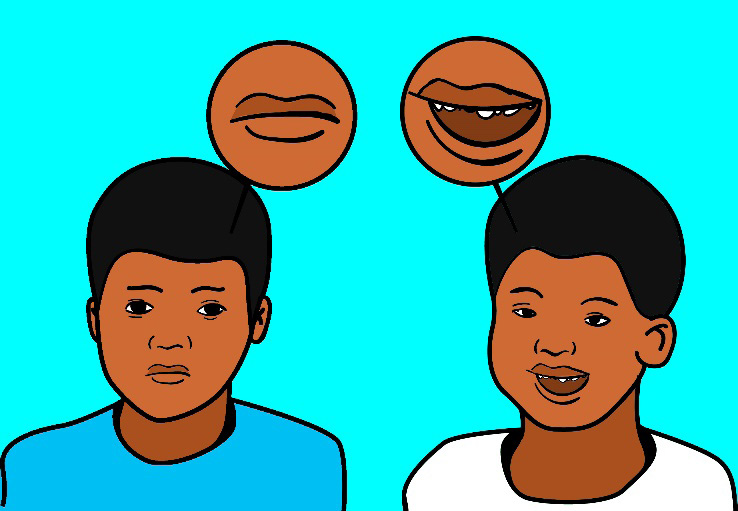
the tongue may protrude from the mouth. Teeth may come in later and in a
different order than usual. Teeth may also be small, unusually shaped, or out
of place.
c. Identify learners with Down syndrome by looking at their
developmental and intellectual abilities
All people with Down syndrome experience cognitive delays, however, the
effect is usually mild to moderate and is not indicative of the many strengths
and talents that each individual possesses. Children with Down syndrome learn
to sit, walk, talk, play, toilet train and do most other activities only somewhat
later than their peers without Down syndrome.
Speaking may or may not pose a challenge for an individual with Down syndrome.
It all depends on the person. Some learn sign language or another form of
alternative communication instead of speaking. People with Down syndrome
easily grasp new words and their vocabularies become more advanced as they
mature. Because grammar rules are inconsistent and hard to explain, those
with Down syndrome may have difficulty mastering grammar. As a result, they
usually use shorter sentences with less detail. Expression can be hard for them
because their motor skills are impaired. Speaking clearly may also present a
challenge. Many people with Down syndrome benefit from speech therapy.Developmental Milestones
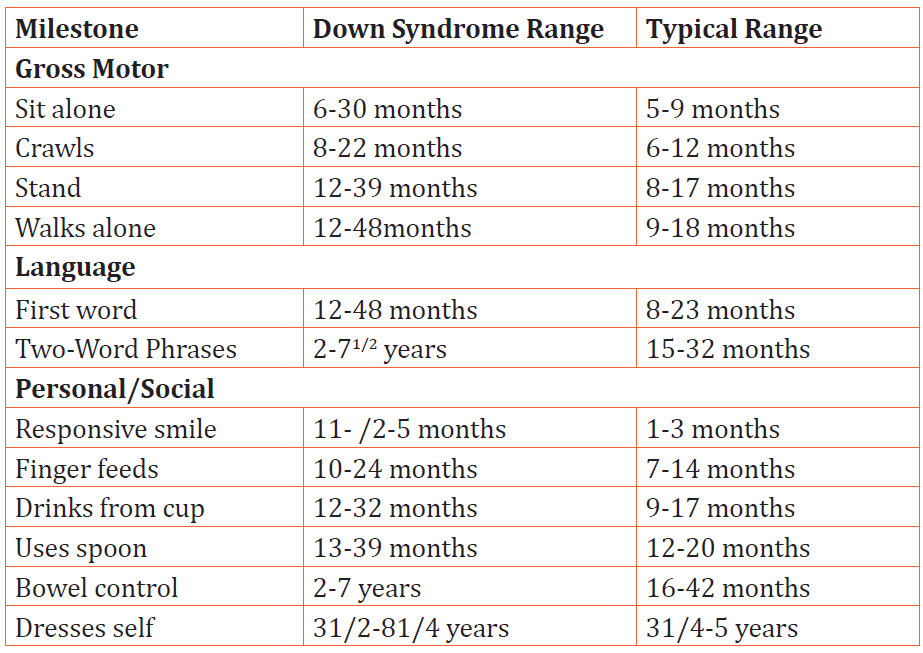
7.2.2. Strategies to help learners with Down syndrome
– Use teaching methods that involve cues and objects
– Pair pictures with spoken words
– Present information visually (e.g. overhead projector, posters, pocket
charts, chalkboard)
– Use simple directions
– Break down directions into small steps
– Allow adequate response time
– Assign fewer problems to a page
– Give students more freedom to choose their work activities
– Foster independence and self-reliance by balancing developmental
and chronological needs as higher academic expectations are set in the
classroom
– When presenting independent work, try to divide it into small segments
(e.g. fold test in half).
– Allow extra time to complete tasks. Reduce length of assignments
– Avoid large group and whole class instruction as they are least effective
– Be aware that some students may lack the fine motor coordination to
use a keyboard and mouse effectively.
– Assistive and/or adaptive equipment such as specialized key guards or
alternative keyboard can be used
– Minimize distractions. When choosing stimuli or objects, ensure that
they have clear and obvious dimensions that vary on as few dimensions
as possible (e.g., colour, size, texture)
– Pay attention to seating. Avoid seating students with Down syndrome
near a window, door or high traffic area
– Give immediate feedback or praise to ensure that students associaterewards with their efforts
SELF-ASSESSMENT 7.2
1. Identify the characteristics of children with Down syndrome
2. Explain 5 approaches to teach learners with Down syndrome
SKILLS LAB
Visit a special center or school that have children with different types of
disabilities. Identify children with Down syndrome. Observe identified
children/child in the classroom during teaching time. Finally, advice the
teacher in regards to suitable teaching approaches to be used in order
to respond to the needs of these learners with Down syndrome.
END OF UNIT ASSESSMENT
1. What is Down syndrome?
2. What does nondisjunction mean?
3. In few words, explain why Down syndrome is referred to as a
genetic condition?
4. How can you identify a child with Down syndrome?
5. List 5 approaches to be used when teaching learners with Downsyndrome
UNIT8 LEARNERS WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD) AND LEARNERS AUTISM
Key Unit Competence: Explain the characteristics of learners with autism
and ADHD and use appropriate approaches to
teach them
INTRODUCTORY ACTIVITY
Kalisa is a 13-year boy and was born in rural village. In his daily activities
he had inattention to accomplish tasks and was not able to follow some
instructions because of his hyperactivity. His parents had tried to take him
to the nearest school in order to help him but his condition did not improve.
He interrupted his classmates during class activities (taking notes, talking,
throwing things, etc.). During break time he would run, jump and drive
imaginary vehicles. Even though he was overactive he was also interested in
playing music with piano or guitar and singing. His teacher had discovered
that Kalisa may be good at music and then oriented him to another teacher
who could use appropriate techniques to teach music and musical instrument
playing to Kalisa. The teacher advised his parents to take him to a specialist,
this they gladly did and Kalisa was diagnosed with ADHD (Attention Deficit
Hyperactive disorder). In three years later Kalisa was able to play the piano
and sing some songs. His parents became happy because of their child’sattainment and his parents want to support him to make album of his songs.
Question:
1. Describe Kalisa’s behaviours in her class and outside?
8.1. Learners with Attention Deficit Hyperactivity Disorder
(ADHD)
8.1.1. Definition, causes and characteristicsof Attention Deficit
Hyperactivity Disorder (ADHD)
ACTIVITY 8.1.1
Use books or other sources of information to answer the following
questions:
2. What do you understand by Attention Deficit Hyperactivity
Disorder (ADHD)?
3. According to you, what do you think as risk factors of ADHD?
4. What do you understand by the following terms?
• Inattention
• Hyperactivity
• impulsivity
Definition of Attention Deficit Hyperactivity Disorder
Attention Deficit Hyperactivity Disorder is defined as persistent pattern of
inattention and/or hyperactive impulsivity that is more frequent and severe
than is typically observed in individual at a comparable level of development.
In order to make clear the meaning of ADHD, there are guidelines that help
everyone to describe it but even though those criteria may seem to happen to
every person, also there is a persistent or a chronic condition for those who
have Attention Deficit Hyperactive Disorder which makes some differences. It
is believed to affect around 3 to 5 percent of children who are or before 7 years
old. It is a chronic condition that affect a million of children in the world and
often continues in adulthood. It a combination of persistent problem such as
sustaining attention, hyperactivity and impulse behaviours.
Causes of Attention Deficit Hyperactivity Disorder (ADHD)
The exact cause of ADHD is not well known but researchers explore possible
possibilities including neurological foundations, hereditary and environmental
conditions.
Neurological foundation: using the neuroimaging technology,
researchers found that some parts of brain appear to exhibit
abnormalities in persons with ADHD. The front lobes are one part
of the brain in charge of executive functions such as self-regulation,
working memory, inner speech. The basal ganglia are responsible in
controlling and coordination of motor behaviour. Attention Deficit
Hyperactive Disorder results from dysfunction of neurotransmitter ofdopamine in the region of the brain that control activity and attention.
Hereditary factors: There is strong evidence of the role of heredity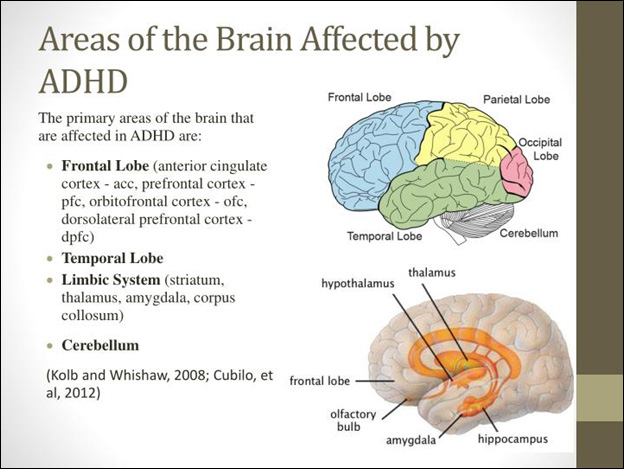
in contributing to ADHD. Family studies revealed that a child who
has ADHD is more likely to have a parent who exhibit ADHD (Barkley,
2006). Also, the investigating of monozygotic (identical) and dizygotic
(fraternal) twins have consistently found a high concordance of ADHD
in identical twins that in fraternal twins.
Environment factors: Virous pre-, peri-, postnatal traumas are
also implicated as contributing to Attention Deficit Hyperactive
Disorder (ADHD). Some example of environmental factors includes
maternal smoking and alcohol abuse, lead poisoning, low birth
weight and prematurity. There are other many environmental
factors that researchers found to be typical examples but with
poor scientific support such as too much/little sugar, badparenting, too much television, food addictive/colouring, yeast.
Characteristics of learners with Attention Deficit Hyperactivity
Disorder (ADHD)
Attention Deficit Hyperactivity Disorder is the chronic nature of characteristic
and their duration that often lead to impaired functioning in activities of daily
living. ADHD has three subtypes:
ADHD with inattentive type, inattention indicates that child might have
attention span, or difficulties of sustaining his or her attention for more
than a brief period of time.
ADHD with predominantly hyperactive-impulsive type, Hyperactivity
is a condition in which a child is easily excitable or over-active.
Impulsivity is the inability to think first before resorting to an action.
ADHD with combined inattentive and hyperactive-impulse types.
ADHD has criteria for each of those subtypes. Six of these following symptoms
may lead to confirm an ADHD if these symptoms last for 6 months to a degree
that is maladaptive and inconsistent with developmental level.
Characteristics of learners ADHD by each subtype
Characteristics of Inattention
• Often fail to give close attention to details or makes careless mistake in
schoolwork, work or other activities.
• Have difficulties of sustaining attention in tasks or play activities.
• Often does not seem to listen when spoken to directly.
• Does not follow through on instructions and fails to finish school work,
chores, duties in the workplace (not due to oppositional behaviour or
failure to understand instructions)
• Often avoid, dislike, or is reluctant to engage in tasks that require
sustained mental efforts (school work and home work)
• Often loose things necessary for tasks or activities (e. g: toys, school
assignments, pencils, books, or tools)
• Is often easily distracted by extraneous stimuli.
• Is often forgetful in daily living
Characteristics of learners Hyperactivities
• Often fidgets with hands or feet or squirms in seat
• Often leave seats in classroom or in other situations in which remains
seated is expected
• Often runs about, claims excessively in situation in which it is
inappropriate
• Often has difficult in playing or engaging in leisure activities quietly
• Talk excessively
Characteristics of learners Impulsivity
• Often blurts out answers before questions have been completed
• Often has difficult of awaiting turn
• Often interrupts or intrudes on others (e. g: butts into conversation or
games).
The symptoms must be present in before 7 age. Clear evidence must also
be present in the two or more setting (social, academic and occupationalfunctioning...).
SELF-ASSESSMENT 8.1.1
1. Discuss the following term: Inattention, hyperactivity and
impulsivity.
2. What are subtypes of ADHD learners?
3. Discuss the characteristics of children with ADHD.
4. Discuss the meaning of ADHD
5. What is the range of children from which are affected by ADHD?
8.1.2. Teaching and learning approaches for learners with ADHD
ACTIVITY 8.1.2
1. According to you, how can you teach learners with ADHD?
This is an important issue for many classroom teachers and parents who have
children with ADHD. Most people with ADHD experience significant difficulties
in school while attention and impulse control are prerequisites for success.
Most of children with ADHD respond to a structured and predictable learning
environment where rules and expectations are clearly stated and understood,
consequences are predetermined, reinforcement is delivered immediately.
Environment modifications alone are not the key to success. Educational
researches believe multimodal interventions, or concurrent treatment, are
generally more effective for individuals with ADHD than any one strategy.
Here are four main approaches that help to teach leaners with Attention Deficit
Hyperactivity Disorders
Instructional adaptations: Instructional adaptation coupled with
modification of the learning environment are powerful tools that can
help people to sustain attention while cultivating a climate that fosters
learning and encourage the child to control his/her behaviour. Teachers
should know individual differences and learning styles of children who
exhibit impairment that limit a major life activity like learning. Lerner
and Lowenthal (1993) provided some suggestions for teachers:
• Place the youngster in the least distracting location in the class (in
front of the class, away from doors, windows, air conditions, etc.
• Surround the students with good role models,
• Maintain a low pupil- teacher ratio whenever through the use of aids
and volunteers.
• Avoid unnecessary changes in schedules and monitor transitions
because the child with DAHD often has difficult copping with changes.
• Maintain eye contact with the student when giving verbal instructions
• Combine verbal and tactile cues with verbal instructions.
• Make a list that help the student organize tasks.
• Adapt break assignment into small chunks
• Ensure that the student has recorded homework assignment
• If the child has difficult staying in one place at school, alternate sitting
with standing and activities that requires moving around during the
day.
• Provide activities that requires active participation such as talking
through problems or acting out the steps.
• Use learning aids such as computers, calculators, tape records, and
programmed learning materials
• Provide student opportunities to demonstrate strengths at school.
Behavioural interventions:This approach helps to determine the
purpose of or function that a particular behaviour serves and how to
discourage or motivate. Once a good assessment is done the goal is
to construct interventions that modify the antecedent or triggering
behaviours and/or the consequences that are reinforcing and
maintaining the undesirable performance.
Home - school communication:It is essential for all pupils but
especially for those who have ADHD, it is an important ingredient
in promoting their success at school, the partnership must be
ongoing, reciprocal, mutually respect, and student centred. Parents
are encouraged to participate actively in their children’s plans and
collaborate with the multidisciplinary team. Teacher-parents may use
strategies work best for them.
Medication, and counselling represent some of available
intervention options for individual with ADHD. Some medication
like psychostimulants may play an important role in the treatment of
behaviours of ADHD. It is good to use this medication in conjunction
with educational and behavioural interventions. Teacher should
not recommend to parent that their son or daughter needs to be on
medication but only child’s health care professional can make such
a determination. Medication represent one part of the total package
and should not be seen as the panacea for ADHD. Instructional
and environmental accommodation should always be the first
intervention tactic used to assist pupils with Attention DeficitHyperactive Disorder,
SELF-ASSESSMENT 8.1.2
1. Describe one method that helps schools and parents to teach
learners with ADHD.
2. Discuss the instruction adaptational methods of teaching learners
with ADHD that should be used by teachers.
