Topic outline
UNIT 1 MEDICAL PATHOLOGIES OF RESPIRATORY SYSTEM
Key Unit Competence
Demonstrate an understanding of the appropriate management of different commonMedical pathologies of respiratory system.
Introductory activity 1.0
Observe the picture below and answer the following questions:
1. Indicate the normal and abnormal lung on the above figure?
2. From the abnormal lung, what are the features did you observe?
3. What are the possible diseases that can affect the abnormal lung?
1.1 ASTHMA
Learning Activity 1.1
Read careflly this below situation and answer the following questions:
Mrs. T.N. is 40-year-old woman, an athlete comes to the clinical setting with
complaints of shortness of breathing, wheezing, mucus secretions, cough, chest
tightness and chest pain, the history taking revealed that her mother died due
to asthma, oxygen saturation was 78% on room air. Chest x-ray was normal,
complete blood count (CBC): within normal limits, white blood cells (WBC) were
10000 per microliter (Normal range: 4000-11000), eosinophils was 7% (Normalrange: 0.0-6.0%), allergy-skin test: Positive for dust, trees.
Mrs. T.N. then was prescribed treatment with a low-dose corticosteroid, fluticasone
44 microgram at two puffs twice per day. However, she remained symptomatic
and continued to use her rescue inhaler 3 times per week. Therefore, she was
switched to a combination inhaled steroid and long-acting beta-agonist (LABA)
(fluticasone propionate 250 microgram and salmeterol 50 microgram, one puff
twice a day) by her primary care doctor. Her dose of inhaled corticosteroid (ICS)
and LABA was increased to fluticasone 500 microgram/salmeterol 50 microgram,
one puff twice daily. However, she continued to have symptoms and returned tothe pulmonologist for further management.
1. What are abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the
confirmation of the medical problem?
4. What was included in the management of this case?5. If not treated, what will be the consequences?
The function of the respiratory system is to supply body cells and tissues with oxygen
and eliminate carbon dioxide (CO2). Damage and disease in the respiratory system
greatly affect a person’s normal health function. It is a must to maintain the normal
and clear respiration, the maintenance of normal respiration and tissue oxygen
supply requires the well-functioning of airway flow. Some medical condition such as
asthma among others alter the proper respiratory pattern thus disturb an individualwellbeing.
Asthma is a chronic inflammatory disorder of the airway that causes recurrent
spasmodic episodes due to increased hyperirritability or responsiveness of the
bronchial tree to the various stimuli. It is a deterioration of the baseline asthma
control leading to acute wheeze, shortness of breath and dyspnoea. Asthma isusually a reversible obstructive disease of the lower airway.
Causes and risk factors of asthma
The asthma is chronic disease characterized by the various associated risk factors:
• Upper respiratory tract infections (viral, etc)
• Exposure to triggers (occupational exposure: working in industry, smoking,
air, pollution, cold, dust, etc)
• Stress
• Family history
• Obesity
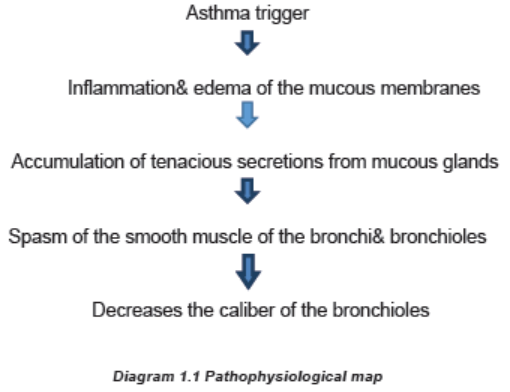
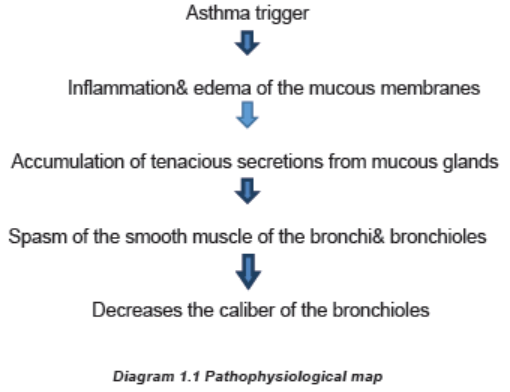
Pathophysiology overview of Asthma
The primary pathophysiologic process in asthma is persistent inflammation of the
airways which results in bronchoconstriction, airway hyper responsiveness (hyper
reactivity) and edema of the airways. The following is brief pathophysiologicalprocess of asthma development.
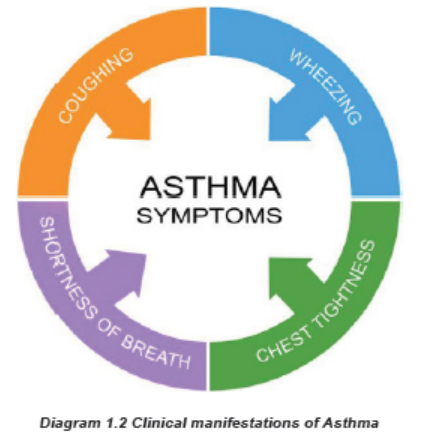
The clinical manifestations of asthma/ Signs and symptoms of asthma
The asthma symptoms are associated with shortness of breath, wheezing, mucoussecretions, cough, chest tightness, quiet chest and decreased oxygen saturation.
Investigations
The following medical investigations that are most used in diagnosis of asthma
include Laboratory (Full blood account (FBC), Immunoglobulin E); Spirometry; andImagery (chest x- ray).
Treatment plan for asthma
The goals of asthma therapy are to reduce symptoms, improve lung function, andminimize impairment of normal activity and sleep.
The goals of asthma therapy are to reduce symptoms, improve lung function, and
minimize impairment of normal activity and sleep.
Properly using asthma medication, as prescribed by the doctor, is the basis of
good asthma control, in addition to avoiding triggers and monitoring daily asthmasymptoms.
There are two main types of asthma medications:
a. Anti-inflammatories: This is the most important type of medication for most
people with asthma. Anti-inflammatory medications, such as inhaled steroids
(Beclomethazone) to reduce swelling and mucus production in the airways.
Oral steroids (Prednisolone) are taken for acute flares and help increase theefficacy of other medications and help reduce inflammation.
Possible side effects of steroids: Increased appetite, Weight gain, Changes
in mood, Muscle weakness, Blurred vision, Increased growth of body hair, Easybruising, Lower resistance to infection.
b. Bronchodilators: These medications relax the muscle bands that tighten
around the airways. This action rapidly opens the airways, letting more air inand out of the lungs and improving breathing.
The two main types of bronchodilator medicines
There are beta 2-agonists (short- and long-acting forms) and anticholinergics.
a. Short-acting beta 2-agonists (also called SABAs)
In inhaled forms, these medications include: Albuterol (Proventil® HFA, Ventolin®)
Short-acting beta 2-agonists (SABAs) are called “reliever” or “rescue” medicines
because they stop asthma symptoms very quickly by opening the airways.
They work within 15 to 20 minutes and last four to six hours. They are also the
medicines to use 15 to 20 minutes before exercise to prevent exercise-inducedasthma symptoms.
Asthma medications can be taken by inhaling the medications (using a metered
dose inhaler, dry powder inhaler, or asthma nebulizer) or by swallowing oralmedications (pills or liquids).
b. Long-acting beta-2 agonists (also called LABAs):
These medications include: Salmeterol (Serevent®), Formoterol (Foradil®),
Theophylline (Amnophylline): They contain both the long-acting beta agonistand an inhaled corticosteroid.
They are used twice a day to maintain open airways for long-term control, and they
must be used with an inhaled corticosteroid for the treatment of asthma.
Theophylline may be used to treat difficult-to-control or severe asthma and must betaken daily.
When taking theophylline, blood tests are needed to make sure you are receivingthe right amount of medicine.
Side effects include: Nausea and/or vomiting, Diarrhea and/or stomach ache,
Headache, Rapid or irregular heartbeat, Muscle cramps, Jittery or nervous feeling,hyperactivity.
c. Anticholinergic drugs
There are two anticholinergic bronchodilators currently available ipratropium
bromide (Atrovent® HFA). These are not quick-relief medications, but they can add
to the bronchodilator effect for certain asthmatics with difficult-to-control symptoms.Treatment plan of patient with asthma
• Monitor vital signs (temperature, respiratory rate, pulse, blood pressure,SP02)
• Conduct basic health assessment
• Decision making (identify disturbed patient needs)
• Ensure the client safety and quality patient care
• Collaborate with health care team (Registered Nurse (RN), Physician)
• Implement medical prescription (administration of bronchodilators and
corticosteroids, antibiotics if signs of infection, oxygen therapy if desaturating).
• Keep confidentiality of patient
• Demonstrate ethical and moral values principles while nursing care delivery
• Demonstrate effective communication skills with patient, family members and
multidisciplinary team.
Evolution and complications of asthma
Although asthma is a chronic disease with no cure, most people with mild to
moderate signs and symptoms, asthma can improve with time or go into remission
for long periods. Without treatment of asthma, the improvement can occur. Somecomplications related to asthma are:
• Severe asthma can disrupt daily life
• Sleeping disturbance
• Patient may be hospitalized
• Chronic airway inflammation/Chronic obstructive pulmonary disease
• Respiratory failure and death.
Self-assessment 1.1
Carefully read below case study and answer the following questions:
A 44-year-old woman, currently working in a bakery, presents with cough,
wheeze, shortness of breath and chest tightness with itchy red watery eyes anda stuffy, runny, itchy nose.
These symptoms become worse within 1-2 hours of starting work each day,
and worsen throughout the workweek. She especially finds red bran to worsen
her symptoms almost immediately on exposure. She notices an improvement
within 1-2 hours outside of being at her workplace. Her past medical history is
significant for seasonal allergic rhinitis in the summer months since childhood.
She is a lifelong smoker. Her family history is significant for asthma in her motherand brother.
1. According to the above signs and symptoms of patient, what is possible
medical diagnosis?
2. Describe the triggering factors contributing to the asthma development
3. What are different drugs that you can administer to this patient
4. Describe the nursing and medical management of this patient5. If this patient is not treated effectively, what could be the complications?
1.2 PNEUMONIA
Learning Activity 1.2
Read carefully the clinical case scenario below and answer the questionsthat follow.
You were going to fetch water and you meet a person who is having transpiration,
chills, coughing. While talking to him, he states that he has been in this condition
for 1 week, where he is starting to experience the productive cough like bloody
mucopurulent discharge. He has also difficulty in breathing associated withchest pain.