8.2. Learners with autism
8.2.1. Definition, causes and characteristics of Autism
ACTIVITY 8.2.1
Use books or other sources of information to answer the following
questions:
1. How do you understand Autism?
2. According to your mindset, what do you think are causes of
autism?
3. What will push you say that achild has autism?
Definition of Autism
Autism is a complex neurobiological disorder of development that lasts through
a person’s lifetime. Autism onset is between 0-5 years, and is three times more
likely to affect males than females. Autism Spectrum Disorder (ASD) affect
three area of deficiencies (also called triad of impairment) of development such
as communication development, social relatedness, and behaviours.
Brief introduction about Autism
People with autism have problems with social interactions and communication,
so they may have trouble of having conversation with others, they may not look
at in the eye. They may sometimes have behaviours that they have to or that
they do ever over and ever, like not being able to listen until their pencils are
lined up or saying the same sentences again and again. They may frap their
arms to tell you they are happy or they may hurt themselves to tell you they are
not.
The term Autism was first used by the Leo Kanner in 1943. Kanner described
eleven children with inability to relate themselves in ordinary way to people
and situations. Kanner used the term Autistic which means to “escape from
reality”, to describe the condition. Prior to Kanner’s work, autists people were
given many labels including: childhood schizophrenia, feebleminded, ideots,
imbeciles, mentally retarded.
Kanner believed that those children come to the world with innate to form the
usual, biological effective contact with people, just as other children come into
the world with the innate physical or intellectual handicap. He described those
children as having an excellent rote memory, delays in the acquisition of speech
and language (including pronouns reveal, echolalia, and extreme literalness
and obsessive desire for the maintenance of sameness. People use to confuse
Schizophrenia and Autism. Schizophrenia is a mental illness characterized by
strange speech and abnormal behaviour and a decreased ability to understand
reality.
Kanner (1943) differentiated both disorders in three areas:
• An extreme aloneness from the beginning of the life
• An attachment to objects
• Powerful desire for aloneness and sameness
For Kanner, Autism is inability to relate to themselves, it starts as extreme
autistic aloneness, whenever possible, disregards, ignores, shuts out at anything
that comes to the child from outside.
According to Diagnostic and Manual of Mental Disorders of American Psychiatric
Association (2000), there are five specific autism diagnoses under pervasive
developmental disorders (PDD) such as:
Autistic disorder: it is a disorder which is characterized by deficit
in reciprocal social communication, deficits in communication and
language, restricted and repetitive behaviours and interests.
Asperger disorders: it is known as milder form of autism. The major
characteristic of this disorders is a lack of interest in social relationships
or difficulties in forming a relationship with others. According to
Ozonoff and Rogers, 2003, The language is not impaired and there is no
impairment in cognitive functions
Rett disorder: it is a condition found only in girls. Children who receive
diagnosis usually show typical growth up to 5 or 6 months of age. They
begin to use their interest in other over time.
Childhood disintegrative disorders: it continues a period of typical
growth in the child followed by loss of developmental skills, which
eventually ends in severe cognitive deficits and others abilities.
Pervasive not otherwise specified
Pervasive Developmental Disorder (PDD) refers to a group of
disorders which are characterized by delays in the development of
socialization and communication skills.
Causes of Autism
We know that there is no one cause of autism. Researchers believe that genetic
and non-biological factors may influence the risk of having autism.
Genetic factors:
Researchers believe that autism tends to run in families. Changes in certain
genes increase the risk that a child will develop autism. If a parent carries one
or more of these gene changes, they may get passed to a child (even if the parent
does not have autism). Other times, these genetic changes arise spontaneously
in an early embryo or the sperm and/or egg that combine to create the embryo.
Current knowledge regarding ASD mostly comes from family and twins’ studies.
Environmental risk factors
Researchers believe that certain environmental influences may further
increase or reduce autism risk in people who are genetically predisposed to
the disorder. Importantly, the increase or decrease in risk appears to be small
for any one of these risk factors. Exposure to environmental toxins, such as
maternal exposure to memory during pregnancy, excessive use of antibiotics in
children, household and environmental pesticides.
The characteristics of Autist
Autism is looked through three criteria including impairment in communication,
impairment in the use of non-verbal behaviours, restricted and stereotyped
patterns of behaviours, interests and activities. The abnormal functioning in at
least one of social interaction and language, with onset prior to age 3 can define
autism but not limited to that.
a. Qualitative impairment in social interaction, as manifested by at least two
of the following:
• Marked impairment in the use of multiple nonverbal behaviours such
as eye to eye gaze, facial expression, body postures and gestures to
regulate social interactions.
• Failure to develop peer relationships appropriate to developmental
level.
• Lack of spontaneous seeking to share enjoyment, interests, or
achievement with other people (lack of showing, bringing, or pointing
out objects of interest.
• Lack of social or emotional reciprocity.
b. Qualitative impairment in communication as manifested by at least one
of the following:
• Delay or total lack of the development of spoken language (not
accompanied by not to attempt to compensate through alternative
modes of communication such as gestures or mime)
• Individual with adequate speech, married impairment in the ability to
initiate or sustain a conversation with others
• Stereotyped and repetitive use of language or idiosyncratic language.
• Lack of varied, spontaneous make-believed play or social imitative play
appropriate to developmental level.
c. Restrictive repetitive and stereotyped patterns of interests, and activities
as manifested by at least one of the following:
• Encompassing preoccupation with one or more stereotyped and
restricted patterns of interest that is abnormal either in intensity of
focus.
• Apparently inflexible adherence to specific, non-functional routines or
rituals.
• Stereotyped and repetitive motor mannerism hands of fingers flappingor twisting, or complex whole-body movement).
SELF-ASSESSMENT 8.2.1
1. Define the word autism
2. Discuss three angles through which autism is seen.
3. Describe characteristics of learners with autism.
4. Provides some labels given to autistic people according to
Kanner’s work
5. For DSM IV there are four types of autism, discuss.
8.2.2. Teaching strategies for learners with Autism
ACTIVITY 8.2.2
1. From your own thought, what are some of the services that
should be given to learners with autism to help them in everyday
lives?
Early educational intervention makes a positive difference in the life of
an individual with autism. Early intervention services typically include a
structured educational and behavioural modification strategies with related
and specialized services. Those related and specialized services may include:
• Assistive technology and services
• School nursing services
• Parent counselling and training
• Nutrition services
• Artistic and cultural programs-art, music, and dance therapy
• Occupational therapy
• Speech and language therapy
Early interventions begin with the development of an individualized family
service plan (is a plan for special services for young children with developmental
delays, IFSP), which typically addresses needs in the areas of social skills,
functional skills (dressing, toilet training, self-feeding), communication,
and behaviour modification. No one program is applicable to all children
with Autism, the strength and needs of each child must be considered in thedevelopment of specific educational plan.
Techniques of a structured educational approach
Some of techniques of a structured educational approach include but not
limited to:
• Use Task Analysis: very specific, tasks in sequential order.
• Always keep your language simple and concrete.
• Teach specific social rules/skills, such as turn-taking and social
distance.
• Give fewer choices and avoid using sarcasm
• Avoid using idioms. “Put your thinking caps on”, “Open your ears”
and “Zipper your lips” will leave a learner completely mystified and
wondering how to do that.
• Give very clear choices and try not to leave choices open ended.
• Repeat instructions and checking understanding. Using short sentences
to ensure clarity of instructions.
• Providing a very clear structure and a set daily routine including time
for play.
• Providing warning of any impending change of routine, or switch ofactivity. Etc…
According to Bayat (2012) adaptations and modification of the environment and curriculum
for autist learners should be based on their sensory and behavioural needs.
Early childhood special education and inclusive classrooms will benefit
from arranging the environment based on the following guidelines:
Use of visuals in the classroom: these are the objects and pictures
that can be used in order to enhance communication with learner
with autism. Pictures are symbols that represent specific objects,
actions, concepts. Visual has become important element of a
successful interventions for children with autism in Early Childhood
Special Education and inclusive classrooms. Picture exchange
communication system is an effective method of working with
autism that enables them to communicate with peers and adults.
Specific physical arrangement of the classroom and home: The
environment should [provide messages in the regard where things
are and what to be done. Visual should be used to labels, desks,
drawers, and materials.
Cozy corner and sensory-oriented activities to support selfregulation:
Children with autism should have a cozy corner, contained
refuge that has a calming effect for children. Pillows beanbags, and
blankets should be available for children to calm down when they
are having tantrum as a result of a sensory overload.
Providing daily and weekly schedules: Children with Autism benefit
from predictable routine. In daily schedule the adults give clear
messages to children about plan of a day and what exactly willhappen through the day.
SELF-ASSESSMENT 8.2.2
1. What are some specialized services available for children with
autism?
2. Why should visuals be used in a classroom for learners with
autism?
SKILLS LAB
1. Visit a special school and identify two learners, one is suspected
to have Attention Deficit Hyperactivity Disorder and another one
suspected to have autism. Spend four hours with both children.
On three pages, describe the characteristics of each child and
suggest strategies you could use to teach both leaners and suggest
some recommendations.
END OF UNIT ASSESSMENT
1. Mention four main approaches teachers can use to teach learners
with ADHD.
2. Discuss ADHD subtypes and its characteristics
3. Discuss the interventional approaches for a learner with ADHD
4. What are the characteristics of an Autist? child ?
5. What is the role of early intervention for leaners with autism?
6. Discuss three areas which characterize learners with autism?
7. Discuss the techniques of structured educational approaches
which are used to teach learners with Autism?8. What are the guidelines for supporting the learners with autism?
UNIT 9 GIFTED AND TALENTED LEARNERS
Key Unit Competence: Identify the characteristics and educational needs
of Gifted and talented Learners
INTRODUCTORY ACTIVITY
Case study: Deborah
Deborah is a 9-year-old girl, intense, inquisitive, energetic, and imaginative
P3 learner. When you talk to her you mark her potential for performing many
things in unexpected way. She excels in school and enjoys finding solutions
to problems independently. She loves science and enjoys researching topics
and abstract tasks, especially in Sciences and Mathematics. She dislikes
routine mathematics and may make careless computation errors, but she is
always above average in her standardized mathematics tests. Deborah has
few close friends though generally tolerated by her peers.
Tasks:
1. In small group, discuss the learning problems Deborah has.
9.1. Definition, causes and characteristics of gifted and
talented learners
ACTIVITY 9.1
1. What is the difference between a gifted learner and a talented
learner?
2. In your opinion, what are the key promotors of a gifted or talented
behaviour?
3. Suppose that you have probably heard about a gifted/talented
child, what do you think that differentiates them from others?
4. In your opinion, how can you describe a gifted or talented child?
Definition of gifted and talented learners
According to Karnes and Suzanne (1993), gifted and talented children and youth
are those with outstanding talents and who perform or show their potential for
performing at remarkably high levels of accomplishment when compared with
others of their age, experience or environment.
They exhibit high performance capability in intellectual, creative and/or artistic
areas, possess an unusual leadership capacity or excel in specific academic
fields. They require services or activities not ordinarily provided by the schools.
Here are some differences for those Gifted and Talented learners:
• Gifted learners are those who have superior general ability in academic
performance.
• Genius learners excel in almost all academic domains and with less
effort.
• Talented learners are those who show signs of special aptitude orability in specific areas of the arts, sciences, business, etc.
Causes of giftedness and talented ness
Researchers indicate that genetic factors are known to contribute significantly
to behavioural development, including intelligence and gifted performance. But
also, environmental factors, families, schools and communities are also known
to influence the development of giftedness.
Basing on this argument, giftedness is therefore the result of combined
biological and environmental influences that is therefore the result of combined
biological and environment influences that is nature and nurture. They further
suggest that one’s collection of genes sets limits of performance; the actualperformance within those limits is determined by environment factors.
Classification of learners who are gifted and talented
Children who are gifted and talented are a heterogeneous group. They are
classified into six categories such as:
• General intellectual ability: Learners have excellent memories and ask
many questions. They are able to grasp concepts, generalize, analyse or
synthesize new ideas.
• Specific academic aptitude: Learners with specific aptitude are those
who are high academic achievers, study purposefully and achieve high
academic grades in their work.
• Creative and productive thinking: Creative and productive thinkers
are those learners who develop or come with new ideas, projects and
products (they may involve all spheres like science, medicine, politics
or leadership).
• Leadership ability: Learners with leadership ability are those who
typically display:
a. Well-developed social skills
b. Empathy
c. Ability to motivate others
d. Ability to keep others united
e. Effective communication skills
• Visual and performing arts: learners who are gifted in visual and
performing arts are good in performances that please the eyes and the
ears of their audience (include different arts like dancers, musicians,
actors…)
• Psychomotor ability: Psychomotor means “high coordination of the
mind and muscle for super performance” it is closely related to visual
and performing arts since performance are required in both.
Characteristics of gifted, genius and talented learners
• Learn new material faster, and at an earlier age, than age peers;
• Always remember what has been learned without making revision;
• Is able to deal with concepts that are too complex and abstract for age
peers;
• Has a passionate interest in one or more topics, and would spend all
available time learning more about it if possible;
• Does not need to look at the teacher to hear what is being said;
• Can operate on multiple brain channels simultaneously and process
more than one task at a time.
• Fluent and flexible thinking• Excellent thinking and reasoning
SELF-ASSESSMENT 9.1
1. Discuss three characteristics of gifted and talented learners
2. With clear examples, discuss six categories of gifted and talented
learners
3. What are some of the environmental factors known to influence
the development of giftedness?
4. How do Karnes and Suzanne (1993) define a gift or talented
learner?
9.2. Effect and teaching approaches of gifted and talented
learners
ACTIVITY 9.2
1. Discuss what you think are the best ways of teaching gifted and
talented learners.
Effects of a gifted and talented learners
Despite general being well adjusted, they experience some emotional and
adjustment problems. They experience intra-psychic conflicts in classrooms
because although they would like to excel academically, at the same time they
are afraid of outperforming their mediocre or less performing classmates since
this would lead to their rejection.
Learners who are gifted and talented often experience conflicts with their
teachers and parents as a result of persistent inquisitiveness which poses a
challenge to those who interact with them. In addition, their independence of
mind, desires to pursue projects of their own, demand for stimulating materials,
books pose a challenge to both parents and teachers.
Strategies of accommodating gifted and talented learners
Learners who are gifted and talented are considered to require special education
in the form of: differentiated teaching strategies, curriculum and services.
Learners who are gifted and talented are just like any others. They have
basic needs like other learners and the teacher needs to be tolerant, loving,
understanding, and flexible. Also, the teacher needs to remember that those
learners are creative, competent, have broad range of interests and skills, and
ready to learn. To help the child who is gifted and talented, the teacher therefore
needs to:
• Recognize and accept the learner’s special abilities
• Encourage the child to explore his fields of interests
• Help the learner to develop or enrich his social confidence
• Avoid imposing expectations and demands that are beyond the
learner’s level of ability
• Avoid having negative attitudes towards the learner
• Positively reinforce learners with SEN.
School management of the gifted and talented involves the provision of an
educational programs that encourages:
Use of special classes: Gifted children are removed from the regular
classroom for special instruction, so they benefit from classes which
are like resources rooms.
Ability grouping: Can be defined as the practice of placing leaners
in groups according to their level of cognitive ability. Children who
are good achievers are put together in one group for the purpose
of providing differentiated learning experiences. Benefit of ability
grouping include learning activities can be accelerated or enriched,
it reduces boredom and frustration, develops creative and thinking
skills among the learners. But also, this technic may lead to elitism in
the class where learners who are gifted and talented may feel superior
to others and this may de-motivate the weak ones.
Acceleration: It is the practice of offering the standard curriculum
to children who are gifted and talented at younger age than usual
or covering the content in less time than as normally prescribed.
Some forms of accelerations include early admission to school, grade
skipping, telescoped programs.
Enrichment: It refers to study, experience or activity which is above
and beyond the normal curriculum followed by other children of the
same age. The learners are given the opportunities to explore the
subjects in-depth.
Curriculum diversification: Considering the curriculum for these
group of learners, one should consider the following: chronological
age of the child, the current class of the child, the child’s mental age.
Guiding and counselling: Gifted and talented learners need
special attention to be able to function normally in the society.
Some supports are very crucial such as: intra and inter-personal
relations, development of communication skills such as turn taking in
conversations and dialogues, development of self-care skills.
Acceleration, accommodation, enrichment and modification are qualities of
differentiated instructions of which should be used for the education for all
exceptional children. The assessment guides the Individualized Education Plan
(IEP). Specific curricula activities and strategies are highly recommended forall learner who are gifted.
SELF-ASSESSMENT 9.2
1. What do you understand by the terms?
a. Acceleration b. Ability grouping
2. Discuss the effect of being genius or talented in the classroom
SKILLS LAB
1. Visit a primary school and identify a child who is expected to be
gifted and talented. Take time and spend three hours with the
child. Write down all the characteristics of the child and suggest
strategies you could use to support that child improve her/ his
studies.
END OF UNIT ASSESSMENT
1. Who are the children referred to as gifted and talented?
2. Discuss the different traits of gifted and talents learners
3. What are the teachers’attitudes towards the gifted and talented
learners ?
4. What strategies should schools use for proper management ofgifted and talented learners
UNIT 10 LEARNERS WITH EMOTIONAL AND BEHAVIOURAL DISORDERS (EBD)
Key Unit Competence: Explain the characteristics and Special Educational
Needs of learners with Emotional and Behavioural
Disorders (EBD) and use appropriate teaching/
learning approaches
INTRODUCTORY ACTIVITY
MUTETE is a young girl of seven years old, she has 3 siblings. She was
born in Rubavu district but at 4 years of age she become an orphan of both
parents due to an accident. After the death of her parents she was taken to
start school out her uncle’s home. But as the time goes by it was not easy
for MUTETE to study and stay in class like other learners because she had
fear of unexpected things and often cried in class, failed to obey teacher’s
instructions, and feeling distressed apparently. During the end of year
exams, MUTETE shouted and run out of the examination room. The Head
teacher and her elder brother decided to take her to the psychologist for
assessment. The assessment was well done and she was diagnosed with EBD.
With the advice from the psychologist, the family made a plan in order to
help MUTETE improve her situation slowly. MUTETE now attends a regular
school and succeeds in class and attends regularly as other learners.
Questions:
In your groups:
1. According to the case study, what was the source of MUTETE’s
problems
2. Discuss MUTETE’s problem in this case study?3. What intervention plan was made for MUTETE?
10.1. Definition and causes of EBD
ACTIVITY 10.1
Using your resources:
1. How can you explain Emotional and Behavioural Disorder (EBD)?
Definition of EBD
Emotional and Behavioural disorder (EBD) is a disability that is characterized
by behavioural or emotional responses in school programmes different from
appropriate age, culture, or ethnic norms that affect education performance,
including academic, social, vocational and personal skills.
EBD is a broad term used commonly in educational settings, to group a range
of more specific difficulties experienced by learners and adolescents.
Both the general definitions and the concrete diagnosis of EBD may be
controversial, as the observed behaviour may depend on many factors.
Behavioural disorders, also known as conduct disorders, are one of the most
common forms of psychopathology among learners and young adults, and
are the most frequently cited reason for referral to mental health services. In
Rwanda, these services are available.
The people with Emotional and Behavioural Disorder (EBD) are described
using different terms including but not limited to: emotionally disturbed,
behaviourally disordered, emotionally conflicted, socially handicapped,
personally impaired, socially impaired, and many others.
There are four dimensions of EBD which are common to each of the Emotion
and Behaviour disorders:
• The frequency at which the behaviour occurs
• The frequency of the behaviours
• The duration of the behaviours
• Age-appropriateness of the behaviours.
Causes of Emotional and Behavioural Disorders
Even though there no known and exact causes of Emotional and Behavioural
Disorders. Researchers believe that biological, developmental and
environmental factors with some preventive measures are considered as
leading factors of EBD in young children.
Biological causes
Chemical imbalances in the brain and body can make managing emotions a
challenge. Here are some examples of biological condition that may lead to EBD:
• Prenatal exposure to drugs or alcohol
• A physical illness or disability
• An undernourished or malnourished lifestyle
• Brain damage
• Hereditary factors
Environmental factors
This is the conditions a person’s daily life in the community. There are so many
element that have been correlated to emotional disturbance including family
income below the poverty level, stress in the family unit because of divorce
or some other emotional upset; inconsistent rules or expectations as well as
inconsistent and unhealthy discipline, parents have a lack of interest or concern
for the teen, which leads to a lack of supervision or neglect; family members
are poor role models, perhaps violent, perhaps getting in trouble with the law;
parents or siblings physically abuse the teen; there is an overall low rate of
positive interactions and high rate of negative interactions in the family; the
family has a poor attitude toward school or education.
Developmental factors
Development refers to the lifelong process of changing and maturing. Every
stage of life has its tasks that must be completed successfully for mental health
and life satisfaction. When a child’s development is disrupted and problematic,
there can be negative consequences for mental health and cognitive growth.
There is no single known factor that may cause Emotional Behavioural disorder
Here are some examples of developmental causes:
• Attachment problem: it may be either lack of positive attachment to
the primary caregiver or over attachment leading to clinginess and
difficulties separating from the caregiver
• A failure to develop trust during infancy and early toddlerhood,
resulting in fear and mistrust
• Inability to experience some autonomy and instead internalize a sense
of shame for exploring
• Opposed attempts to show initiative and instead made to feel guilty for
wanting to try new things
• Failure to experience a sense of competence, which leads to feelings ofinferiority, during the elementary years.
SELF-ASSESSMENT 10.1
1. Explain what is by EBD?
2. What is the most known disorder of EBD?
3. Explain environmental factors of EBD?
4. What do you understand by developmental factors of EBD?
10.2. Classifications and characteristics of learners with
EBD
ACTIVITY 10.2
Using your resources:
1. Hearing the meaning of Emotional and Behavioural Disorder, it is
a broad term, what do you think about it?
2. Describe some criteria that may help to confirm EBD?
Emotional Behavioural Disorder is classified into three groups:
• Conduct disorders
• Emotional disorders
• Personality disorders
Conduct disorder
The diagnosis of conduct disorder is based on antisocial behaviour, and it
says little about the child’s inner life motives, and disabilities. The disorder
is classified by: aggressive and overt versus convert.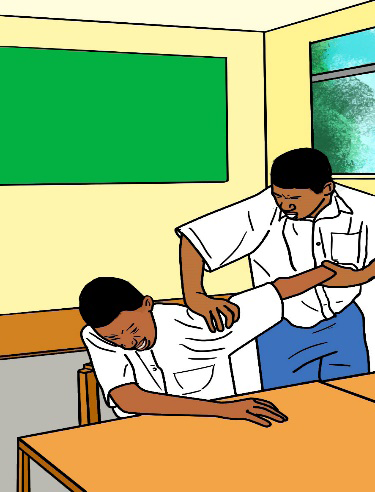
Examples of undesirable behaviours exhibited are anger, attention seeking and
boisterousness bossiness, disobedience, impatience, irresponsibility, jealousy
and temper tantrums.
Emotional disturbances
It is a condition exhibiting one or more of the following characteristics over
a long period of time and to a marked degree that adversely affects a child’s
educational performance:
• Inability to learn that cannot be explained by intellectual, sensory or
health factors;
• Inability to build or maintain satisfactory interpersonal relationships
with peers and teachers
• Inappropriate types of behaviour or feelings under normal
circumstances
• A general pervasive mood of unhappiness or depression
• A tendency to develop physical symptoms or fears associated with
personal or school problems.Characteristics of Emotionally Disturbed Child
Personality disorders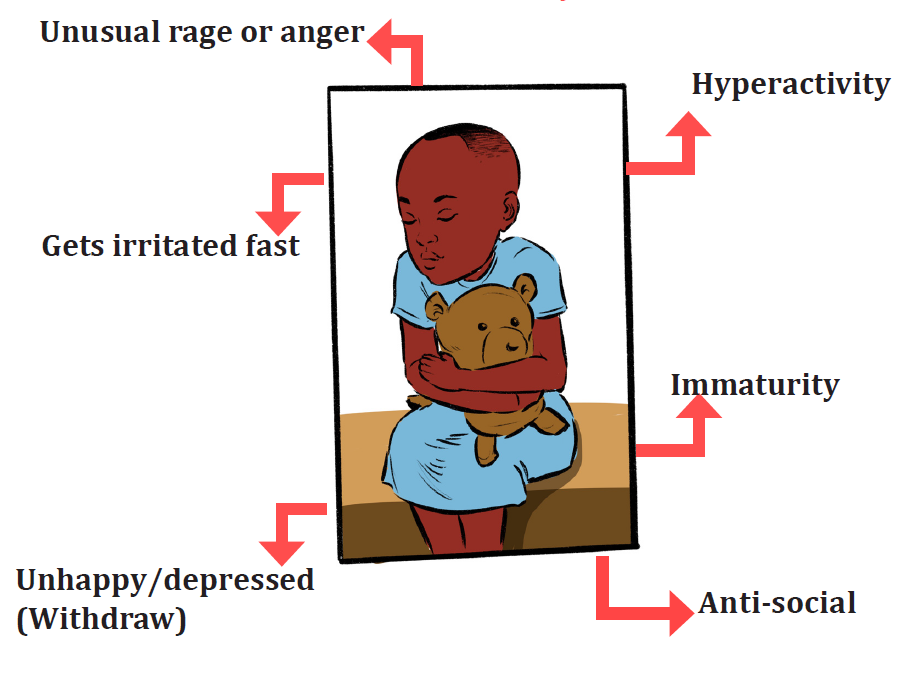
Personality disorder refers to a disorder enduring pattern of inner experience
and behaviour that deviates markedly from the expectations of the individual’s
culture, that is pervasive and flexible, has an onset in adolescent or early
adulthood, is stable over time and lead to distress of impairment.
Characteristic of learner with EBD
Learners with emotional or behavioural disorders are characterized primary
by behaviour that falls significantly beyond the norms of their cultural and age
group on two dimensions:
• Externalization and
• Internalizing.
Both patterns of abnormal behaviors have adverse effects on children’s
academic achievement and social relationship.
Externalizing behaviors are as under-controlled disorders which
are characterized by aggressiveness, temper tantrums, acting out and
noncompliant behaviors.
Internalizing behaviors sometimes referred to as “over controlled
disorders “which are characterized by social withdrawal, depression
and anxiety. Learners with internalization are unlikely to be identified
by the teachers and families because they do not create the chaos that
are commonly associated with learners with externalizing behaviors.
Learners with EBD portray:
• Impulsivity and, hyperactivity, or “out of control” behaviours
• Episodes of extreme irritability, anger and outbursts.
• Moods that change quickly and seemingly without reason
• Poor grades at school due to lack of work completion and behavioural
problems
• Sadness, withdrawal, decreased energy level.
• Inflexibility and low tolerance for frustration.
• Loneliness
• Low attention span
• Inability to concentrate
SELF-ASSESSMENT 10.2
1. Discuss the classification of Emotional and Behavioural disorder
2. Differentiate conduct disorder from Personality disorders and
emotional disorders.
10.3. Teaching approaches for learners with Emotional
and Behavioural Disorders
ACTIVITY 10.3
1. After having some information about EBD, how can you
educationally help learners who have Emotional and Behavioural
disorder?
The following interventional measures have been known to manage EBD
learners:
• Implementation of behaviour modification strategies
• Effective behaviour management procedures put in place,
• Appropriate routines for classroom procedures
• Effective instructional delivery and a variety of relevant instructional
activities.
• Clear hierarchical reprimand or consequence system. For example,
non-verbal warning, verbal warning, parent conference, suspension
and referral.
The management of learners with EBD require a good and flexible teacher.
There are some measures that help teachers to manage learners with EBD.
Those measures are classified into three categories:
a. Physical environment interventions: Positive behavioural support
include providing effective academic content and instructional to students
with emotional disorders.
Researchers show that student EBD can benefit from certain teaching strategies.
Five of them include effective instructional cycles, teaching mnemonics,
self-monitoring strategies, curriculum-based measurement, and contentenhancements,The components of effective instructional cycle include:
• Beginning each lesson with a statement of goals, with a review of
previous, prerequisite learning
• Presenting new material in small steps, with students practice following
each step
• Providing active and sufficient practice for all students.
• Asking questions, checking frequently for student understanding and
obtaining responses from all students.
• Providing systematic feedback and corrections to students.
• Providing explicit instructions and practice for seatwork activities and
actively monitoring students during those activities.
• Continuing to provide practice until students are independent and
confident.
b. Academic and instructional interventions
In this strategies PBS (Positive Behavioural Support) is the most used and very
crucial. Positive behavioural support is the application of positive behaviour
interventions and systems to achieve socially important behaviour changes.
It can be used in preschool setting. Working with parents to provide positive
support at home can directly foster school readiness and behavioural health in
young children.
These strategies can be used:
School wide positive behaviour support: it can be used in inclusive
school to manage the children with disabilities’ behaviours. The
school wide positive behaviour has three components:
• Universal support,
• Group support
• Individual support
Class wide strategy promote social competence in order to create
a positive classroom climate there are some strategies to be adapted
in inclusive and special education.
• Use close supervision and monitoring of all children at all times
by scanning, moving frequently, initiating
• Establish and teach classroom rules, which detail expected
behaviours at the beginning of the year, and systematically
teach the rules to children throughout the year.
• Provide opportunities for children to respond by questioning,
providing visual and verbs prompts.
• Increase use of contingent and specific praise by frequently
acknowledging the children’s appropriate behaviour in a
descriptive way
• Provide feedback and help children learn the correct responses
in a timely fashion.
c. Behavioural and cognitive-behavioural interventions
It begins with assessment of child’s behaviour. Functional Behavioural
assessment (FBA) is the process that determines why a child engages a specific
behaviour and how the child’s behaviour relates to his or her environment. It
gathers data from multiple sources to identify the antecedent and consequence
event that predict and maintain problem behaviours.
Functional Behavioural assessment (FBA)
• Analysis of a child’s behaviour
• The condition that might contribute to the child’s behaviours
• Forming the hypothesis regarding the reason for behaviours
• Identifying consequences that might contribute to the prevention, orreoccurrence of, the behaviour in future.
SELF-ASSESSMENT 10.3
1. What is the role of Functional Behavioral Assessment?
2. Discuss the school wide positive behavior
SKILLS LAB
1. Visit a secondary school and identify a student who is suspected
to have an emotional behavioral disorder. Spend two hours with
the student. Write down all the characteristics of the child and
suggest strategies to be used to help the child improve her/ his
studies and provide some recommendations (in schools and
teacher, parents).
END OF UNIT ASSESSMENT
1. Explain the classification of EBD
2. Discuss the characteristic of learners with EBD
3. What are three interventional approaches for a learner withEBD?
UNIT 11 CHILDREN WHO ARE EDUCATIONALLY VULNERABLE
Key Unit Competence: Identify all other categories of learners with
different special educational needs, specify
their characteristics and impact on learning and
teaching
INTRODUCTORY ACTIVITY
Case study: Muhire
Muhire is a 11 years old boy. Since he was born, he did not know his father,
his mother died of breast cancer when he was 10 years. After the death of
his mother Muhire was taken to be cared for by his elder brother who is his
only sibling. Muhire’s brother earned an insufficient salary to satisfy all their
needs even though Muhire was attending a fee free Primary school, but there
were other needs that his brother was not able to satisfy. At 13 years Muhire
was enrolled into a secondary school. As Muhire had passion for school he
walked 12 km to school without school fees to pay but when he arrived at the
school, he was sent back home. Muhire’s sister in law (wife to his brother)
was unhappy to see Muhire coming to request from them money for school
fees and other school materials and not ready to support him. Muhire stayed
home for 6 months. Later a brilliant idea come to his mind, he went to nearest
sector office to raise his problems and leaders of the sector promised him to
pay for his secondary and university studies as is the government policy to
support vulnerable. Muhire went back to school and is now at his last year
as a medical student.
Tasks:
In groups
1. What problems did Muhire encounter after his primary education?2. How was Muhire’s problem solved?
11.1. Definition, categories and characteristics of children who
are educationally vulnerable
ACTIVITY 11.1
1. Who are children living under difficult circumstances?
2. According to you, what are some of the problems that may hinder
children from attending school?
Children are said to be vulnerable when their basic needs for food, shelter,
education, medical care, or protection and security are not met. This has
different factors including political, socio-cultural and economic and health
difficulties. Such children are at great risk of suffering malnutrition, disease
and possible death. Unless their own situation changes their conditions of gross
disadvantages will extend to their own children who may suffer even greater
misery and suffering.
Categories of children who are educationally vulnerable
Children living under especially difficult circumstances are classified into
twelves categories.
a. Street children: They are children who live or spend significant amount
of time on the streets of urban area to fend for themselves and/or their
families. Also include children who are inadequately protected, supervised
and cared for by responsible adults. There two main categories of street
children:
Children of streets: children of the streets are boys and girls who see
the street as their home. They may still have their families ties but
seek shelter, food and a sense of family among their companions on
the streets or they may have completely broken ties with their families
and literally live on streets. Often, they have been abandoned by their
parents, are orphans or runaways from neglected or abusive families.