You accompanied him to the nearest health center. On his arrival, the vital signs
were performed and revealed respiratory rate: 36 cycles/min, Temperature: 39
Celsius degrees, pulse rate: 98 beats/min. Due to seriousness of his condition,
he has been transferred to the nearest district hospital where the medical doctor
ordered the following investigations: CBC (complete blood account) with white
blood cells of 14000/microliter (Normal 4000-11000/microliter) and chest x-ray
revealed infiltrations, blood smear was negative. His general status deteriorated
and the medical doctor decided to hospitalize the patient, ordered antibiotics
intravenous ceftriaxone 1gram BID for 7 days, oxygen therapy 3 liters/minute,
intravenous fluids therapy and required the continuous suctioning due to high
secretions causing the depletion of oxygen saturation (SPO2 of 86% on roomair, Normal value above 95-100%).
1. What are the signs and symptoms that the patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What diagnostic studies have been ordered to guide the confirmation of
that medical problem?
4. What will be included in the nursing and medical management for this
case?5. If not well treated, what will be the consequences?
The respiratory system supplies oxygen for cellular metabolic need and removes
carbon dioxide (CO2), a waste product of cellular metabolism. Respiratory disorders
and diseases are common, ranging from mild to life threatening. Disorders that
interfere with breathing or the ability to obtain sufficient oxygen greatly affect
respiratory and overall health status, the disorders that affect this system includes
inflammatory and infective disorders, the pneumonia is predominant infectivedisorder among others.
Pneumonia is an acute infection of the pulmonary parenchyma. Despite being the
cause of significant morbidity and mortality, pneumonia is often misdiagnosed,mistreated, and underestimated.
Causes of pneumonia
Pneumonia is classified according to its etiology; bacterial pneumonia is referred
to as typical pneumonia. Some of the most common causal microorganisms
include bacteria, virus, fungi. Some examples of bacterial microorganisms that may
cause pneumonia including pneumococcal pneumonia caused by streptococcus
pneumonia, staphylococcus pneumonia caused by staphylococcus aureus, gram
negative bacterial pneumonia caused by klebsiella pneumonia, anaerobic bacterial
pneumonia caused by normal oral flora. Some examples of virus that may cause
pneumonia are viral pneumonia: Influenza virus A&B adenoviruses, respiratory
syncytial virus, parainfluenza viruses. Mycoplasma: Mycoplasma pneumonia: by
mycoplasma microorganism. Fungal agents: Fungal pneumonia: by histoplasmosis,
candidiasis. Protozoa: Parasitic pneumonia, common organism is pneumocystis
carinii.
Nosocomial pneumonia is acquired within a hospital to the patient admitted to
the hospital for something else. Risk increased with an underlying illness, recent
surgery, recent intubation, and in persons already on antibiotics.
The following are some risk factors for pneumonia: advanced age,
immunocompromised, underlying lung disease, alcoholism, altered consciousness,
smoking, endotracheal intubation, malnutrition, immobilization, most cases of
pneumonia are preceded by an upper respiratory infection (often viral).
Pathophysiology overview of pneumonia
Pneumonia results from the proliferation of microbial pathogens at the alveolar
level and the host’s response to those pathogens. Many pathogens are inhaled as
contaminated droplets.
When microorganisms evade upper respiratory defense mechanisms, the alveolar
macrophage is capable of removing most infectious agents without triggering
a significant inflammatory or immune response. However, if the microbe is
virulent or present in sufficiently high numbers, it can overwhelm macrophages
and result in a full-scale activation of systemic defense mechanisms. These
mechanisms include the release of multiple chemical mediators of inflammation,
infiltration of white blood cells, and activation of the immune response.
Tight adherence of some bacteria (e.g., Pseudomonas) to the tracheal lining and biofilm
of an endotracheal tube makes clearance of these microbes from the airways
difficult and accounts, in part, for their highly virulent nature. In non-hospitalized
people, bacteria reach the lung by one of four routes:
• Inhalation of microorganisms that have been released into the air when an
infected individual coughs or sneezes
• Aspiration of bacteria from the upper airways
• Spread from contiguous infected site
• Hematogenous spread
Signs and symptoms of pneumonia
Symptoms vary for the different types of pneumonia. The onset of bacterial
pneumonia is sudden. The client experiences fever, headache, myalgia, arthralgia,
chills, chest pain, a productive cough (mucoid, purulent, bloodstained sputum),
dry cough, dyspnea, tachypnea, and hemoptysis and discomfort in the chest wall
muscles from coughing. 20% of patients may have gastrointestinal symptoms such
as nausea, vomiting, and/or diarrhea. Physical examination: Dullness to percussion,
crackles, egophony, individuals also may demonstrate signs and symptoms of
underlying systemic disease or sepsis and decreased level of consciousness.
Pneumonia can be categorized into 3 types:
• Community Acquired Pneumonia (CAP) caused by Streptococcus
pneumonia, Haemophilus influenza, Legionella pneumophila, Mycoplasma
pneumonia, Influenza virus types A, B, adenovirus, parainfluenza,
cytomegalovirus, coronavirus, Chlamydia pneumonia.
• Hospital Acquired Pneumonia (HAP) caused pseudomonas aeruginosa,
Staphylococcus aureus, Klebsiella pneumonia.
• Pneumonia in Immunocompromised Host caused by Pneumocystis carinii,
Aspergillus fumigatus, Mycobacterium tuberculosis.
Investigations
The sputum culture and sensitivity studies can help to identify the infectious
microorganism. A chest film (chest x-ray) shows areas of infiltrates and consolidation.
A complete blood count (CBC) discloses an elevated with Blood Cells (WBC) count.Blood cultures also may be performed to rule out any microorganisms in the blood.
Figure 1.4 Sample chest x-ray of the lungs, lung A revealed the normal lung while Lung B shows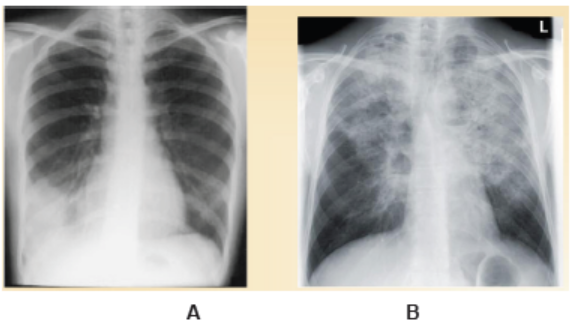
abnormal lung image.
Adequate medical diagnosis
The auscultation of the chest reveals wheezing, crackles, and decreased breath
sounds. Cyanosis of nail beds, lips, and oral mucosa may be observed duringphysical examination (inspection).
The most common investigations to be carried out during pneumonia suggests
the chest x-ray, the biological laboratory tests needed to be performed such as full
blood count (FBC) elevated (more than10000/mm3), although it may be low (below
6000/mm3) if the individual is debilitated. Sputum: Gam-stain and culture, blood
culture, Chest x-ray show infiltrates that may involve a single lobe of the lung (lobarpneumonia) or may be more diffuse (bronchopneumonia).
Treatment plan for pneumonia
Medical management of bacterial pneumonia consist of initiating antibiotic therapy,
hydration to thin secretions, supplemental oxygen to alleviate hypoxemia, bed
rest, chest physical therapy and postural drainage, bronchodilators, analgesics,
antipyretics, and cough expectorants or suppressants depending on the nature ofthe client’s cough chest physiotherapy and postural drainage.
The following are different treatment options:
• Antibiotics in case of bacterial pneumonia such as a macrolide (clarithromycin/
Erythromycin or Doxycycline.
• In case of comorbidities or antibiotics in past 3 months: High dose Amoxicilline
or Ceftriaxone plus Macrolide/ doxycicline
• In case of hospitalization: Cefotaxime or Ceftriaxone or Ampicillin plus a
macrolide/ doxycline
• Supportive therapy in case of viral pneumonia
• Adequate hydration
• Good pulmonary hygiene (deep breathing, coughing, chest physical therapy)
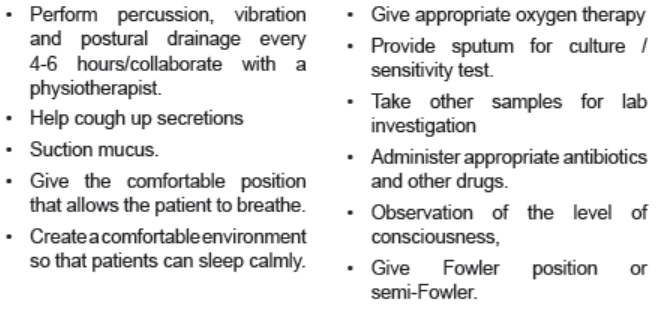
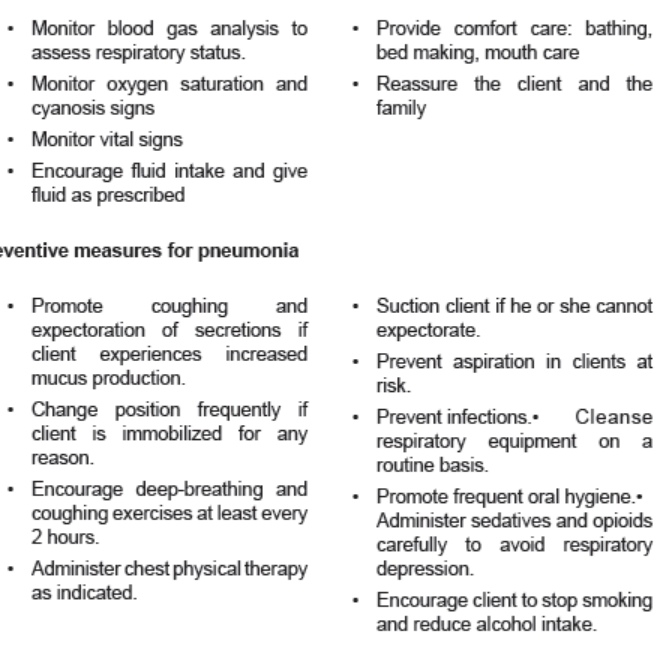
The nursing management of pneumonia depends on the degree of which upon the
patient is admission. The nurse auscultates lung sounds and monitors the client
for signs of respiratory difficulty. He or she checks oxygenation status with pulse
oximetry. Assessments of cough and sputum production also are necessary. The
nurse places the client in the semi-Fowler’s position to aid breathing and increase
the amount of air taken with each breath. Increased fluid intake is important to
encourage because it helps to loosen secretions and replace fluids lost through
fever and increased respiratory rate. The nurse monitors fluid intake and output,
skin turgor, vital signs, and serum electrolytes. He or she administers antipyreticsas indicated and ordered
Evolution and complications of pneumonia
When pneumonia is early and managed effectively, the outcome is observed in fewdays. However, in case of late management the following complications may occur:
• Pleural effusion
• Lung abscess
• Respiratory failure
Self-assessment 1.2
1. Describe the different causes of pneumonia
2. Explain the overview pathophysiology of pneumonia
3. Outline the signs and symptoms of pneumonia
4. List the investigations that should be ordered for confirming pneumonia
5. What is the treatment plan of patient with pneumonia?
6. What are the complications of pneumonia?
1.3 BRONCHIOLITIS
Learning Activity 1.3
Read carefully this below situation and answer the following questions:
A 5-month-old boy presents with a 3-day history of cough, rhinorrhea, congestion,
and fevers. Today his mother noticed he was breathing faster and taking in less
formula than normal. His 4-year-old sister has a cold and he attends a local
day care. On physical exam, the boy’s temperature is 102.5°F (39°C), heart
rate is 140beats per minute, respiratory rate is 60 breaths per minute, and
blood pressure is 90/50mmHg. His oxygen saturation is 95%. He appears alert
and smiling but is tachypneic and coughing. He has subcostal and intercostal
retractions. On auscultation of his lungs, wheezing is heard on both inspirationand expiration. The complete blood count was performed and revealed normal.