Children on the streets: are those who still have family connections.
They live at home, often in more than shacks, sometimes even attend
school, but are sent to street by parents or go of their own accord tosupplement the family income.
Street children smoking cegarette
b. Abused and neglected children:
child abuse is any act or intention
to treat children badly by directly
or indirectly hurting them. It can
be physical and or psychological
violence. On the hand, child neglect
is rendering no care to children by
parents or caregivers. It is also a
failure to provide for the daily needs,
hence affecting the children’s social,
emotional and psychological status.
Other form of abuse and neglected
include: lack of affection, systematic
scolding and withdraw from
the school. Forced marriages may also interfere with their education. S/he
may be reluctant to say something because s/he may want to protect that
person or is afraid of what they will do if s/he speaks up. Sexually abused
children can be defined as those who have had sexual contacts or interactionsbetween them and other or more knowledgeable people.
c. Children who are traumatized:
a traumatic event involves a single
experience, or an enduring or repeating
event that may completely overwhelm
a child’s ability to cope or integrate the
ideas and emotions involved with that
experience.
d. Child mothers: Young girls who become pregnant and give birth at early
age hence assume the role of being a mother.
e. Child soldiers: A child associated with an armed force or armed group
refers to any person below 18 years of age who is, or who has been, recruited
or used by an armed force or armed group in any capacity, including but
not limited to children, boys and girls, used as fighters, cooks, porters,
spies or for sexual purposes. It does not refer to child who is taking, or has
taken, a direct in hostilities. Their enormous tasks undertaken by thesechildren affects theirs learning and emotional wellbeing.

Child soldiers
f. Children Heading Families:
Children who take up responsibilities
of parents as result of incapacitation or even death of their
parents. This could be due to wars, tribal clashes, displacementand others natural calamities.
g. Child labourer: It refers to work that is mentally, physically, socially or
morally dangerous and harmful to children, and interferes with their
schooling by depriving them of opportunities to attend the school. Child
labour is often defined as work that deprives children of their childhood,
their potentials and their dignity, and that is harmful to physical and mental
development. Term “child labour” is also referred to as employment of
children below adult age, which is considered illegal by law and custom.
But the stipulated age varies from country to country and government tomovement.
h. Children who are refugees and displaced: Those are children who
forces to leave their homes, often travelling the long distance to escape
enemy, fire and become the most vulnerable victims of violence, disease,
malnutrition and death.
i. Homeless and unaccompanied children: Children who are not in the
physical custody of a parent or guardian.
j. Orphaned children: Children who are bereaved for both mother and
father hence exposed to many challenges such as lack of basic needs, that is
food, shelter, and clothing. The death of both parents leads to deprivation
and feeling of insecurity. Their learning and development will be affected
since they have to fend themselves most of the time.
k. Children affected and infected by HIV/AIDS: Are children who are
infected and those from families affected by HIV/AIDS may be stigmatized
and suffer discrimination. Loosing on of their parents of family members
affect their emotions, physical and education. The lives of children who
may not have HIV themselves are affected when family members have HIV
and AIDS. Families face increased poverty and stress when adults are too
sick to continue with paid employment or farm their land. Mothers who
are ill find it difficult to take care for young children and young children
may end up caring for parents or young siblings.
l. Children living in family conflicts.
Characteristics of children who are educationally vulnerable
The characteristics are displayed in four ways:
• Physical characteristics:
• Cognitive characteristics
• Behavioural characteristics
• Socio-emotional characteristics
a. Physical characteristics
Those are physical event that may cause a child not to attend the class as
expected including: fractures, bruiser and welts, burns and scalds, head or
brain injuries, human bite marks.
b. Cognitive characteristics
They are drive and or mind-set that push a leaner to have a repeated absent in
school like Development delays in cognitive abilities, distractibility and poor
attention span, unrealistic expectation in life.
c. Behavioural characteristics
In behavioural characteristics include drug and alcohol misuse, abusive
behaviour and language, poor memory and concentration, suicidal behavioural,
truancy and running away from the school, etc.
d. Socio-emotional characteristics
Some characteristics are:self-harming behaviours such as head-banging,
persistent rocking, disturbed toileting behaviours, excessive hunger drives,
short attention span, excessive hunger drive, bizarre eating behaviours,
disrupted sleep behaviours.
SELF-ASSESSMENT 11.1
1. What are some of the factors that make children vulnerable and
what are the risks?
2. Discuss characteristics of children who are educationally
vulnerable?
3. Explain some examples of categories of children who are
educationally vulnerable.
11.2. Intervention strategies for children who are educationally
vulnerable
ACTIVITY 11.2
1. Suppose that you have children who are educationally vulnerable
in your class, how can you help them out of their vulnerability?
Children with different problems have the right to protection and participation
like all other children. Learners who are educationally vulnerable should be
helped in different ways at school by teachers or any others.
It is important for a teacher and others who work with those learners to bear
in mind that all children may not present the same challenges due to their
individual experiences.
Measures that teachers can keep in when taking care of venerable children:
• Exercise caution in assigning homework
• Be conscious of educational gaps of learners
• Be on the alert for mental health problems;
• Be attentive to other matters.
• Be vigilant of children who are streetwise or manipulative.
The way children are helped will depend on different factors including families,
parenting styles, environmental, literacy levels and economic status of the
parents among other.
The interventions and support are categorized into the following:
a. Crisis interventions: This is to offer short term or immediate support to
someone who experience the event that produces mental, physical and
emotional difficulties. Crisis happens to everyone and intervention may
take many forms. They are aimed at helping people to individually cope
with crisis in ways that it reduces the negative psychological, physical,
physiological and behavioural effects of trauma on that person and his/
her environment.
b. Improved family interventions: Family pay a very crucial role in a child’s
development and growth. A child learns much from a good family like
social role through interaction. This foster a sense of psychological and
emotional security necessary for the child’s growth and development.
Families are encouraged to create a conductive family environment for
health interactions.
c. Mobilization of the community: Various professionals, CSOs (civil
society organization) and NGO are mobilized to contribute in different
ways for example donations, trainings through workshops and seminars,
availability of communication and transport)
d. Government policy and interventions: The government has the
obligation to organize and have relevant policies in place to support
vulnerable children.
SELF-ASSESSMENT 11.2
1. Differentiate the Improved family intervention from crisis
intervention
SKILLS LAB
In your home community, identify a child who does not attend school.
Spend around two hours with the child. On two pages, discuss her/
his condition and locate the child in categories of children who are
educationally vulnerable, find out the effect of the current situation and
then propose the educational interventions for this child
END OF UNIT ASSESSMENT
a. Who is a vulnerable child ?
b. What some of the characteristics of learners who are educationally
vanerable in the following areas.
• Physical
• Cognitive
• Behavioural
• Socio-emotional
c. Discuss strategies to help children who are educationally
vulnerable.
d. Identify the categories of learners who are educationally
vulnerable
e. What can teachers do to help children who are educationally
vulnerable ?UNIT 12 INTERMEDIATE RWANDAN SIGN LANGUAGE AND DEAF EDUCATION
Key Unit Competence: Interpret and use intermediate Rwandan sign
language
INTRODUCTORY ACTIVITY
Read the following text and answer the questions that follow:
Ishimwe became deaf at the age of 5 as a result of meningitis. She could
not communicate using Sign Language because her vocabulary was very
limited. She could not express herself and it was extremely difficult for
her to survive as she had to live with her siblings, parents and peers who
had no knowledge in Sign Language. With the help of her teacher who was
trained in Sign Language, Ishimwe started to learn simple vocabularies. She
can now ask for food, greet people, ask for help, count, etc. with confidence.
As she progresses in school, she become fluent in Sign Language. She can
now construct meaningful sentences using Sign Language grammar. Though
Sign Language grammar is different from English grammar, her peers and
teachers are able to understand what she says and write. Ishimwe is a smart
learner, bright and now ready to sit for national exam. He is confident that he
will pass the exam with excellency.
Questions:
1. Which areas that Ishimwe encountered difficulties after she became
deaf?
2. Why do you think Sign Language grammar is different from Englishgrammar?
12.1. Sign Language vocabularies
ACTIVITY 12.1
Sign Language vocabularies
1. How would you sign number “ 1 , 2,3” in Sign Language?
2. How do you think we should sign the following words: Farther,
mother, baby?
3. How would you sign” Good Morning in Sign Language?
4. If you want food, how would you sign” Cassava, chicken in Sign
Language?
5. If you are attacked by an animal, how would you sign: “Animal,
Giraffe”?
6. You attend a conference and you introduce yourself and have to
say that you are from Rwanda. How would you sign it?
7. You are sick, and you want to go to the hospital, how would you
sign the words” Hospital, doctor”?
Numbers in Rwandan sign languageVocabularies related to sign language of numbers and their meaning
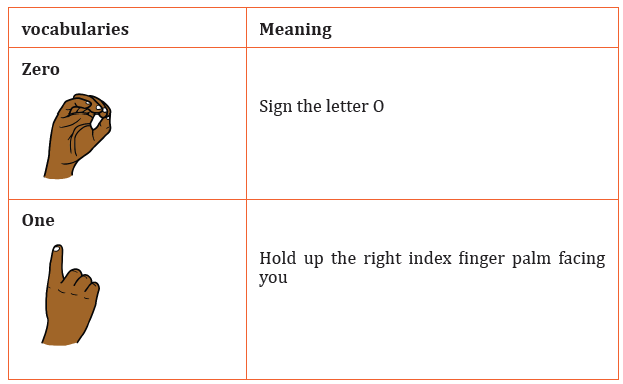
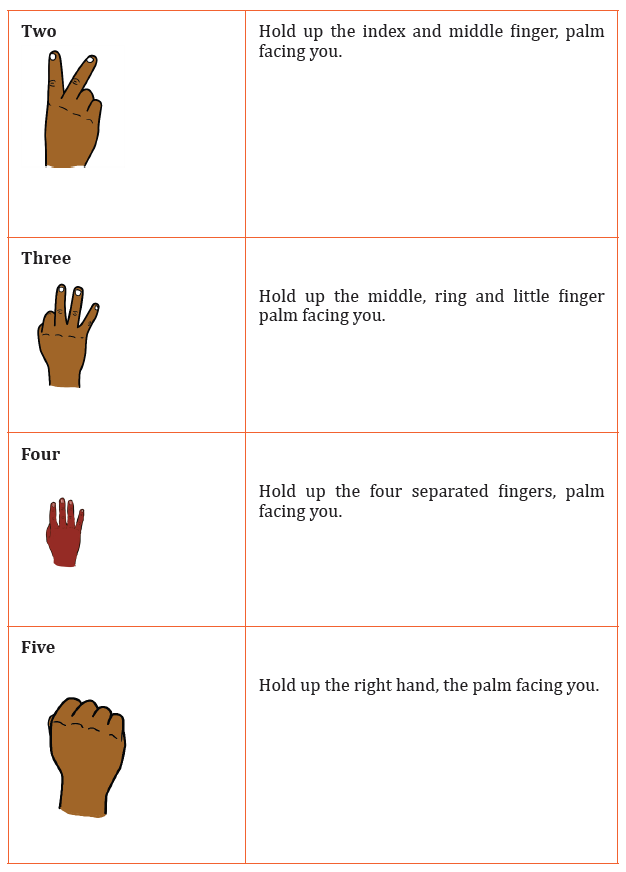
Greetings related vocabularies
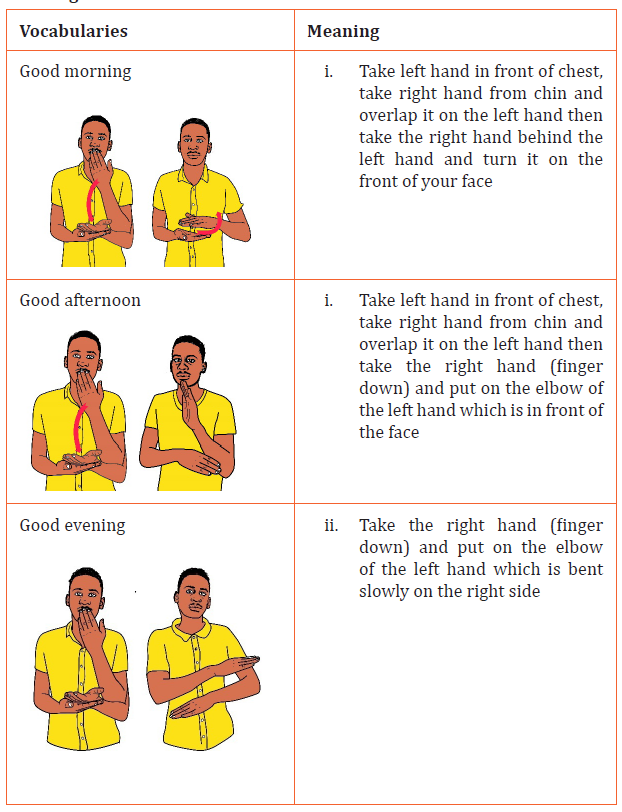
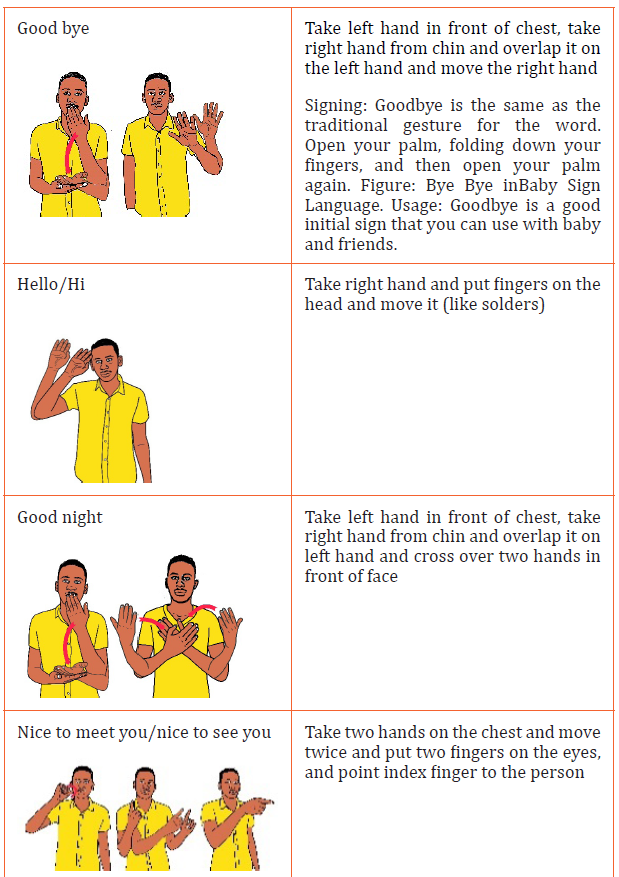
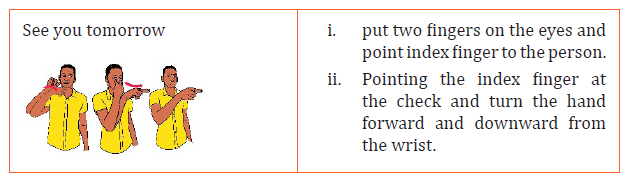
Family related vocabularies
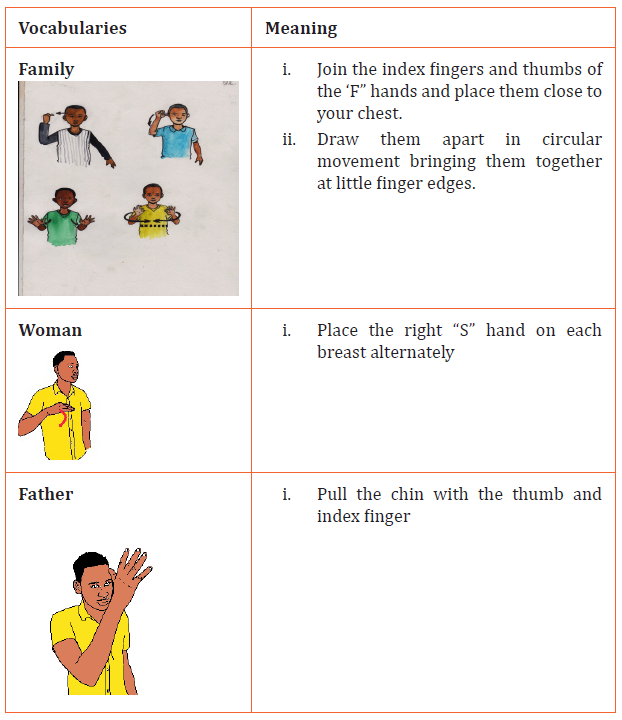
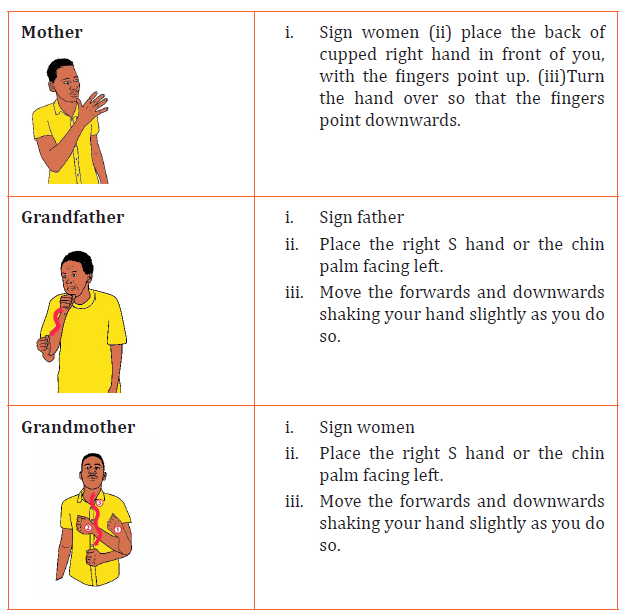
Food and drink related vocabularies
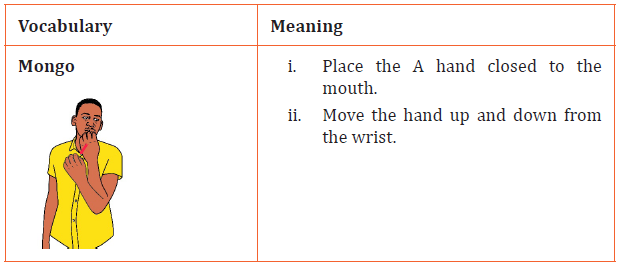
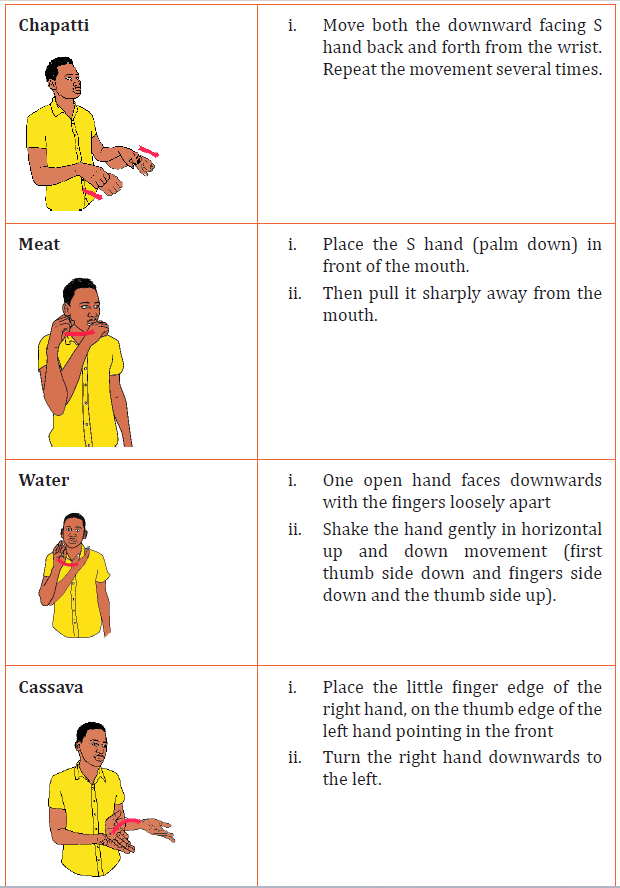
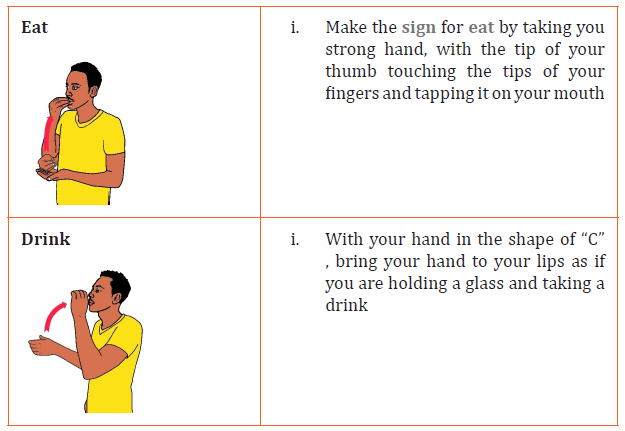
Animals related vocabularies
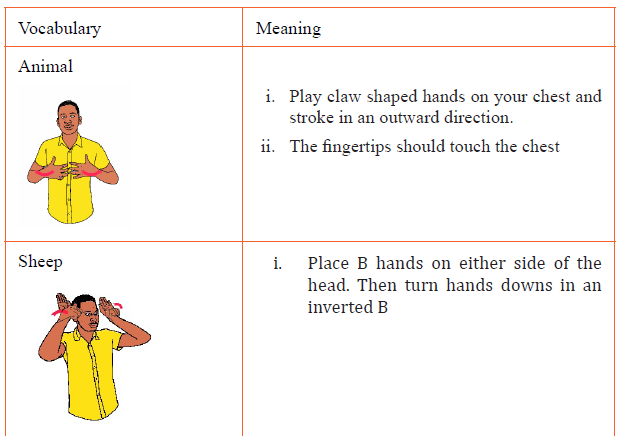
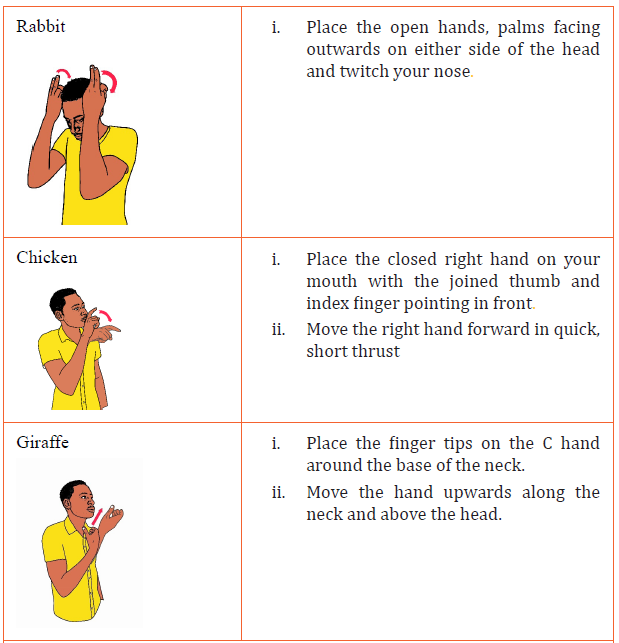
Countries related vocabularies
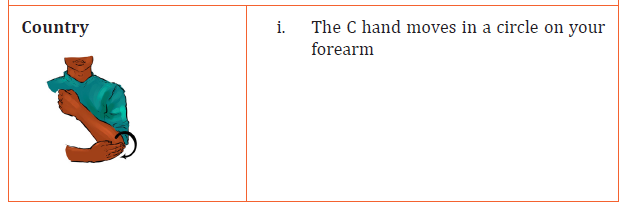
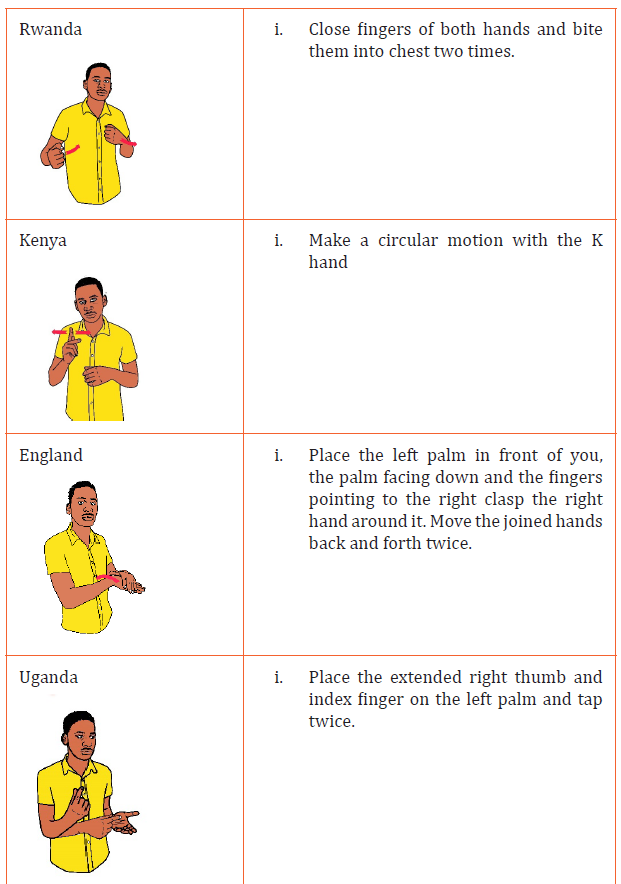
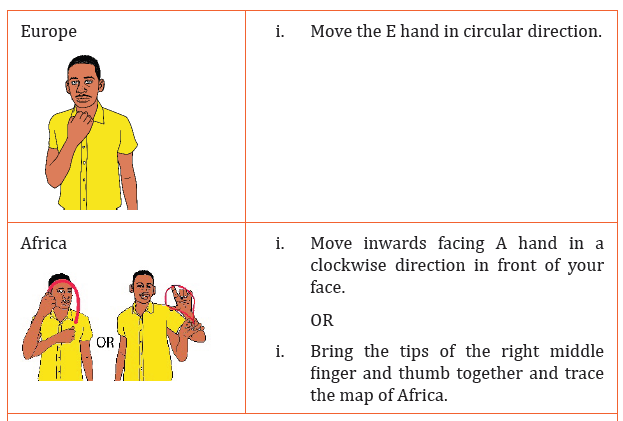
Education related vocabularies
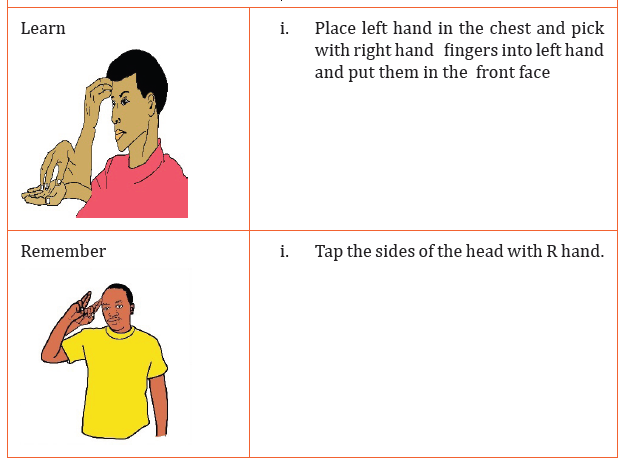
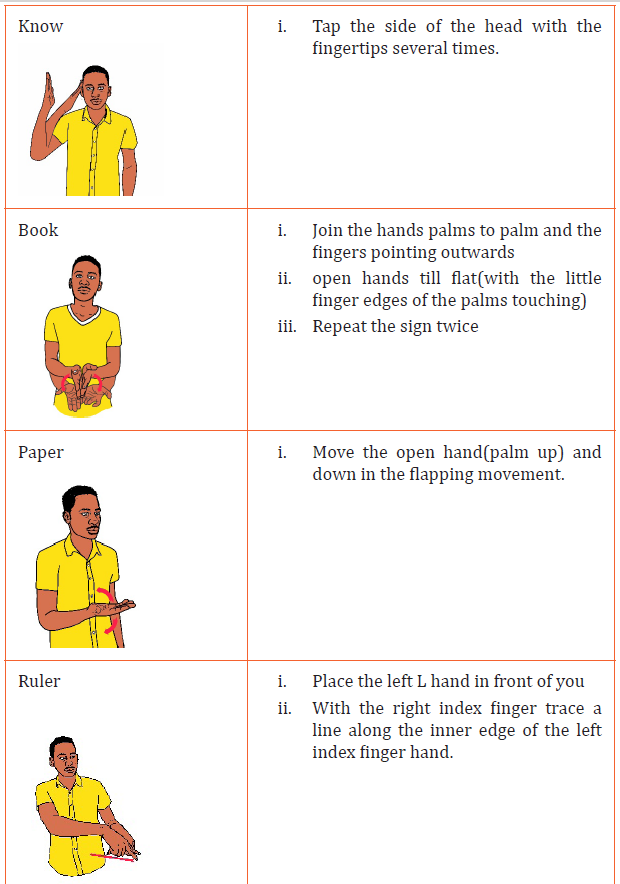
Health related vocabularies
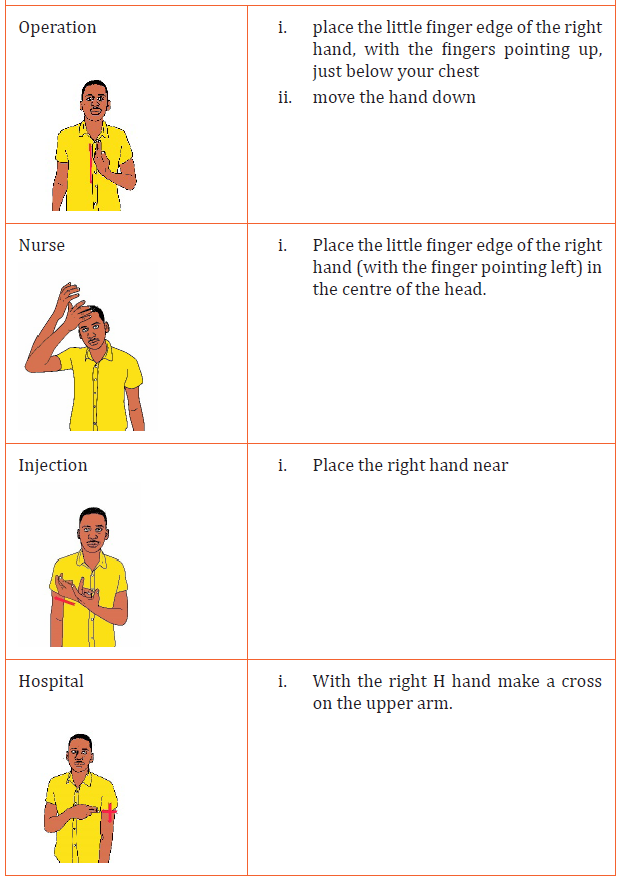
SELF-ASSESSMENT 12.1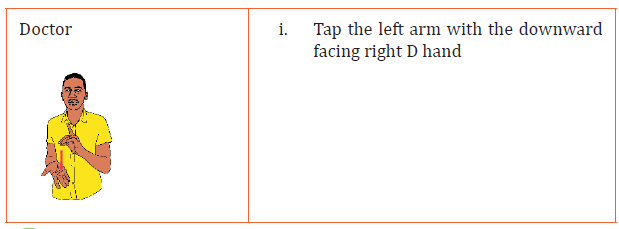
1. How would you sign the following words:?
• Doctor, Hospital, Book, Remember, Uganda, Rabbit, Water, Aunt
12.2. Sign language grammar rules
ACTIVITY 12.2
Sign Language grammar rules.
1. What do you understand by the word “grammar”?
2. Sign Language grammar is different from English Grammar. Givean example that can explain this statement.
The ten grammatical rules in Sign Language
Grammar in any language is a set of rules about how that language may be used.
These rules guide users in the correct speaking or signing of a language.Just
like most other languages, Sign Language has a set of rules that it follows when
being signed. A tool you can use to remember the rules is “TRIPSTONCL”, you
have probably heard about it, and it goes like this:
1. Topic/Comment
2. Rhetorical
3. Information Seeking
4. Pronominalization
5. Simple Yes/No
6. Tense With Time
7. Ordering of Simple Sentences
8. Negation
9. Conditional
10. Long Yes/No
Below are the definitions of each grammatical rule, and an example of each
written in Sign Language grammar and then put into English grammar.
1. Topic/Comment: In a simple topic/comment sentence, the topic is
described first, followed by the comment.