1. What are the abnormal clinical manifestations can you identify from above
scenario?
2. What do you think is the medical condition the boy is presenting?
3. List the causes and risk factors contributing to the development of the
identified medical condition.
4. Outline the treatment modalities of the above medical condition.
5. Describe the preventative measures that will be advised to the family to
avoid cross-contamination.
Bronchiolitis is a common lower respiratory tract infection that affects babies and
young children. The early symptoms are similar to those of a common cold, such
as runny nose or cough.
Causes of bronchiolitis
Bronchiolitis is usually caused by a viral infection. Many different viruses can be the
culprit, including the flu, but the most common in children is what’s called respiratorysyncytial virus.
Outbreaks of this virus happen every winter. They may only get mild symptoms, butin severe cases it can cause bronchiolitis or pneumonia
Pathophysiology overview
The pathophysiology of bronchiolitis begins with an acute infection of the epithelial
cells lining the small airways within the lungs. Such infection results in edema,increased mucus production, and eventual necrosis and regeneration of these cells.
The inflammation, edema, and debris result in obstruction of bronchioles, leading
to hyperinflation, increased airway resistance, atelectasis, and ventilation-perfusion
mismatching. Bronchoconstriction has not been described. Infants are affected
most often because of their small airways, high closing volumes, and insufficient
collateral ventilation. Recovery begins with regeneration of bronchiolar epithelium
after 3-4 days; however, cilia do not appear for as long as 2 weeks. Mucus plugsare instead predominantly removed by macrophages.
The pathogenesis of bronchiolitis involves a combination of airway edema,
increased mucus production, and necrosis of airway epithelial cells due to direct
cytotoxic injury. Respiratory syncytial virus transmission occurs from person to
person either by direct inoculation of nasal mucosa with contaminated secretions
or by inhalation of large infectious droplets. Virus replicates in the nasal epithelium,
and an exaggerated immune response occurs, with an influx of natural killer cells,
lymphocytes, and granulocytes into the epithelium. After an incubation period of 4
to 6 days from transmission, upper respiratory tract symptoms appear, includingnasal congestion and rhinorrhea.
Signs and symptoms
The most common signs and symptoms of bronchiolitis are: runny nose, fever,
stuffy nose, loss of appetite and cough are the first signs of the infection. Symptoms
may worsen after a few days and may include wheezing, shortness of breath, andworsening of the cough. The child might show more severe signs, including:
• Making grunting noises.
• Having trouble sucking and swallowing, this makes feeding difficult on top of
having a poor appetite.
• Trying so hard to breathe that the chest retracts (the skin is drawn down
tightly against the rib cage and looks like it is going inward).
• Turning blue or gray in the lips, fingertips or toes.• Being sluggish.
Investigations
The diagnosis of bronchiolitis is mainly based on clinical manifestations. Pulseoximetry is useful if hypoxia is suspected. It is not unusual for these infants to
experience mucous plugs leading to hypoxia. If supplemental oxygen is required,
the goal should be to maintain saturation levels between 90 and 100%.
Beyond the physical exam, the following diagnostic tests might be done:
• Laboratory: Full blood count (FBC), white blood cells are increased (Normal
range: 4000-11000/mm3), chain reactive protein might be positive and
increased (Normal range: 6.8-820 mcg/dL), neutrophils are increased (Normal
range: 0-8%), increased erythrocyte sedimentation rate (Normal value: <30
mm/hr).
• Chest Radiograph: A chest radiograph is indicated if pneumonia, a chest
mass, a foreign body, or heart failure are suspected. In bronchiolitis, the
radiograph may show hyperinflation or scattered areas of atelectasis. This is
can be misinterpreted as bacterial pneumonia.
• Nasal Specimen: A nasal aspirate for antigen detection of respiratory
syncytial can be performed. Influenza A and B and adenovirus can also be
detected by this method.
Adequate medical diagnosis of bronchiolitis
The diagnosis of bronchiolitis is made primarily based on history and physical
examination findings. A mucus sample test (where a sample of mucus from your
child’s nose will be tested to identify the virus causing their bronchiolitis) urine or
blood tests. A pulse oximeter test (where a small electronic device is clipped to the
child’s finger or toe to measure the oxygen in their blood) must be performed.Treatment plan of bronchiolitis
The physician has the role to diagnose and prescribe the medication according
the signs and symptoms, also the results of investigation done; the physician
orders the following medications according the medical decision and guideline:
Bronchodilators. Bronchodilators are frequently tried in infants presenting with
wheezing due to bronchiolitis because of its similarity to asthma, Anticholinergicagents, Corticosteroids, Ribavirin, Antibiotics, Surfactant, Heliox.
Treatment at home:
• Keep the child upright. Keeping the child upright may make it easier for them
to breathe, which may help when they are trying to feed.
• Make sure the child drinks plenty of fluids.
• Do not smoke at home.
• Relieving a fever.
• Saline nasal drops.
Symptomatic care: There is no cure for bronchiolitis, so treatment is aimed atthe symptoms (eg, difficulty breathing, fever). Treatment at home usually includes
making sure the child drinks enough and saline nose drops (with bulb suctioningfor infants).
The nurse carries out the following activities at hospital: Provide oxygen if saturations
are low, Assist with oral hydration, Listen to the lungs, Monitor oxygenation, Assess
vitals, Intake and output, IV (intravenous) fluids if your child can’t drink well, Extra
oxygen and a breathing machine (ventilator) to help with breathing, Frequent
suctioning of the child’s nose and mouth if respiratory tract secretions, Breathingtreatments, as ordered by your child’s healthcare provider.
Evolution and complications of bronchiolitis
In most cases, the disease is mild and self-limited. With bronchiolitis, as any other
diseases, various complications are possible. If the child develops complications from
bronchiolitis, it’s likely that they’ll need hospital treatment. Potential complicationsof bronchiolitis include:
• Cyanosis (a blue tinge to the skin caused by a lack of oxygen)
• Dehydration (when the normal water content of the body is reduced)
• Fatigue (extreme tiredness and a lack of energy)• Severe respiratory failure (an inability to breathe unaided)
Self-assessment 1.3
Carefully read the following case scenario and answer the followingquestions:
J.N is a 5-month-old previously healthy boy who presents today with a 3-day
history of cough, runny nose and fever. His mother brought him into the
emergency department because since this morning he has been sleepy and
not interested in feeding. He has no significant gestational or birth history, and
is meeting his developmental milestones, but of note, he is bottle-fed. He is upto-
date on his immunizations. The only other significant detail is that his older
sister was home sick from daycare last week. On exam, his heart rate is 120
beats/minute, his respiration rate is 60 breaths /minute, and his temperature
is 39°Celsius and oxygen saturation (88 %). His weight is 7kg. He has signs
of respiratory distress and on auscultation; bilateral wheeze and crackles, andnasal flaring was observed.
1. After reading the above situation, identify the signs and symptoms that
present this patient.
2. Basing on clinical manifestations of J.N, what could be the medical
diagnosis?
3. Briefly, describe the pathogenesis of the medical diagnosis?
4. What are the most common causes of J.N medical condition?
5. What are investigations might be ordered to J.N?
6. What is the medical and nursing management of J.N medical condition?
7. What are the most complications that might occur to J.N if it’s poorlymanaged?
1.4 END UNIT 1 ASSESSMENT
End unit 1 assessment
Section A: Multiple Choice Questions
Circle the letter that corresponds to the best answer for each question
1. Pneumonia is infection of the lungs caused by :
a. Bacteria
b. Virus
c. Fungid. All the above
2. Nosocomial pneumonia is pneumonia that is acquired from:
a. The community
b. Hospital environment
c. Within the place of residenced. From the neighbors at home
3. Pneumonia that develops following passage of food particles, drink etc.
into the lungs is called:
a. Community acquired pneumonia
b. Aspiration pneumonia
c. Atypical pneumoniad. None of the above
4. Which of these causes atypical pneumonia?
a. Pneumococcus
b. Mycoplasma
c. Influenza virusd. Respiratory Syncytial Virus
5. …………………is a common lung infection in young individuals
a. Bronchiolitis
b. Pneumonia
c. Bronchitisd. Asthma
6. ……………is inflammation of the bronchioles usually caused by an acute
viral
a. Asthma
b. Bronchitis
c. Pneumoniad. Bronchiolitis
7. Which of the following is correct regarding bronchiolitis?
a. It is more common in the summer months.
b. Parainfluenza virus is the commonest cause.
c. The disease is most common in children aged 2-4 months.d. Wheezing is a highly specific symptom for bronchiolitis
8. The following are known to cause bronchiolitis in infants EXCEPT:
a. Para influenza
b. Chlamydia
c. Mycoplasmad. Streptococcus pneumonia
9. Symptoms included in a written asthma action plan that would prompt
the use of reliever therapies include all of the following EXCEPT
a. Chest tightness
b. Hemoptysis
c. Wheezingd. Persistent Cough
10. What is a common symptom of asthma?
a. Wheezing
b. Full breaths
c. Snoringd. Crackles
11. What is the cure for asthma?
a. There is no cure of asthma
b. It depends on the patient
c. It depends the drugs administeredd. It depends the triggers
12. In providing patient education, which of the following has been shown to
result in emergency care utilization?
a. Teaching about the pathophysiology of asthma
b. Teaching self-management skills
c. Teaching inhaler techniqued. Teaching about the pharmacology of the drugs
13. Asthma is characteristically defined by the following triad:
a. Airway inflammation
b. Airway hyper-responsiveness
c. Reversible airflow obstructiond. Reversible airflow constriction
14. Normal pulse oximeter readings usually range from:
a. 95 to 100 percent
b. 90 to 95 percent
c. 85 to 90 percentd. 80 to 85 percent
a. Which of the following statement about Salmeterol is not true?
a. It acts by relaxing muscles in the airways to improve breathing
b. It is a short-acting selective β2 agonist
c. Salmeterol inhalation is used to prevent asthma attacks
d. Salmeterol inhalation is used to treat COPD including emphysema andchronic bronchitis
15. ……………is a bronchodilator that relaxes muscles in the airways and
increases air flow to the lungs.
a. Ventolin (albuterol)
b. Beclomethasone dipropionate (Qvar)
c. Budesonide (Pulmicort)d. Budesonide/Formoterol (Symbicort)
16. These are Anti-inflammatory medications reduce swelling and mucus
production in the airways EXCEPT
a. Beclomethasone dipropionate (Qvar)
b. Budesonide (Pulmicort)
c. Budesonide/Formoterol (Symbicortd. Theophylline
17. Side effects of beta 2-agonists include EXCEPT:
a. Increased heart rate.
b. Upset stomach (rare).
c. Trouble sleeping (rare).d. Increased appetite.