Example: HER MONEY LOST, SHE UPSET
English: She’s upset that she lost her money
The topic was described first (her money was lost) and then the commentfollowed (she was upset).
2. Tense with Time: The time sign is placed at the beginning or near the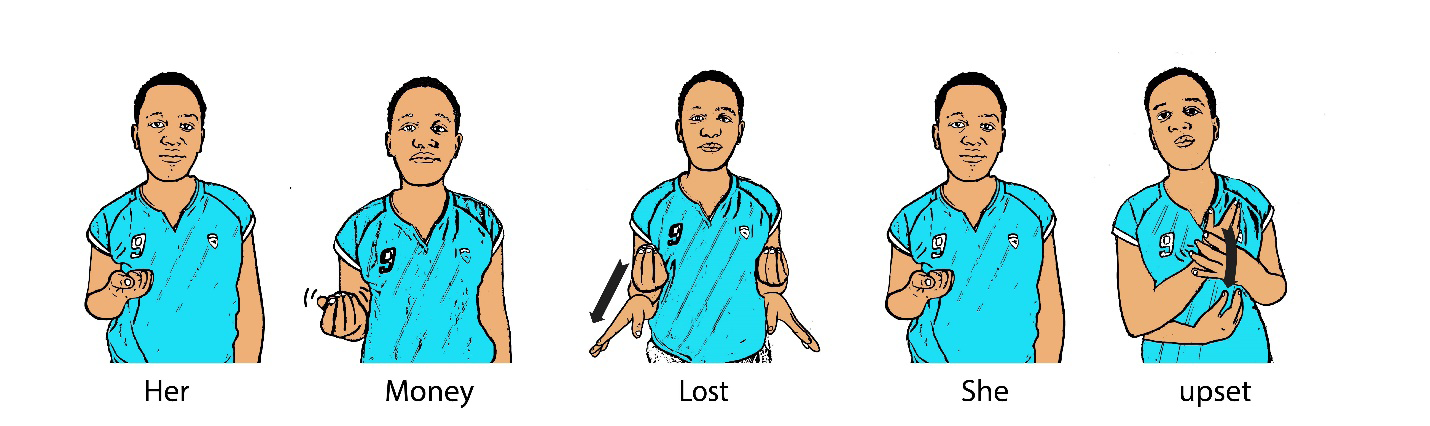
beginning of a sentences.
Example: YESTERDAY, ME STAY HOME
English: I stayed home yesterday.
The time sign was “yesterday” and was located near the beginning of thesentence.
3. Simple Yes/No: Short sentences that ask a yes/no question. The order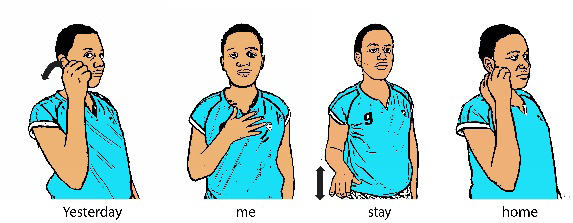
of the signs varies.
Example: EXERCISE YOU WANT YOU? with eyebrows raised
English: Do you want to exercise?
The sentence given was short and the answer would be a yes or a no; the orderof the signs could be moved around as well and mean the same thing.
4. Long Yes/No : Long yes/no questions, sometimes they use a topic/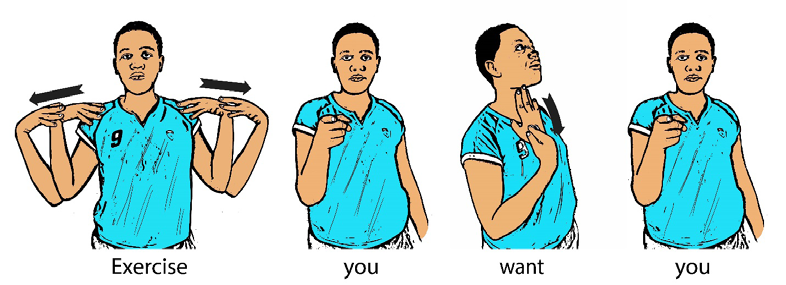
comment format.
Example: CAT BLACK TREE CLIMB, YOUR? with eyebrows raised
English: Is that black cat climbing the tree yours?
The question was longer than that of a simple yes/no; the topic was describedbefore the comment (which was the “your” part).
5. Information Seeking: Simple questions that ask for information. They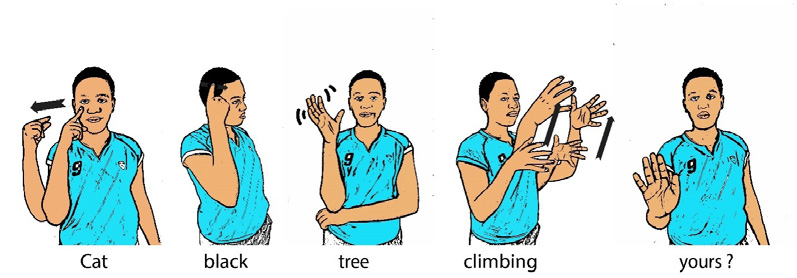
can have variable sentence structures, and rely sometimes on nonmanual
signals to distinguish them from a declarative sentence.
Example: OLD++ YOU? with eyebrows squeezed
English: How old are you?
The question was short and simple, the sentence structure doesn’t really have
much to change though. Normally, non-manuals would be used in all threequestion situations.
6. Pronominalization : Pronouns are indicated by pointing to either a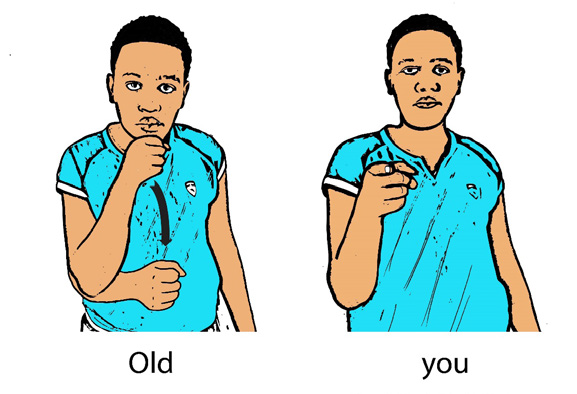
person or thing that is present, or a place in the signing space that is used
as a referent point for a person or thing. Pointing is mostly done with the
index finger, but eye gazing and other handshapes are sometimes used.
Example: MY BROTHER VISIT-MEEnglish: My brother is visiting me.
In this case, the pronominalization was when “he” was used; you could eitherbe pointing at the brother or a spot in your signing space to refer to as “he”.
7. Rhetorical: In a rhetorical question, the signer asks a question and then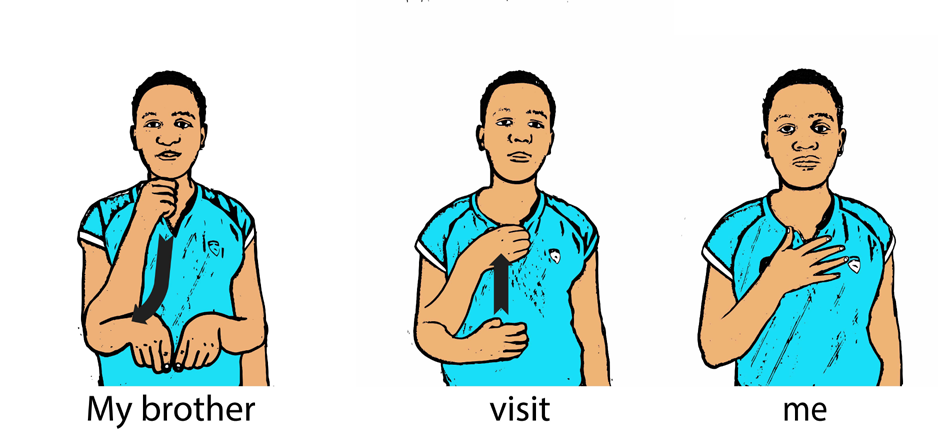
answers it.
Example: ME KNOW SL? YES.
English: I know SL.
The signer asked his or her question, and then answered it; by doing so, weknew he or she knows SL.
8. Ordering of Simple Sentences: In simple sentences, the verb can be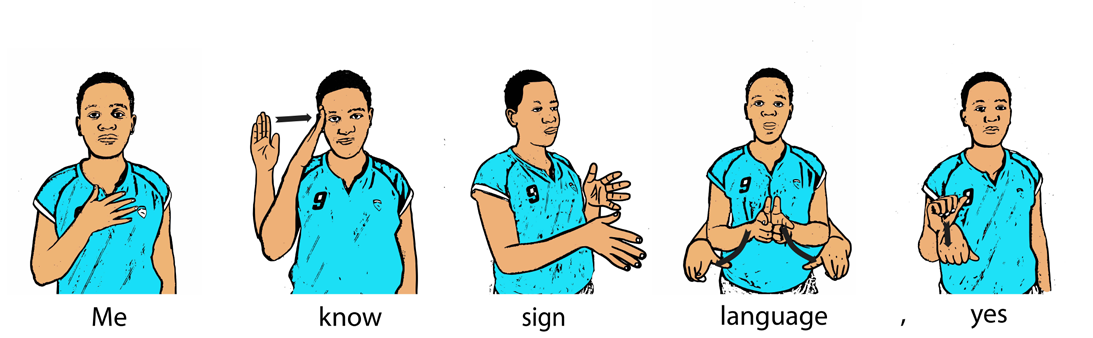
placed before or after the object of the sentence.
Example: GAME ME PLAY
English: I’m playing a game.
The sentence was short and simple, and we were allowed to move around theverb and not have it change the sentence.
9. Conditional: In a conditional sentence, the condition is described first,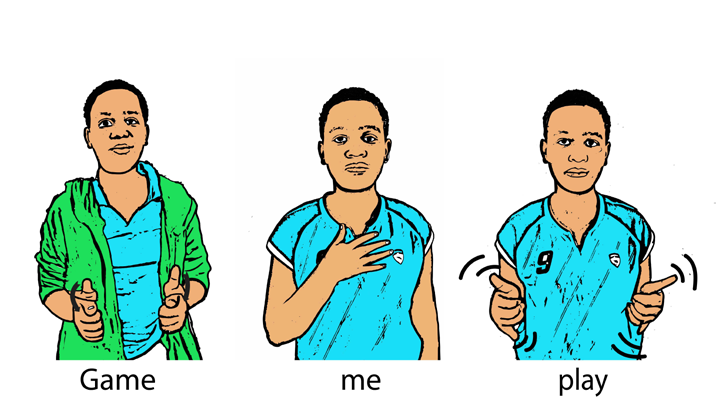
then the outcome of the condition is described.
Example: SUPPOSE SHE SEE ME, ME HAVE-TO LEAVE
English: I will have to leave if she sees me.
In most conditional statements, the word “suppose” is used; the condition was
said first (suppose she sees me), and then the outcome came afterward (I’llhave to leave).
10. Negation: You can negate a thought by placing a negative sign before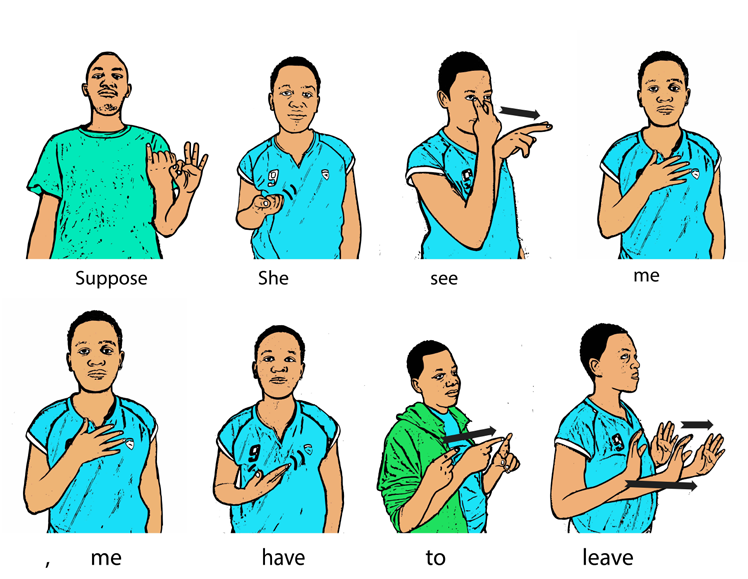
the verb or by first describing a topic and then signing the appropriate
negative sign, or by giving a negative head shake.
Example: ME NOT WATCH FOOTBALL GAME.
English: I’m not watching the football game.
In this case, the word “not” was the negation portion of the sentence, makingthe sentence negative.
SELF-ASSESSMENT 12.2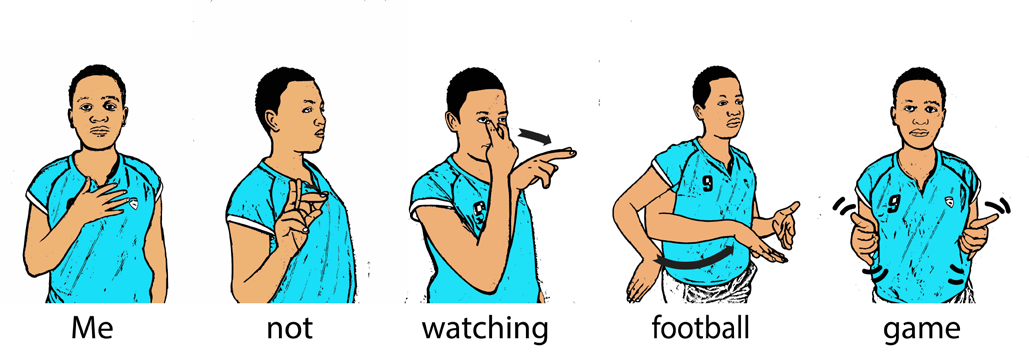
Give the correct sentence and it sign language
1. My brother visit-me
2. Yesterday, me stay home
3. Exercise you want you?
12.3. Approach of teaching and learning for deaf and hard
of hearing learners
ACTIVITY 12.3
1. Teaching deaf require a particular method and techniques.
Discuss
Approach used in education of deaf children
Before putting into action any kind of educational approach it is better to firstly
assess the severity of the hearing loss. After, you can pick a method for each
individual child. There are three primary communication methods used in
education of deaf children. These are:
a. Oral/aural:An approach to deaf education that emphasizes auditory
training, articulation ability and lip-reading.
b. Total communication: A method of interacting with individuals with
language impairments using a combination of spoken language and
signs, which includes sign language, voice, finger-spelling, lip-reading,
amplification, writing, gesture and visual imagery (pictures).
c. Bilingual/bicultural (bi-bi):This is a philosophy of teaching that
recognizes the authenticity and importance of both hearing and Deaf
cultures, and that incorporates elements of both in the classroom.
Techniques that are used to help the child with a particular method
In these methods there may be techniques that are used to help the child with
a particular method, such as:
a. Cued Speech:A manual used by some deaf children and their teachers/
parents, that uses hand shapes near the mouth to help make lip-reading
easier.
b. Lip-reading (Speech-reading):Decoding the language of a speaker by
paying close attention to the face and mouth, without being able to hear
the speaker.
SELF-ASSESSMENT 12.3
1. Explain trees approaches used to teach deaf learners?2. Discuss on at least 2 techniques of teaching deaf learners
SKILLS LAB
1. You are invited in a meeting to interpret for deaf persons. How
would you interpret the following sentences:
• I am eating two chapattis
• I will see my father tomorrow
• My country is Rwanda
• I sell chicken
• I have two sisters
• I saw a doctor yesterday
END OF UNIT ASSESSMENT
1. What is the sign language of the following numbers: 1,3,4?
2. What is the sign language of following family members: Father,
Mother, grandfather, woman?
3. What is sign language of the following greetings?
a. Good Morning b. Good Afternoon c. Good Evening d. Goodbye
f. nice to meet you
4. What is the sign language of the following food?
1. Water 2. Meat 3. Cassava5. 4. Mango
5. Give the correct sentence and it sign language
1. My brother visit-me
2. Yesterday, me stay home
3. Exercise you want you?
6. Discuss on the techniques and approaches of teaching deaflearners.
UNIT 13 INTERMEDIATE LEVEL OF BRAILLE AND TEACHING APPROACHES FOR LEARNERS WITH VISUAL DIFFICULTIES
Key Unit Competence: Use Braille transcriptions at intermediate level,
and teaching approaches for learners with visual
difficulties.