18. Bronchodilators are the most effective treatment for asthma (True or Fal
se)
19. Cough can be the only presenting complaint in patients with asthma (
True or False)
20. Asthma is a chronic respiratory disease (True or False)
21. People with reduced immunity tend to suffer from a more severe form of
pneumonia (True or False)
22. The cough in bacterial pneumonia is a dry type of cough (True or False)
23. Pneumonia can be prevented by vaccination (True or False)
Section B: Short Answer Questions
1. Define asthma and its clinical features.
2. How to diagnose pneumonia?
3. Explain the pathophysiology of asthma.
4. What is treatment plan of patient with bronchiolitis?5. What is treatment plan of pneumonia?
UNIT 2 PATHOLOGIES OF CARDIOVASCULAR SYSTEM
Key unit Competencies
Take appropriate decision on different common medical pathologies of cardiovascularsystem.
Introductory Activity 1.0
Observe the following schematic representation that shows the connectionbetween the heart and blood vessels and answer the following questions:
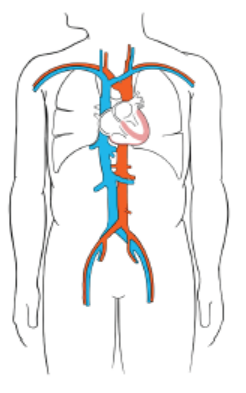
Figure 2.1 Blood Circulation system.
1. Basing on anatomy and physiology of the heart and circulatory system you
learnt, what do you think may happen to the human being if the required
cardiac output for better function of entire parts of the body changes are
noted?
2. What might be your interventions towards a patient with abnormal (lowand high) cardiac output?
1.1 HYPOTENSION
Learning Activity 2.1
Read carefully the case below and answer following questions:
A 52 years old female patient presented with general weakness, headaches and
occasional dizziness for the past three months. She had also had occasional
abdominal discomfort, moderate anorexia and weight loss due to nausea. She
tired more easily than before. She seemed frustrated and concerned about her
condition. During the examination, the blood pressure was 94/55 mmHg (Normal
systolic BP: 90-120mmHg/60-90 mmHg)), a regular pulse rate of 97 beats
per minute (Normal pulse 60-80 beats per minute), and a normal abdominal
examination. She was treated by some non-steroids anti-inflammatory drugs torelieve headache and sent back home.
During the following week, she continued to have same clinical manifestations
and decided to go back at health care setting. At arrival, blood pressure recheck
confirmed a significant drop from 94/55mmHg to 84/45mmHg. She also continued
to have headache associated with blurred vision. She was at that moment
unable to stand due to dizziness, severe headache and body weaknesses.
Her laboratory investigations revealed normal complete blood count with Hb:
12.5mg/dl (Normal value Hb: 11-16mg/dl), ASAT: aspartate aminotransferasee:
20U/l (Normal value: 10-30U/l), ALAT: alanine aminotransferase: 28U/l (10-40U/
l), creatinine: 0.8mg/dl (0.2-1mg/dl). The decision of hospitalizing her was taken,
prescribed the paracetamol 500mg three times per day for 3 days (painkiller)
and Ringer lactate and Normal saline 1.5 liter/24 hours (intravenous fluids)
and planned for further investigations to look for all possible causes of those
persistent signs and symptoms.
1. What are the abnormal signs and symptoms that the patient was
presenting?
2. From the case scenario, identify different investigations that have been
requested and their results?
3. Basing on those signs and symptoms, what could be the medical problem
of this patient?
4. What will be included in the medical and nursing management of this
case?5. If not treated, what will be the consequences?
The function of the cardiovascular system is to supply body cells and tissues with
oxygen-rich blood and eliminate carbon dioxide (CO2) and cellular wastes. Damage
and disease in the cardiovascular system greatly affect a person’s health and the
entire parts of his/her body. Cardiovascular diseases are conditions and diseases
that affect the heart and vasculature (blood vessels).
A good blood circulation requires the good cardiac output related to the capacity
of the heart to pump and the normal functionality of blood vessels that determine
the peripheral resistance. Blood pressure is the force exerted by the blood from
the heart against the walls of the blood vessels. It must be adequate to maintain
tissue perfusion during activity and rest. The maintenance of normal blood pressure
and tissue perfusion requires the integration of both systemic factors and local
peripheral vascular effects. Blood pressure is primarily a function of cardiac output
and systemic vascular resistance. Any condition that can have an impact on thesetwo aspects might have an impact on the blood pressure.
Hypotension is a decrease in systemic blood pressure below accepted values.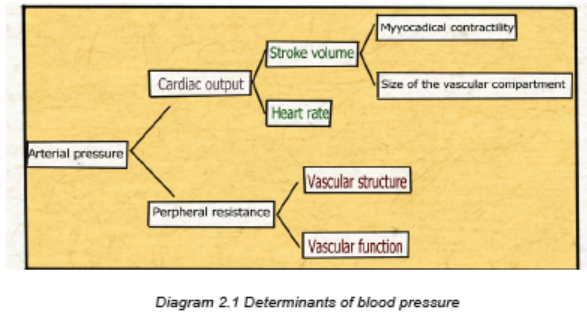
Even though there is no accepted standard hypotensive value, the blood pressure
less than systolic of 90-120mmHg/diastolic of 60-90mmHg is considered as
hypotension. The hypotension becomes a concern once pumping pressure is not
sufficient to perfuse key organs with oxygenated blood. This leads to symptomsimpacting the quality of life of a patient.
Causes and Pathophysiology
Blood pressure is determined by 2 major factors: cardiac output and total peripheral
vascular resistance. The cardiac output is determined by stroke volume and heart
rate. Therefore, any disease or pathology that impacts one or more of these factors
will induce hypotension.
Disease that reduces stroke volume or heart rate will decrease the total cardiacoutput of the heart, therefore decreasing the ability to generate blood pressure.
Some medications including diuretics, calcium channel and beta blockers can
cause hypotension by having impact on stroke volume and heart rate.
A combination of the weakened autonomic nervous system and mild hypovolemia
from dehydration causes orthostatic hypotension. When lying flat, there is equal
and smooth distribution of fluid throughout the body. However, on standing the
heart rate fails to increase appropriately and peripheral resistance fails to increase
appropriately leading to a rapid, transient decrease in blood pressure that improves
with postural changes, then classic symptoms like dizziness and syncope occur.
Certain conditions can cause prolonged periods of hypotension that can become
dangerous if left untreated: pregnancy, due to an increase in demand for blood
from both mother and the growing fetus; large amounts of blood loss through injury;
impaired circulation caused by heart attacks or faulty heart valves, weakness and
a state of shock due to dehydration, anaphylactic shock due to a severe form
of allergic reaction, infections of the bloodstream, endocrine disorders such as
diabetes, adrenal insufficiency and thyroid disease. Nutrient deficiency like lack of
vitamin B12 and folate can cause low blood pressure due to reason that nutrients
are essential to produce the red blood cells and their deficiency can lead to drop in
blood pressure levels.
Hypotension as a result of troubles of the factors determining the blood pressure,
when persistent the patient might be into different types of shock:
Distributive shock occurs as a failure of the ability to maintain total peripheral
resistance with maintained cardiac function attempting to compensate. This is
associated with anaphylactic allergic reactions and septic shock.
Cardiogenic shock is a failure to achieve sufficient cardiac output with maintained
total peripheral resistance.
Hypovolemic shock is a loss of total blood volume such that a blood pressure is
not maintained. Both cardiac output and total peripheral vascular resistance are
maintained. This is possible due to trauma with massive loss of blood, overuse of
diuretic medications with fluid volume loss via urine, burns, diarrhea and vomiting,
hemorrhage, etc.
Obstructive shock occurs with the obstruction, constriction, or compression of the
cardiovascular system such that blood flow does not efficiently occur or there is adecrease in stroke volume of the heart. This leads to drop in blood pressure.
Signs and symptoms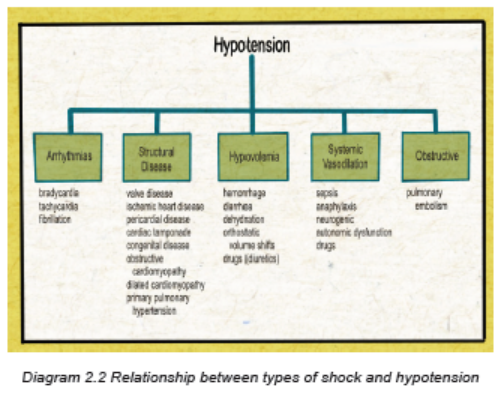
Patient with hypotension is most commonly asymptomatic. The chronic asymptomatic
hypotension isn’t usually harmful. But there are possibilities that sudden drop in
blood pressure may develop several health problems. The most common symptoms
are lightheadedness or dizziness. In extreme low blood pressures, syncope may
occur. Other symptoms are possible which typically begin from the underlying
etiology rather than hypotension itself. They may include chest pain, shortness of
breath, irregular heartbeat, headache, fatigue and weakness, pale skin color, rapid
breathing, blurred vision, fainting when having syncope, nausea, rapid pulse rate,etc.
Investigations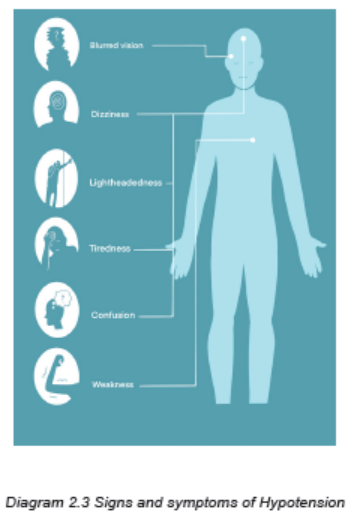
The investigations to be requested depend on the suspected cause. Basic lab work
including complete blood count (CBC), cardiac enzymes, renal function tests (urea
and creatinine), liver function tests, blood smear for malaria, blood sugar levels,
electrolytes (sodium, potassium, chloride, calcium, etc). If a patient present signs
and symptoms of shock, all these investigations must be ordered among others:
chest x-ray, electrocardiogram, blood culture, urine culture, ultrasound of the heart,
chest computerized tomography scan with angiography, etc).
Adequate Medical diagnosis
The diagnosis of hypotension requires relying on clinical manifestations supported
by laboratory and imaging investigations, and hemodynamic findings. Imaging or
hemodynamic indices of low cardiac output or systemic vascular resistance are not
diagnostic but may help to classify hypotension.
Treatment plan
Asymptomatic hypotension patient should not receive extreme interventions.
However, if symptoms are present, the treatment of hypotension should focus on
reversing the underlying etiology. The management must focus on:
• Patients should be assessed (monitoring of all vital signs) for possible need
for an immediate intervention so that lifesaving therapies can be administered
very early. After immediate stabilization, the comprehensive physical
examination must be followed.
• The airway should be stabilized and adequate intravenous access secured
so that patients can be immediately treated with intravenous fluids to restore
adequate tissue perfusion. The first priorities must be focused on the airway
and breathing with oxygen and/or mechanical ventilation, when necessary;
and insertion of intravenous catheter and IV fluids (Normal saline or Ringer
lactate) must be initiated to restore adequate tissue perfusion.
• Ensure the investigations needed are done to investigate the suspected
cause of hypotension
• Monitoring the inputs and outputs
• Treat underlying medical conditions, and this should include medications for
heart disease, diabetes, or infection. Patients with suspected infection (eg,
fever, hypotension, and a suspected septic source) must benefit from the
early administration of intravenous antibiotics.
• Shock-induced hypotension is the most serious form of the condition. Severe
hypotension must be treated immediately, should give IV fluids and possibly
blood products to increase the blood pressure and stabilize the vital signs and
hemodynamic status.
• Advise the patient to drink plenty of water to avoid hypotension due to
dehydration, especially if you are vomiting or have diarrhea. Staying hydrated
can also help treat and prevent the symptoms of mediated hypotension. If
you experience low blood pressure when standing for long periods, be sure
to take a break to sit down. And try to reduce your stress levels to avoid
emotional trauma.
• Treat orthostatic hypotension with slow, gradual movements. Instead of
standing up quickly, work your way into a sitting or standing position using
small movements. Avoid orthostatic hypotension by not crossing the legs
when you sit.
• Exercise regularly aiming at raising the heart rate and resistance exercises
two or three days a week.Evolution and complications
The prognosis of hypotension is very good, but symptomatic hypotension might
have variable prognosis depending on the etiology and its severity.
Some complications resulting from Hypotension are:
• Shock depending on etiology of hypotension
• Injury resulting from falls due to fainting. Falls are particularly dangerous
because they cause other secondary injuries (fractures, lacerations, wounds,
limited movements, etc.) that might have an impact on a person’s quality of
life.
• Severe hypotension deprives the body of oxygen, which can damage the
heart, brain, kidney and other organs (multiple organ dysfunction); and thiscondition can be life threatening if not immediately treated.
Self-assessment 2.1
1. What are the signs and symptoms of hypotension?
2. What are the possible causes of hypotension?
3. What are the investigations for the patient with hypotension?
4. What is the most appropriate treatment for hypotension?
CASE STUDY
Carefully read the case scenario below and answer the following
questions:
K.L., a 25 year old man, was not wearing his seat belt when he was the driver
involved in a motor vehicle crash.
K.L. was found 10 meters away from his car and was crying. His wife and daughter
were found in the car with their seat belts on. They sustained no serious injuries,
but were upset. All passengers were taken to the emergency department. He
states that he can’t breathe and cries when abdomen is palpated. His vital signs
were: temperature of 37.6oC blood pressure of 80/56 mm Hg; apical pulse 138 but
no palpable radial or pedal pulses; carotid pulse present but weak. Respiratory
rate 38 cycles/min; oxygen saturation of 86% on room air and asymmetric chest
wall movement; he had slight distended and left upper quadrant pain on the
abdomen. He had open wound of the lower left leg.
1. What is the medical condition is K.L. experiencing?
2. What clinical manifestations did he display that support your answer?
3. What would be included into this patient’s comprehensive assessment?
4. What investigations would you advise to be done to K.L to confirm the
medical condition? Justify the rationale of them.
5. What are the nursing interventions towards for K.L. medical condition?
6. After stabilization of K.L, what will be included into his medical and nursing
management?7. What are the possible complications related to K.L medical condition?
2.2 HYPERTENSION
Learning Activity 2.2
H.E. is a 45-years-old man with 88Kgs and 1.60m (obese) presented at a health
clinic and was found having the blood pressure of 170/95 mmHg (Normal BP:
90-120mmH/60-90mmHg). His father died of stroke at age 80 years; the mother
is alive but has hypertension. He states that he feels fine except the headache,
dizziness, chest pain especially during physical activities. He smokes one pack
of cigarettes daily for the past 28 years. He drinks 1-2 bottles of beer on most
Friday and Saturday nights. From the Laboratory investigations, he had full blood
count with Hb of 14mg/dl (Normal range 11-16 mg/dL), triglycerides of 350mg/
dl (Normal value: <150 mg/dL), sodium of 143 mEq/l (Normal range: 135-145
mEq/l). His care provider prescribed the hydrochlorothiazide 12.5 mg/day and
gave him the appointment to come back at clinic once a month.
1. From the case described above, what are the abnormal signs and
symptoms was he presenting?
2. What type of information you may ask the patient, family members to
guide in diagnosis?
3. What do you think is the medical condition of H.E?
4. Enumerate all risk factors that predisposed H.E for developing that
medical condition.
5. What are the investigations that have been requested to H.E?
6. What are different medical and nursing management options are effective
in managing H.E medical condition?
7. H.E. wants to know the most effective preventive strategies for lifestyles
changes to lower his blood pressure. What will be the content of lifestyles
modifications would you tell him?
8. What do you think will happen to H.E if there is poor adherence toprescribed treatment regimen?
The blood pressure reflects the ability of the arteries to stretch and fill with blood,
the efficiency of the heart as a pump, and the volume of circulating blood. Blood
pressure is affected by age, body size, diet, activity, emotions, pain, position,
gender, time of day, and disease states.
All these factors can have an impact on lowering or increasing the blood pressure.
Hypertension, or high blood pressure, is an important medical and public health
problem.There is a direct relationship between hypertension and cardiovascular disease.
Hypertension is a repeatedly elevated blood pressure exceeding the 90-120mmHg
as systolic and 60-90mmHg of diastolic pressure. When measuring the blood
pressure, we are looking for the pressure during systole and diastole, and is
expressed as a fraction. The top number is the systolic blood pressure; the bottomnumber is the diastolic blood pressure.
A. Systolic Blood Pressure
Systolic blood pressure is determined by the force and volume of blood that the left
ventricle ejects during systole and the ability of the arterial system to distend at thetime of ventricular contraction.
B. Diastolic Blood Pressure
Diastolic blood pressure reflects arterial pressure during ventricular relaxation
where the heart is being filled by blood either from his automatism functionality orfrom venous return.
Classification of blood pressure for Adults age 18 years or older
The term hypertension, sustained elevations in systolic or diastolic blood pressure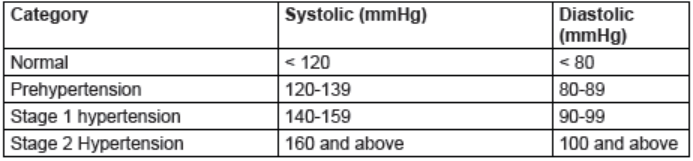
that exceed prehypertension levels, is divided into two categories:
Stage 1 hypertension: is systolic blood pressure of 140 to 159 mm Hg or a diastolic
blood pressure between 90 and 99 mm Hg.
Stage 2 hypertension: is systolic blood pressure that equals or exceeds 160 mmHg or a diastolic pressure that equals or exceeds 100 mm Hg.
Other terminologies:
When elevated blood causes a cardiac abnormality, the term hypertensive heart
disease is used. When vascular damage is present without heart involvement, theterm hypertensive vascular disease is used.
When both heart disease and vascular damage accompany hypertension, theappropriate term is hypertensive cardiovascular disease.
Causes and pathophysiology overview
A. Causes and Risk Factors
Basing on causes and risk factors, hypertension is divided into two main categories:
essential (primary; idiopathic) and secondary.
Primary (essential or idiopathic) hypertension: represent about 90-95% of all
hypertension cases. It is sustained elevated blood pressure with no known cause.
Although the exact cause of primary hypertension is unknown, there are several
contributing factors which include increased sympathetic nervous system activity,
overproduction of sodium-retaining hormones and vasoconstricting substances,
increased sodium intake, overweight, diabetes mellitus, tobacco use, and excessivealcohol consumption.
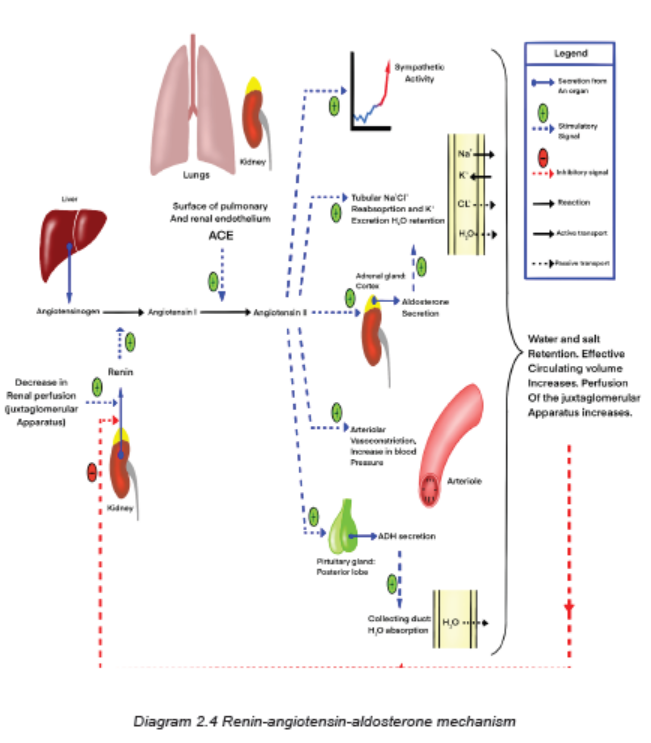
Essential hypertension also may develop from alterations in other body chemicals
such as defects in blood pressure regulation resulting from an impairment in the
renin-angiotensin-aldosterone mechanism.