INTRODUCTORY ACTIVITY
Read the following passage and answer the questions
Mukunzi was born in Kigali, Kimironko sector, Gasabo District. She was
born in a family of four children where she was the first-born. Mukunzi was
very beautiful girl who was loved by many people in her family. She started
school at the age of six and when she was in class four, she lost her sight as
a result of an infection and became totally blind. This meant that she could
not continue with her education and she was forced to remain at home when
her brothers and sister went to school. Her parents were psychologically
affected and lost contact with members of the family and also their friends
because of what had happened to their daughter. They went around looking
for people who could treat their daughter. Finding no proper treatment in
hospitals they decided to go for traditional medicine.
One day some blind people heard about Mukunzi and they decided to visit
her home. When they arrived there, they met with Mukunzi’s parents and
had a very good discussion with them. They narrated their success stories
and this opened the eyes of Mukunzi’s parents. After two days, the father of
Mukunzi took her to a school for visually impaired where she was admitted
and continued with her education. She was introduced to Braille where she
learnt uncontracted and contracted Braille and also Mathematical numbers
and signs for a period of one month. Mukunzi learnt braille very first and
she was placed in class five surprisingly she was in class for two months and
managed to get the first position after sitting for end term examinations. Her
parents were very happy because they saw the bright future in their daughter.
The neighbors and members of the family who had kept off from this family
started talking to them and also visiting their home. After completion of
primary education Mukunzi went to High School passed her final exams very
well and joined the university where she graduated as a lawyer. Her brothers
and sister never managed to join any university and this made it very clear
that when her child who is blind gets proper education he or she
can be very successful in life. What is required is just an opportunity and
they can show the world what they can do. Mukunzi got a job as a Lawyer
and she managed to support herself and her parents financially. Today she
loves Braille because she feels that if Braille was not there she could not be
living a successful life just like her peers without disability.
1. When did Mukunzi loose her sight?
2. Who informed her parents about school for the visually impaired?
3. What did Mukunzi learn when she arrived in the school?
4. How many children did the parents of Mukunzi have?5. Which child had the highest academic qualifications in this family?
13.1. Intermediate level Braille tactile transcriptions (Vocabulary,
punctuations, figures, math signs etc.)
ACTIVITY 13.1
1. Write in Braille these letters of alphabet: a b c d e f g h i j k l m n o
p q r s t u v w x y z?
2. Why do you think that Braille books are bigger in size compared to
print books?
3. Do you know any words represented by letters of the alphabet when
standing alone in a Braille text?
4. What are the five special common wordsigns?
5. What is the purpose of contractions in braille?
6. List some mathematical signs that you know?
13.1.1. Vocabulary
Simple sign – A sign occupying one cell only.
Upper sign – A sign containing dot 1, or dot 4, or both.
Contraction – A sign that represents a word or a group of letters.
Groupsign – A contraction that represents a group of letters.
Wordsign – A contraction that represents a whole word.
13.1.2. Simple upper wordsigns, five special common wordsigns
and abbreviations.
The following table shows how the letters of the alphabet are used in braille
to represent whole words when they are standing alone; usually it is the firstletter that is taken.
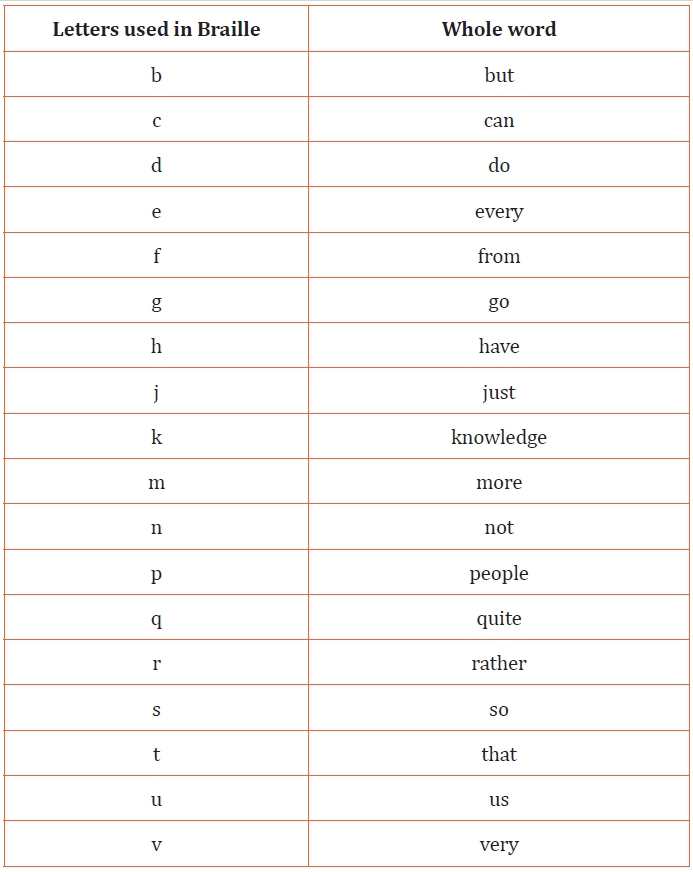
Letter a, i and o do not represent any word in Braille.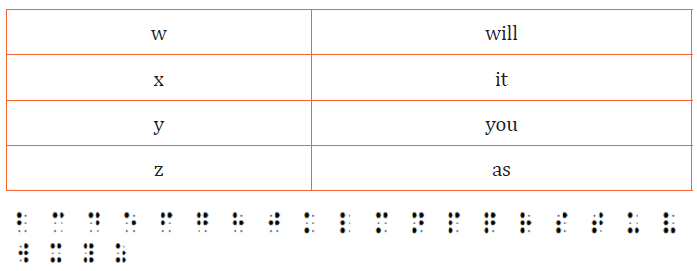
Single letters used in this way to represent words are called simple upper
wordsigns; simple because they take up one cell, upper because they have a dot
in the top of the cell, and wordsigns because they represent words. They may
only be used as abbreviations for the word if they represent the exact word, i.e.when no other letters are added to them.
Abbreviations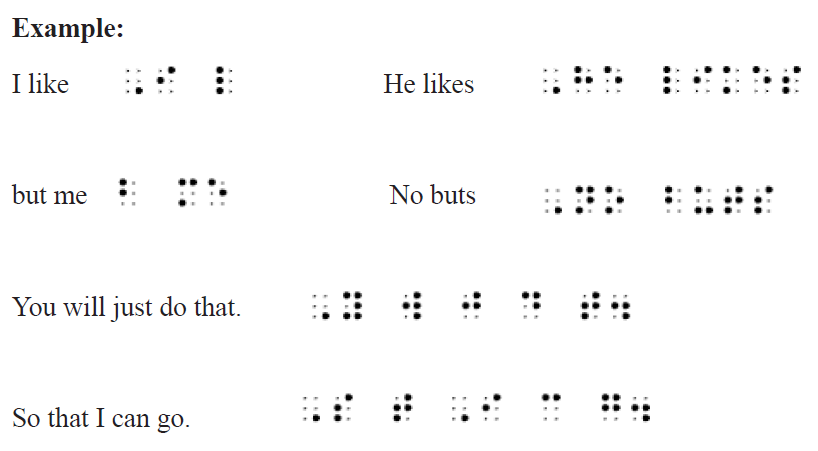
Ab: about; cd: could; xs:its; Td: today; alw: always;
Sd :said; yrf:yourself; acr:across; fr:friend; xf:itself; gd: good;
Ll: little; wd :would; brl: Braille;Grt:great; qk: quick; yr:your.
13.1.3. Five special common wordsigns (and, for, of, the, with)
One uniqueness about these five wordsigns is that where two or more of these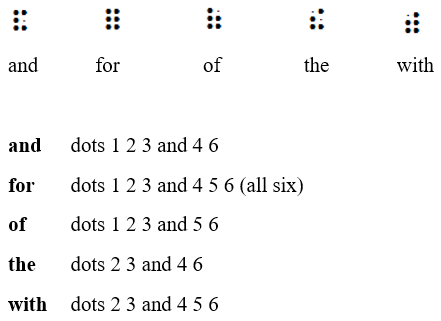
words came in succession and in the same phrase, the wordsigns that express
them are written adjoining one another (if in the same line of Braille) as if they
were one word, in order to save space.Example: with the knowledge of the people and for the purpose.
The article “a” is similarly to be written unspaced from any of these wordsigns
in the same line of Braille.Example: and a and with a

Having learnt the words represented by the letters of the alphabet and the five
special common wordsigns you should always remember the rules that govern
them.
13.1.4. Contractions used in Braille
Groupsigns are signs expressing two or more letters which form part of a word.
Let us groupsigns which have at least one dot on the top line of the cell i.e. dot 1
or dot 4, or both, and which occupy only one cell. They are called simple uppergroupsigns (or one-celled upper groupsigns).
And, for, of, the, with, as Groupsigns
We begin with the very same five signs which we had learnt previously as
wordsigns to represent these five words. For these signs are also used as
groupsigns or contractions to present the letters they stand for in a word.Example:
Abbreviations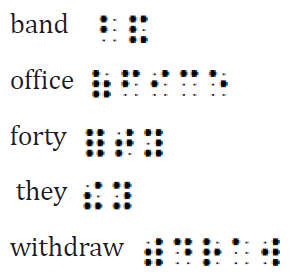
Afn : afternoon; ag: again;
Hm: him; pd: paid Five Upper Groupsigns (with h)
Choice of Contractions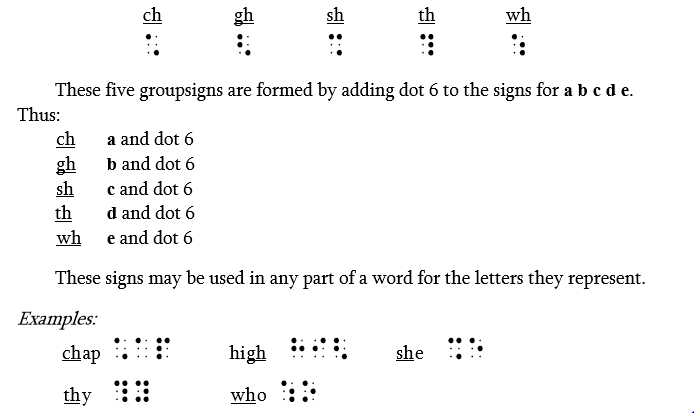
If “th” is followed by “e”, the groupsign to be used is the, because it represents
the greater number of letters, as: then them clothes other.
Wordsigns ch, sh, th and wh are also used as wordsigns:
ch stands for “child”
sh stands for “shall”
th stands for “this”
wh stands for “which”
They may only be used to express the exact word they represent and when noother letters are added to them.
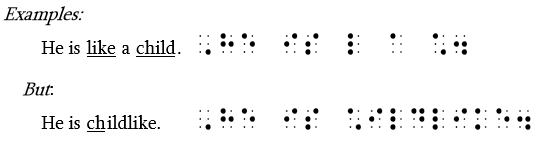
Abbreviations
Al: also; bl: blind;
(ch)n: children; m(ch): much;
(sh)d: should; s(ch) such; tgr : together
Four upper Groupsigns two with e and two with o
Choice of Contractions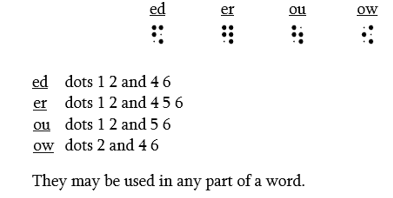
In words containing the letters “thed” and “ther”, use the groupsign the inpreference to the groupsignsth and ed or er. As: cathedral further.
Wordsign
Of these four groupsigns only one, ou, is also used as a wordsign: it stands for
out. It may only be used where it represents the whole word and where no
other letters are added to it.Example:
Abbreviations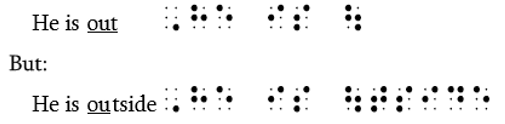
Abv: above; af: after; alm: almost
Alr: already; al(th): although The last four Upper Groupsigns
st dots 3 and 4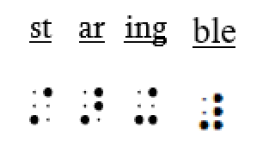
ar dots 3 and 4 5
Both of these signs may be used in any part of a wordExample:
st by itself stands for the word “still”.
ing dots 3 and 4 6
ble dots 3 and 456
These signs (ing and ble) may be used in any part of a word except at thebeginning.
Example:
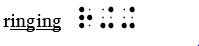
Abbreviations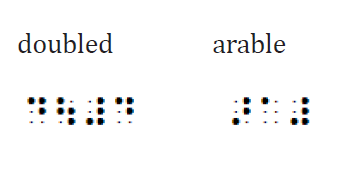
F(st) first; m(st) must;
Tm tomorrow; ac according13.1.5. Punctuation marks
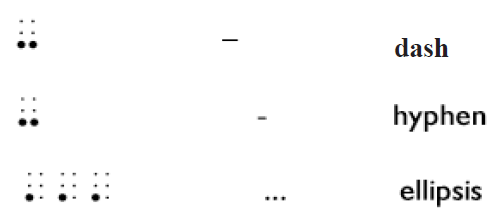
Example:

Child-like

- staring asters steed

- straightest artist farther

- sharper quarrel fare

- winged stinging arriving

13.1.6.Numbers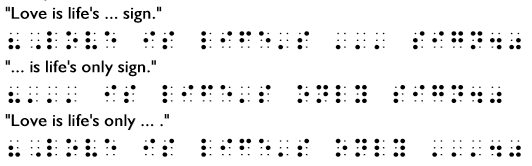
13.1.6.1. The decimal numbers
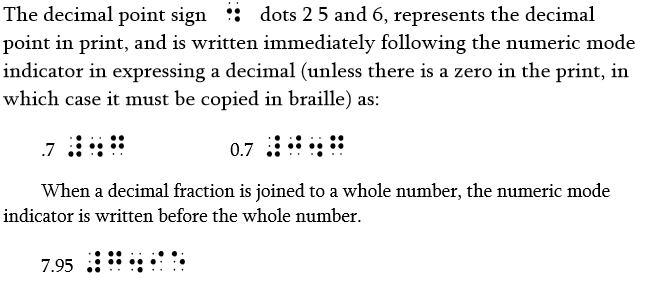
Roman Numbers

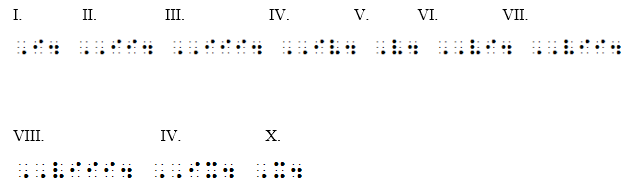
Example:
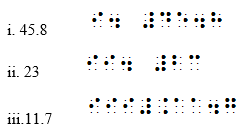
Mathematical signs
Example:
(12 + 4) x (8 - 3) = 80

[(16 + 1) x (5 + 7)] =
SELF-ASSESSMENT 13.1
1. Debraille the following words and sentences:
13.2. Teaching approaches for learners with visual difficulties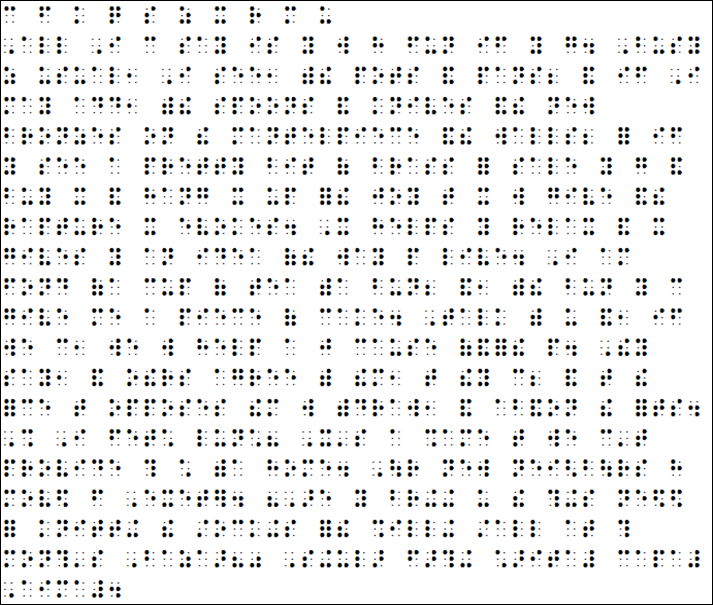
and related resources
13.2.1. Teaching approaches for learners who are blind
ACTIVITY 13.2
1. What methods do you think a teacher can use in class to teach a
learner with visual impairment effectively?