Secondary hypertension: is elevated blood pressure with a specific cause that often
can be identified and corrected. It results from some other disorders such as kidney
disease, pheochromocytoma (a tumor of the adrenal medulla), hyperaldosteronism
(increased secretion of mineral corticoid by the adrenal cortex), atherosclerosis,
use of cocaine or other cardiac stimulants (e.g., weight-control drugs, caffeine), and
use of oral contraceptives. This type of hypertension accounts for 5% to 10% of all
hypertension cases. It should be suspected in people who suddenly develop high
blood pressure, especially if it is severe.
Treatment of secondary hypertension is aimed at removing or treating the underlying
cause. Secondary hypertension is a contributing factor to hypertensive crisis.
Hypertension is the most prevalent modifiable risk factor for most of cardiovascular
diseases, being more common than cigarette smoking, dyslipidemia, or diabetes,
which are the other major risk factors. Hypertension often coexists with these other
risk factors as well as with overweight/obesity, an unhealthy diet, and physical
inactivity. The presence of more than one risk factor increases the risk of adversecardiovascular events.
B. Pathophysiology Overview
Hypertension results from a sustained increase in peripheral resistance (arteriolar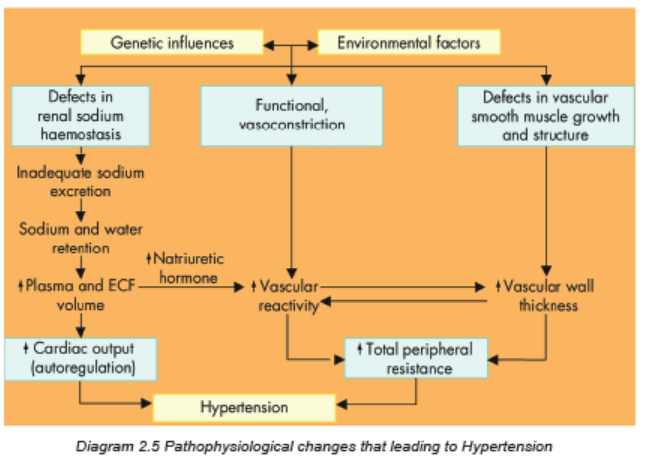
vasoconstriction), an increase in circulating blood volume, or both. Chronic
hypertension damages the walls of systemic blood vessels.Signs and symptoms
Hypertension is often called the silent killer because it is frequently asymptomatic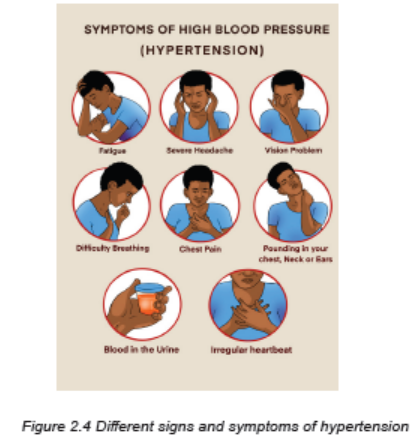
until it becomes severe and targeted organ disease occurs. A patient with severe
hypertension may experience a variety of symptoms secondary to the effects on
blood vessels in the various organs and tissues or to the increased workload of
the heart. These secondary symptoms include fatigue, dizziness, palpitations,
angina/chest pain, and dyspnea. Headache, nosebleeds and bleeding from other
organs might come when the blood pressure is very high. However, patients with
hypertensive crisis may experience severe headaches, dyspnea, anxiety, and
nosebleeds.
Investigations
Most hypertension is not classified as primary hypertension, testing for secondary
causes should be routinely done. Basic laboratory studies are performed to:
• Identify or rule out causes of secondary hypertension,
• Evaluate target organ disease,
• Determine overall cardiovascular risk, or
• Establish baseline levels before initiating therapy.
Basic diagnostic studies performed in a person with hypertension are the following:
1. Full blood count (FBC) to assist in establishing the baseline levels before
initiating the therapy or detect infection if any.
2. Routine urinalysis, bilirubin urea and nitrogen (BUN), liver function tests
(ASAT, ALAT) and serum creatinine levels used to screen for renal and
liver involvement and to provide baseline information about kidney and liver
function.
3. Measurement of serum electrolytes (sodium, potassium, chloride), especially
potassium, is important to detect hyperaldosteronism, a cause of secondary
hypertension.
4. Blood glucose levels (serum glucose) assist in the diagnosis of diabetes
mellitus.
5. A lipid profile (total lipids, triglycerides, cholesterol) provides information
about additional risk factors related to atherosclerosis
6. Uric acid levels establish a baseline, since the levels often rise with diuretic
therapy.
7. An electrocardiogram (ECG) provides baseline information about cardiac
status. It can identify the presence of cardiac ischemia, or previous
myocardial infarction, etc.
8. Ophtalmic examination: may reveal vascular changes in the eyes, retinal
hemorrhages, or edema of the optic nerves, known as papilledema.
Adequate medical diagnosis of HypertensionBlood pressure measurement is the initial strategy and the gold standard to
confirm the diagnosis of hypertension in most patients. In practice, blood pressure
measurement is simple and quick and should be performed at every clinical
encounter.
When hypertension is suspected or confirmed based on blood pressure readings,
a physical examination and all related investigations should be performed to
determine the extent of target-organ damage if any. Look for the presence of
cardiovascular or kidney disease, the presence or absence of other cardiovascular
risk factors, lifestyle factors that could potentially contribute to hypertension,
potential interfering substances (eg, chronic use of nonsteroidal antiinflammatory
drugs, estrogen-containing oral contraceptives) that can lead to hypertension.
The physical examination should include the funduscopic examination to evaluate
for hypertensive retinopathy and must be able to detect/predict all other possible
complications.
Treatment plan
Goals include achieving and maintaining normal blood pressure and reducing
cardiovascular risk and target organ disease. This treatment plan includes lifestyle
modifications and medications:
1. Weight reduction: overweight persons have an increased incidence of
hypertension and increased risk for cardiovascular diseases. When a person
decreases caloric intake, sodium and fat intake are usually also reduced.
Although reducing the fat content of the diet has not been shown to produce
sustained benefits in blood pressure control, it may slow the progress of
atherosclerosis and reduce overall cardiovascular diseases risk.
2. Dietary sodium and potassium reduction: this involves avoiding foods
known to be high in sodium and not adding salt in the preparation of foods
or at meals.
3. Avoid/Moderation of alcohol consumption,
4. Regular physical activity: physically active lifestyle is essential to promote
and maintain good health. Physical activity is more likely to be done if it is
safe and enjoyable, fits easily into one’s daily schedule, and is inexpensive.
People with hypertension must increase their physical activity. Advise
sedentary people to increase activity levels gradually.
5. Avoidance of tobacco use (smoking and chewing), and
6. Management of psychosocial risk factors.
7. Medications: the drugs currently available for treating hypertension have
two main actions: (1) they decrease the volume of circulating blood and (2)
they reduce systemic vascular resistance. The drugs used in the treatment of
hypertension include diuretics, the adrenergic inhibitors, direct vasodilators,angiotensin and renin inhibitors, and calcium channel blockers.
Key nursing interventions:
1. Health promotion: Primary prevention of hypertension is a cost-effective
approach. Current recommendations for primary prevention include lifestyle
modifications that prevent or delay the rise in blood pressure in at-risk people.
2. Blood Pressure Measurement: Initially, take the blood pressure in both
arms to note any differences. Proper size and correct placement of the blood
pressure cuff are critical for accurate measurement.
3. Screening Programs: screening programs in the community are widely
used to check individuals for high blood pressure. At the time of the blood
pressure measurement, give each person a written, numeric value of the
reading. If necessary, explain why further evaluation is needed. Effort and
resources should focus on the following: (1) controlling blood pressurein persons already identified as having hypertension; (2) identifying and
controlling blood pressure in at-risk groups such as obese people, and
relatives of people with hypertension; and (3) screening those with limitedaccess to the health care system.
4. Monitoring of Patient Adherence to medications and regimen: A major
problem in the long-term management of the patient with hypertension
is poor adherence with the prescribed regimen. The reasons for poor
adherence include inadequate patient teaching, unpleasant side effects of
drugs, return of blood pressure to normal range while on medication, lack
of motivation, high cost of drugs, lack of insurance, and lack of a trusting
relationship between the patient and the health care provider.
Also assess the patient’s diet, activity level, and lifestyle as additional
indicators of adherence. Individually assess patients to determine the
reasons why the patient is not adhering to the treatment and develop a
plan with the patient to improve adherence. The plan should be compatible
with the patient’s personality, habits, and lifestyle. Active patient participation
increases the likelihood of adherence to the treatment plan. Measures
such as including the patient in the development of a medication schedule,
selecting medications that are affordable, and involving caregivers help
increase patient adherence.
Substituting combination drugs for multiple drugs once the BP is stable may
also facilitate adherence. Combination drugs reduce the number of pills the
patient has to take each day and may reduce costs. It is important to help
the patient and caregiver understand that hypertension is a chronic illness
that cannot be cured. Emphasize that it can be controlled with drug therapy,
diet changes, physical activity, periodic follow-up, and other relevant lifestyle
modifications.Evolution and complications of hypertension
Hypertension is associated with a significant increase in risk of adverse cardiovascular
and kidney outcomes. Each of the complications is closely associated with thepresence of hypertension.
Complications of hypertension
Regardless of whether a person has essential or secondary hypertension, the
accompanying organ damage and complications are the same. Hypertension
causes the heart to work harder to pump against the increased resistance. The extra
work and the greater mass increase the heart’s need for oxygen. If the myocardium
doesn’t receive sufficient oxygenated blood, myocardial ischemia occurs and theclient experiences angina. Consequently, the size of the heart muscle increases.
When the heart no longer can pump adequately to meet the body’s metabolic needs,
heart failure occurs. In addition to its direct effects on the heart, high blood pressure
damages the arterial vascular system. It accelerates atherosclerosis. Furthermore,
the increased resistance of the arterioles to the flow of blood causes serious
complications in other body organs, including the eyes, brain, heart, and kidneys.
Hemorrhage of tiny arteries in the retina may cause marked visual disturbances
or blindness. A cerebrovascular accident (stroke) may result from hemorrhage or
occlusion of a blood vessel in the brain. Myocardial infarction (MI) may result from
occlusion of a branch of a coronary artery. Impaired circulation to the kidneys mayresult in renal failure.
In summary, the complications of hypertension are:
– Hypertension emergency
– Atherosclerotic coronary artery disease
–Myocardial ischemia/ infarction
– Heart failure
– Renal Failure
– Stroke/ Cerebral hemorrhage/ Cerebral ischemia
– Aortic aneurysm
– Retinal vascular sclerosis– Gangrene of extremities
Hypertensive Crisis:
Hypertensive crisis is a term used to indicate either a hypertensive urgency or
emergency. This is determined by the degree of target organ disease and how
quickly the blood pressure must be lowered.
A hypertensive emergency develops over hours to days. It is a situation in which
a patient’s blood pressure is severely elevated (often above 220/140 mm Hg) with
clinical evidence of target organ disease. It can cause encephalopathy, intracranial
or subarachnoid hemorrhage, acute left ventricular failure, myocardial infarction,
renal failure, dissecting aortic aneurysm, and retinopathy.
Hypertensive urgency develops over days to weeks. This is a situation in which a
patient’s blood pressure is severely elevated (usually above 180/110 mm Hg), but
there is no clinical evidence of target organ disease.
Prompt recognition and management of hypertensive crisis are essential to decrease
the threat to organ function and life. Hypertensive crisis occurs more often in patients
with a history of hypertension who have not adhered to their medication regimens
or who have been under-medicated. In such cases, rising blood pressure is thoughtto trigger endothelial damage and the release of vasoconstrictor substances.
Clinical Manifestations
A hypertensive crisis is often manifested as hypertensive encephalopathy, a
syndrome in which a sudden rise in blood pressure is associated with severe
headache, nausea, vomiting, seizures, confusion, and coma. Patients can have
chest and back pain, dyspnea, and possibly reduced or absent pulses in theextremities.
Management of Hypertensive crisis:
Blood pressure level alone is a poor indicator of the seriousness of the patient’s
condition. It is not the major factor in deciding the treatment for a hypertensive
crisis. The link between elevated blood pressure and signs of new or progressive
target organ disease determines the seriousness of the situation. Hypertensive
crisis require hospitalization, intravenous administration of antihypertensive drugsand intensive care monitoring.
Self-assessment 2.2
1. What is included in the correct technique for BP measurements?
a. Always take the BP in both arms.
b. Position the patient supine for all readings.
c. Place the cuff loosely around the upper arm.d. Take readings at least two times at least 1 minute apart.
2. Which BP-regulating mechanism(s) can result in the development of
hypertension if defective (select all that apply)?
a. Release of norepinephrine
b. Stimulation of the sympathetic nervous system
c. Stimulation of the parasympathetic nervous systemd. Activation of the renin-angiotensin-aldosterone system
3. While obtaining subjective assessment data from a patient with
hypertension, the nurse recognizes that a modifiable risk factor for the
development of hypertension is:
a. A low-calcium diet.
b. Excessive alcohol consumption.
c. A family history of hypertension.d. Consumption of a high-protein diet.
4. When obtaining a health history from a client, which finding is most
suggestive that the client is hypertensive? (select all that apply)
a. The client experiences occasional heart palpitations associated with chestpain.
b. The client has experienced fainting episodes.
c. The client has difficulty sleeping all night.
d. The client is having pounding headache
5. Basing on the causes and risk factors, differentiate briefly the essentialand secondary hypertension.
6. What are two physiologic components that determine blood pressure?
7. You are caring for P.N., a 46-year-old man with a history of poorly
controlled hypertension and chronic kidney disease. You note that he is
taking the antihypertensive medications. He tells you that he can no longer
live with the side effects of these drugs (e.g., fatigue, dry mouth, erectile
dysfunction). He states that he wants to stop taking the medications. He
believes that if he changes his lifestyle by reducing salt from his diet,
losing weight, and beginning exercise, he can control his hypertension.
a. Explain different lifestyle changes you would advise P.N. to practice in
order to be able to control her hypertension.
b. P.N. must continue to take her medications. Justify the importance ofadherence to hypertensive medications.
8. List all essential needed investigations and their rationale in themanagement of hypertension.
9. What are the elements that constitute the nursing management of theclient with hypertension?
10. List all potential complications of uncontrolled hypertension.
11. Which manifestation is an indication that a patient is having a hypertensiveemergency?
a. Symptoms of a stroke with an elevated BP
b. A systolic BP >220 mm Hg and a diastolic BP >140 mm Hg
c. A sudden rise in BP accompanied by neurologic impairment
d. A severe elevation of BP that occurs over several days or weeks
12. Discuss the medical and nursing management of the client withHypertensive crisis.
Case study:
Carefully read the case scenario below and answer the followingquestions:
K.J. is a 73-year-old woman with no history of hypertension. She came to the
clinic for dizziness and chronic headache. She says she has gained 10Kgs over
the past year. Her father died from stroke. She has never smoked and uses no
alcohol. She takes one medication (multivitamin). She eats a lot of carbohydrates
food and does not do exercise because she feels tiredness whenever she wants
to do exercises. Her vital parameters are: height: 168 cm, weight: 86 kgs, BP:
190/82 mm Hg Pulse: 82 beats per minute, Temperature: 36.2 degree Celsius,
Respiratory rate: 18 cycles per minute. During her physical examination there
are no abnormalities at other systems except BMI and blood pressure that are
high. She was primarily diagnosed to have primary hypertension while waiting
for additional investigations.
1. What are the contributing factors to the development of hypertension was
K.J. presenting?
2. What additional information would you need to collect that will help in
deciding about the medical condition of K.J?
3. From her condition, what would you advise as investigations to be
requested that might be helpful in deciding further management of K.J
medical condition? Justify the rationale.
4. Discuss all aspects that might be included into her medical and nursing
management.
5. If drug therapy became necessary to treat K.J.’s hypertension, give three
examples of antihypertensive drugs that would be indicated based on herclinical status?
6. Explain the different lifestyles changes would you recommend to K.J.?7. If her condition is not well managed, what do you expect as complications?
2.3 STROKE
Learning Activity 2.3
Observe the image below and read carefully the scenario below andanswer the questions that follow:

Figure2.5 Patient with left side body functional impairment.
N.J. is a 66-years-old woman who lives in Kigali. She arrives in the emergency
department at CHUK after falling down during the night when she tried to get
up to go to the bathroom. She had history of high blood pressure. She states
that she fell because she could not control her left leg. Her husband brought
her to the hospital, but states that it was not possible for him to get his wife to
the car alone because most of her body parts were not functioning and were
weak. When arrived at CHUK, she was having paralysis of entire left side of the
body involving left arm and left leg, inability to sit and stand alone, general body
weakness, and unable to speak.
1. Referring to the above situation, what might be the possible cause for her
left side body functional impairment and general body weaknesses?
2. What are other additional information you would ask to guide in diagnosing
the medical condition that patient has?
3. In general, what are the causes and risk factors do you think can be at the
origin of that medical problem?
4. What investigations might you expect to be ordered in order to confirm
the medical diagnosis?
5. What will be included into the comprehensive physical assessment of
N.J?
6. What is the medical diagnosis is N.J presenting?
7. What should be included into the treatment plan for N.J?
8. Identify all possible complications that might result from the medicalcondition of N.J.?
the brain, with stroke being the most frequent manifestation of cerebrovascular
disease.
Brain and cerebral nerve cells are extremely sensitive to a lack of oxygen; if they
are deprived of oxygenated blood for 3 to 7 minutes, both the brain and nerve cells
begin to die. Prolonged interruption in the flow of blood and oxygen through one of
the arteries supplying the brain leads to stroke or cerebrovascular accident.
A stroke also called cerebrovascular accident occurs when the blood supply to parts
of the brain is interrupted or reduced, preventing brain tissue from getting oxygen
and nutrients. A stroke is a medical emergency, and prompt treatment is crucial.
Early recognition and action can reduce brain damage and further complications.
Causes, risks factors and pathophysiology
Genetic risk factors (among non-modifiable risk factors) are important in the
development of all vascular diseases, including stroke. A person with a family
history of stroke has an increased risk of having a stroke. Genes encoding products
involved in lipid metabolism, thrombosis, and inflammation are believed to be
potential genetic factors for stroke. Modifiable risk factors are those that can be
altered through lifestyle changing and medical treatment, thus reducing the risk ofstroke.
Cerebrovascular disease arises from pathological processes in blood vessels of
Modifiable risk factors for hypertension are: metabolic syndrome, heart disease,
heavy alcohol consumption, poor diet, drug abuse, sleep apnea, obesity, physicalinactivity and smoking.
Non modifiable risk factors for hypertension are: age, gender, race, heredity/family history.
Strokes are classified on the basis of underlying pathophysiologic findings: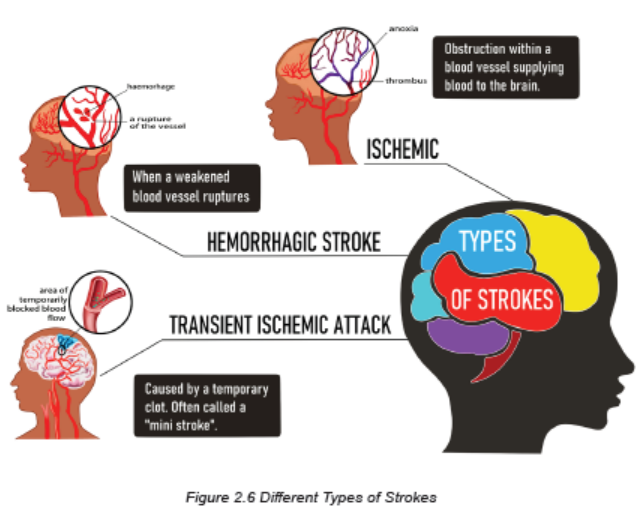
A. Ischemic (represent 80% of all Strokes): mainly due to thrombus, emboli,
systemic hypo perfusion, and atherosclerosis. When ischemic strokes occur,
glucose and oxygen to brain cells are reduced. The reduced glucose quickly
depletes the stores of adenosine triphosphate (ATP), resulting in anaerobic
cellular metabolism and the accumulation of toxic products such as lactic
acid. Although some brain cells die from anoxia, the lack of oxygen destroysadditional brain cells by a secondary mechanism
1. Atherosclerotic: Fatty streak is covered by collagen, forming a fibrous
plaque that appears grayish or whitish, that result in narrowing of vessel
lumen, and continued inflammation can result in plaque instability, ulceration,
and rupture, platelets accumulate and thrombus forms, Increased narrowingor total occlusion of lumen.
2. Systemic hypoperfusion: Reduced blood flow is more global in patients
with systemic hypoperfusion and does not affect isolated regions. The
reduced perfusion can be due to cardiac pump failure caused by cardiac
arrest or arrhythmia, or to reduced cardiac output related to acute myocardial
ischemia, pulmonary embolism, pericardial effusion, or bleeding. Hypoxemia
may further reduce the amount of oxygen carried to the brain.
3. Thrombotic stroke: Thrombosis occurs in relation to injury to a blood
vessel wall and formation of a blood clot that result to narrowing of the blood
vessel. It is the most common cause of stroke. The thrombotic strokes are
associated with hypertension or diabetes mellitus, both of which accelerate
atherosclerosis.