2. Explain some of the braille equipment used in teaching braille to
learners who are blind.
In order to address the needs of blind students, teachers may use the following
methods in teaching them Braille and other subjects in class:
• Use real object in order to understand a literary description. This is
because learners with visual impairment understand better when they
touch an object which they can observe using their hands.
• Add descriptions to all images.
• Use life situation in order to develop the communication skills.
• Dramatize the stories by role play.
• Repeating the information as many times as it takes for the students to
properly understand
• Reading Braille takes more time than reading print. Therefore, the
teacher should allow more time to vocabulary exercises (solving
synonyms, antonyms, homonyms, the meaning of words in contexts,
spelling exercises, etc.) in order to improve communication and avoid
stereotypes.
• Use riddles to develop creativity
• Allow more time for tests and national exams;
• If the book is not in Braille, use audio-books.
• Reading, theatre and other art forms helps the blind to develop
vocabulary, imagination, communication and become an integrated
and a successful person- access to information.
• Good Braille reading is characterized by few zigzag, up-and-down,
or fluttering movements, uniform pressure of the finger on the page,
no regressive movements and well-adjusted movements between
lines with the help of both hands combined with a deep and accurate
understanding of the meaning of the text.
• If necessary, teachers should use one to one approach in teaching
Braille or alternatively they use whole class approach.
• Individual attention is paramount when teaching Braille to beginners
just like any other practical subject.
• It is important that for a child with visual impairment attention be
given to the development of tactual perception and listening skills.
• Students will need special instruction to learn to read and write braille
code.
• The teacher before introducing the child to the slate and stylus he/
she should use the Braille cell peg board. The board has six holes and
each hole represents a braille dot. The pegs should be used to write
the letters of the alphabet. For instance: one peg placed in first hole on
your left hand side will be letter a; if another peg is placed in second
hole downwards still on the left hand side the letter will now be b
represented by dots one and two.
• Usually students are introduced first to the alphabet and uncontracted
braille, and once they are proficient in recognizing and producing
letters, they move on to contracted braille.
Now let us look at related resources used by learners with visual impairment
Writing and reading usually begin at age 6-7 years (depending on country)
and is usually acquired at school. Blind students learn to write the Braille code
using a Braille typewriter (Perkins in most cases) at the same age as studentswithout disabilities

Perkins Typewriter for blind students; the six keys are numbered
Slate and Stylus
Braille characters are small rectangular blocks called cells that contain tiny
palpable bumps called raised dots. The number and arrangement of these dots
distinguish one character from another. A full Braille cell includes six raised
dots arranged in two lateral rows each having three dots. The dot positions are
identified by numbers from one through six.Single cell pegboard
This a board where learners use pegs to write letters of alphabet

Numeral Cell peg Boards

This board can be used to teach number facts, counting, number recognition,
beginning addition and subtraction, number relations, sequencing and color
recognition, and it even helps develop fine motor skills especially to preschool
children.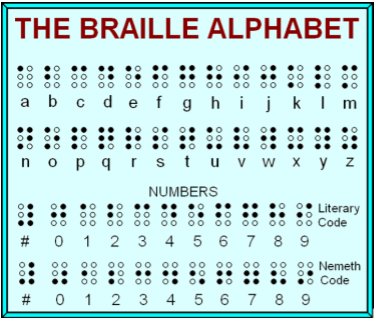
Braille Alphabet chart including numbers
Victor Reader
The Victor Reader is used to record all the lectures. The learner plays it back tolearn more as he/ she revise.
SELF-ASSESSMENT 13.2
1. Why do you think Braille reading takes a longer time than print
reading?
2. Write down any three equipment used in writing Braille?
3. Explain at least three teaching approaches used in teaching
braille to learners who are blind?
SKILLS LAB
1. Visit a nearest school, identify a child with Visual Impairment.
Assess the method he/ she uses in reading (large print, braille).
Write a two-page document to advise the teacher on how to
effectively teach braille to learners with Visual Impairment.END OF UNIT ASSESSMENT
1. Write down the words represented by the following letters in Braille:
2. List down three special common wordsigns
3. Write down the words represented by the following Braille signs:
4. Write the following in Braille:[(1309.67 – 0.28954) : (523.243 +
100)] x (2 +32) =
5. Write any two equipment and two teaching approaches used in
teaching Braille to learners who are blind.6. Debraille the following sentences
UNIT 14 LESSON PLANNING FOR LEARNERS WITH SEN IN AN INCLUSIVE CLASS
INTRODUCTORY ACTIVITY
Uwimbabazi has been a primary teacher since 2007. In the school year
2010, her school decided to be an inclusive school and therefore has to teach
in her class, two learners with intellectual disabilities and one learner with
Visual Impairment. She has been trained by REB on how to teach learners
with different types of disabilities and she has no problems in planning an
inclusive lesson. Every time Uwimbabazi is going to prepare a lesson, she
asks her self these questions: What are the abilities and characteristics of my
learners?What I am going to teach, how I am going to teach it, what should
learners be able to know or do by the end of the lesson, and how will I know
if they know it or can do it?
Uwimbabazi is a good teacher who is a role model to many teachers. She
takes care of all her learners needs and all participate actively. She takes
time to prepare an inclusive lesson to make sure all her students are actively
participating. No wonder, this year she has been rewarded by REB as an
innovative teacher and best performer in all the country. It is true: Hard
work always pays off.
1. What makes Uwimbabazi an innovator and best performer teacher in
the country?
2. There are important questions every teacher should ask him or herselfbefore he /she deliver a lesson, what are those questions?
14.1. Definition and importance of a lesson plan
ACTIVITY 14.1
1. How would you explain the term” Lesson Plan”?
2. Do you think, it is necessary to have a lesson plan before you
teach? Why?
Good lesson planning is essential to the process of teaching and learning. A
lesson plan is a teacher’s detailed description of the course of instruction or
‘learning trajectory’ for a lesson.
A daily lesson plan is developed by a teacher to guide class learning. Details will
vary depending on the preference of the teacher, subject being covered, and the
needs of the learners. A lesson plan is a detailed description of the individual
lessons that a teacher plans to teach on a given day. A lesson plan is developed
by a teacher to guide instruction throughout the day. It is a method of planning
and preparation.
Lesson plans are the teachers equivalent of a blueprint for a construction project.
Unlike construction, where there is an architect, construction manager, and a
myriad of construction workers involved, there is often only one teacher. They
design lessons with a purpose and then use them to carry out the instruction to
construct skilled, knowledgeable students. Lesson plans guide the daily, weekly,
monthly, and yearly instruction within a classroom.
Dynamic lesson planning is time-consuming, but effective teachers will tell you
that it lays the foundation for student success. Teachers who fail to put in the
proper time to plan accordingly short change themselves and their students.
The time invested in lesson planning is well worth any investment as students
are more engaged, classroom management is improved, and student learning
naturally increases.
The following are the importance of lesson planning:
• Lesson- Planning gives the teacher greater assurance and greater
freedom in teaching. The teacher who has planned his lesson wisely,
enters the class-room without anxiety, ready to embark with confidence
upon a job he understands and prepared to deliver.
• It provides for adequate lesson summaries, ensures a definite
assignment for class, and availability of materials for lesson when
needed.
• Since lesson planning establishes proper connections between different
lessons or units of study, it provides and encourages continuity in the
teaching process.
• It enables the teacher to know the most desirable type of teaching
procedures and to prepare tests of progress and checks for judging the
outcomes of instruction.
• Lesson-planning prevents waste because it helps the teacher to besystematic and orderly. It saves him form haphazard teaching.
SELF-ASSESSMENT 14.1
1. Explain what is a lesson plan?
2. Discuss the importance of lesson planning in teaching and
learning process?
14.2. Key elements in lesson planning
ACTIVITY 14.2
1. What do you think should be included in the lesson plan?
2. With an example, explain the difference between learning
objectives and instructional objectives
Planning a lesson is an important responsibility for a teacher and critical for
enhancing the students’ learning and teacher’s confidence. The competencebased
lesson plan has 27 different parts that teachers are expected to complete.
a. Check your scheme of work
Before the start of every academic year, teachers accomplish the scheme of
work based on the subject syllabus, the school calendar and time allocated
to the subject per week. For lesson plan preparation, consider the following
questions:
• What lesson have you planned to teach in a given period, such as a
term, a month and a week?
• What key competence do you hope to develop by the end of unit?
b. Identify the generic competences and cross cutting issues
From the scheme of work, the teacher identified the key unit competence by
looking at the subject syllabus. Each lesson must also incorporate generic
competences and cross cutting issues.
c. Set instructional objectives for the lesson
An instructional objective should have at least 5 components. The following
steps can guide you to write the statement:
1. Determine who you’re talking about
2. Note the behaviour/action/competence you’re looking for - evidence
of student action (choose from the list of verbs in the tips and aim for
higher levels of comprehension).
3. Include the content you want the student to learn
4. Reflect on the conditions, or how the student will accomplish the task
5. Have a standard of performance - criteria for acceptable performance
Examples of instructional objectives
1. Using an extract on agricultural products from an article in The New
Times, and transcribed in Braille for learners with Visual difficulties,
the learners will be able to read one paragraph on the importance of
avocado fluently 150 words in 5 minutes, 10 minutes for learners with
speech difficulties and 15 minutes for those with cognitive difficulties.
• Who: Learners (diverse learners)
• Behaviour: Will be able to read
• Content: one paragraph on the importance of avocado
• Condition: Using an extract on agricultural products from an article in
The New Times
• Performance standard: Fluently in fixed time
2. Given a gap-filling exercise on elements of a good map, learners will be
able to indicate and explain correctly the 5 elements of a good map in
5 minutes and in 15 minutes with more explanation for learner with
cognitive challenges. The teacher will read for the two learners with
visual difficulties and allow them to answer verbally.
• Who: Learner including those with intellectual disabilities and Visual
Impairment.
• Behaviour: Will be able to indicate and explain
• Content: Element of good map
• Condition: Using gap-filling exercise on elements of a good map
• Performance of standard: Correctly in fixed time
d. Identify the types and number of learners with SEN
In the section titled ‘Type of Special Education Needs and number of learners in
each category’, insert the type of SEN that you have identified in your class, and
the number of learners with SEN in the class. In addition, note how learners
with SEN will be integrated or accommodated in the game or activity so that
they are also able to participate and learn.
e. Identify organizational issues
This part of the lesson plan conforms to creating positive learning environments,
specifically related to physical safety and inclusion. In the section titled “Plan
for this Class (location: in / outside)”, you can write down where you will hold
the lesson.
f. Decide on the teaching and learning activities
In this part the teacher summarizes the learning and teaching process
including main techniques and resources required. Afterwards, the teacher
details activities to be carried out by the teacher and learners. In the column
of teacher’s activities, the teacher describes the activity using action verb in
infinitive form. The questions and instructions provided by the teacher are also
written in this column. In column of learner’s activities, the teacher describes
the learners expected activities, findings and answers. However, for some
activities or answers which cannot fit in that column, the teacher will indicate
them in appendix. The teacher will specify if the activities will be carried out
individually, in small groups, or by the whole class.
In the column of the generic competences and cross cutting issues to be
addressed, the teacher writes down generic competences to be developed
through learners’ activities and how they will be developed. The cross-cutting
issues to be addressed depend on the lesson content and activities. In the
column of steps and timing in the lesson plan format, there are three mainsteps; introduction, development of the lesson and conclusion.
SELF-ASSESSMENT 14.2
1. Explain briefly the key elements of lesson planning?
2. What is an instructional objective? Develop an inclusive
instructional objective?
14.3. A sample of an inclusive education lesson plan
ACTIVITY 14.3
1. What do you understand by inclusive lesson plan?
2. What are the main parts of a lesson plan?
Physical Education Sample Lesson PlanSchool Name: GS Mayange A Teacher’s name Mutware Leopord
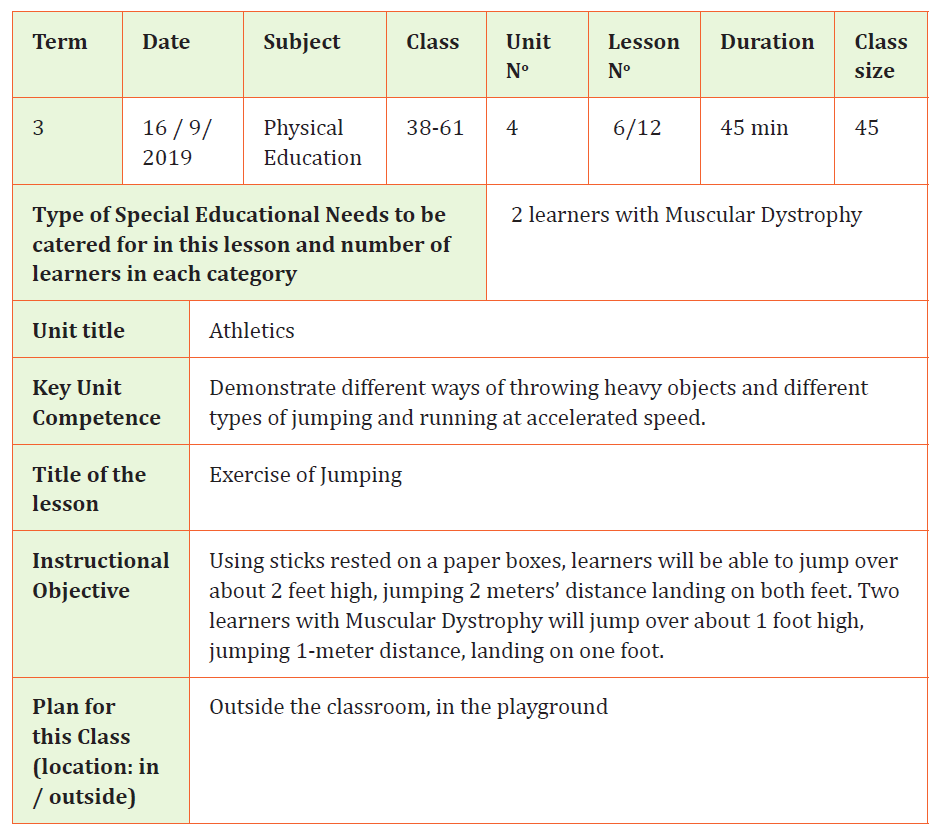
SELF-ASSESSMENT 14.3
1. Briefly explain the element of inclusive lesson plan?
2. Analyse the instructional objective set above and show the
component of inclusive instructional objective?
SKILLS LAB
1. After you have graduated from TTC Rubengere, you have
been deployed to teach mathematics at EP Kayenzi. You are in
primary four and you have to teach a lesson on: “Reading and
writing numbers in words and figures”. In your class, you have
two learners with Dyscalculia and one learner with Visual
Impairment. Prepare an inclusive lesson plan and deliver it.
END OF UNIT ASSESSMENT
1. With an example, explain the components of an instructional
objective?
2. What do you think, teachers should have a lesson plan?
3. In your own words, explain what lesson plan mean?4. What are the main elements of an inclusive lesson plan?
REFERENCES
Braille Authority of North America (1994). English Braille American Edition.
American Printing: House of Printing.
Braille Authority of the United Kingdom (2004). A Restatement of Standard
English Braille Compiled and Authorized. Royal National Institute of the Blind
Bakewell Road, Orton.
Gargiulo, R.M. (2009). Special Education in contemporary society: An introduction
of exceptionality. SAGE, Los Angeles, London.
Hallahan, DP &Kaufffman, J.M(2007). Human exceptionality. School community
and family. New York: Allyn and Bacon
Howse, J., Kathy, R., and Leona, H. (2013). Unified English Braille: Australian
Training Manual. Australia: Round Table on Information Access for People with
Print Disabilities Inc.
Howse, J. (2006). Unified English Braille Primer. Australia. The NSW Department
of Education and Training Publisher.
Mwaura, M., and Mweu, J. (2009). Braille I (Basic English Braille). Kenya Institute
of Special Education.
Ndurumo, M. (2001). Exceptional learners: Developmental consequences and
intervention. Nairobi: National learners in needs network.
Rwanda Education Board ( 2018), All Children can learn together, Toolkit for
Awareness raising on Inclusive Education in Rwanda. Kigali, Rwanda.
Rwanda Education Board (2018). Training manual on Special Needs and
Inclusive Education.Kigali, Rwanda.
Rwanda National Union of the Deaf (2009). Rwandan Sign Language. First
Edition, Kigali.
HWO (2019)Learner