4. Embolic stroke: Occurs when an embolus lodges in and occludes a
cerebral artery. It is the second most common cause of stroke. Most emboli
originate in the endocardial (inside) layer of the heart, with plaque breaking
off from the endocardium and entering the circulation. The embolus travels
upward to the cerebral circulation and lodges where a vessel narrows.
Patient with an embolic stroke commonly has a rapid occurrence of severe
clinical symptoms but warning signs are less common with embolic than with
thrombotic stroke. Onset of embolic stroke is usually sudden and may or
may not be related to activity. Patient usually remains conscious, althoughmay have a headache.
B. Hemorrhagic (represent 20% of all Strokes): due to intracerebral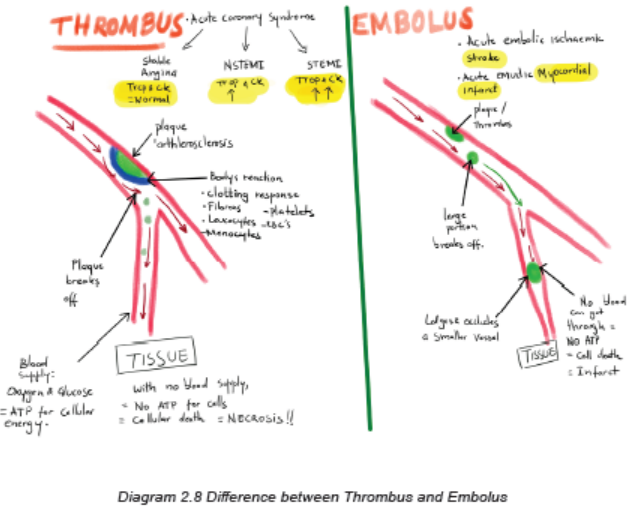
hemorrhage (ICH) or subarachnoid hemorrhage (SAH). Hypertension is
the most important cause. This type of stroke results from bleeding into the
brain tissue itself or into the subarachnoid space or ventricles. Hemorrhage
commonly occurs during periods of activity. It often has a sudden onset of
sympt oms, with progression over minutes to hours because of ongoing
bleeding.
C. Transient ischemic attack (TIA): It is a transient episode of neurologic
dysfunction caused by focal brain, spinal cord, or retinal ischemia, without
acute infarction of the brain. The symptoms last less than one hour and most
TIAs resolve. We need to encourage patients to consult a health facility at any
symptom onset/occurrence since once a TIA starts, one does not know if it
will persist and become a true stroke, or if it will resolve.
Clinical Manifestations
Primary assessment focuses on cardiac and respiratory status (ABC: Airway,
Breathing, Circulation) and neurologic assessment. If the patient is stable, the
history is obtained as follows: (1) description of the current illness with attention to
initial symptoms, particularly symptom onset and duration, nature (intermittent or
continuous), and changes; (2) history of similar symptoms previously experienced;
(3) current medications; (4) history of risk factors and other illnesses such as
hypertension; and (5) family history of stroke or cardiovascular diseases. This
information is gained through an interview of the patient, family members, significant
others, and/or caregiver.
Secondary assessment includes a comprehensive neurologic examination of
the patient. This includes (1) level of consciousness (using the Glasgow Coma
Scale), (2) cognition; (3) motor abilities; (4) cranial nerve function; (5) sensation; (6)
proprioception; (7) cerebellar function; and (8) deep tendon reflexes.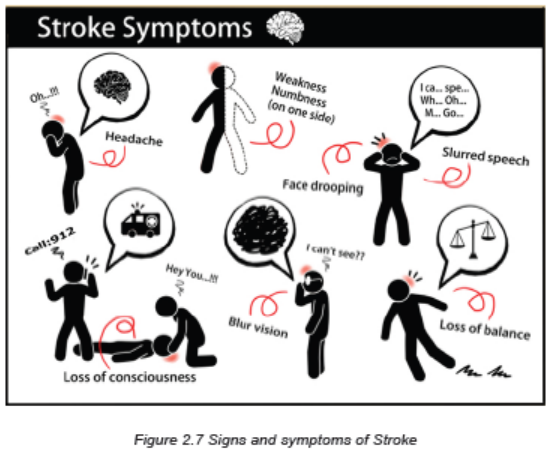
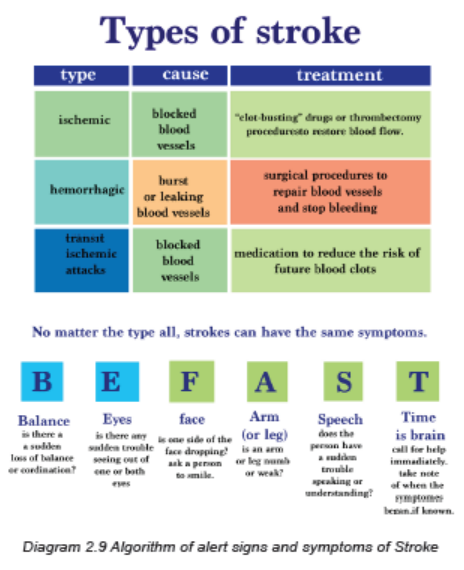
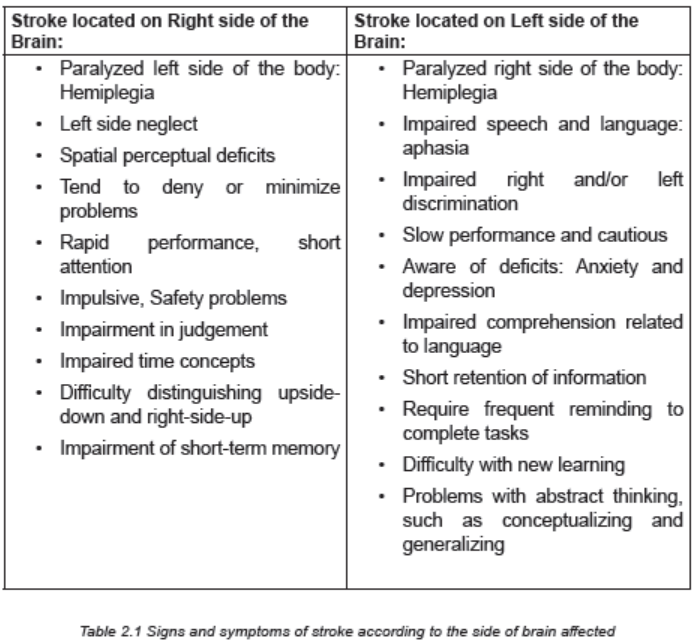
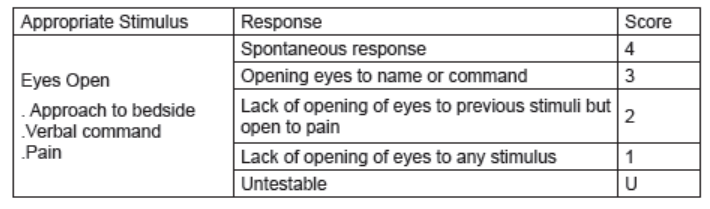
Motor deficits are the most obvious effect of stroke. Motor deficits include impairment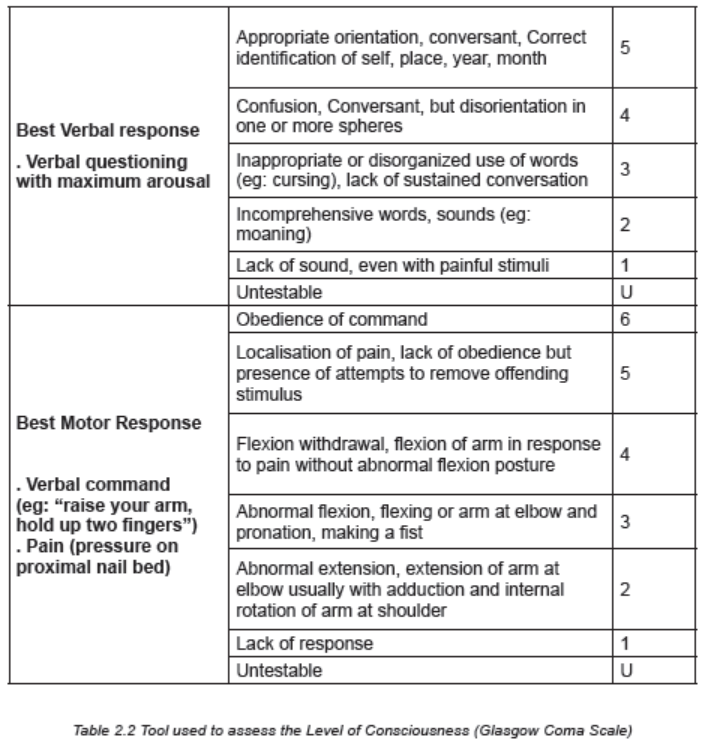
of (1) mobility, (2) respiratory function, (3) swallowing and speech, (4) gag reflex,and (5) self-care abilities.
Investigations
When manifestations of a stroke occur, diagnostic studies are done to:
• Confirm that it is a stroke and not another brain lesion and
• Identify the likely cause of the stroke.
Important diagnostic tools for patients who have experienced a stroke are a non
and/or contrasted computed tomography scan (CT Scan) or magnetic resonanceimaging (MRI). These tests can rapidly distinguish between ischemic and
hemorrhagic stroke and help determine the size and location of the stroke.
The following Blood tests are also done to help identify conditions contributing to
stroke and to guide in deciding the management: Complete blood count (including
platelets, coagulation studies: prothrombin time, troponin, international normalization
rate: INR), Electrolytes (sodium, potassium, calcium, chloride, etc), Blood glucose
levels, Renal function tests (urea and creatinine), and Liver function tests (ASAT,
ALAT), Lipid profile, Cerebrospinal fluid analysis. The Electrocardiogram can alsobe performed.
Adequate Medical Diagnosis
Stroke is diagnosed through several technics: history taking, and comprehensive
physical exam that include the neurological examination. Imaging investigations like
CT scan and MRI are helpful. These imaging are helpful in determining the extent
of injury and location, therefore determining the causes and subtypes. Laboratory
investigations are needed to look for other factors that might be associated withstroke.
Treatment Plan
Hypertension is the single most important modifiable risk factor, therefore it needsto be detected early and adequately treated. The goals for collaborative and
comprehensive management of stroke are:
1. To prevent secondary brain injury (intracranial hypertension, hematoma
expansion, elevated intracranial pressure, seizures, herniation )
2. To maintain and secure the airways (due to paralysis of the pharynx
muscles),
3. To provide general body support (vital signs, fluid and electrolyte balance,
hemodynamic patient monitoring: all Systems to be cared for) and
4. To anticipate the occurrence of complications (atelectasis, aspiration
pneumonia, airway obstruction that might require tracheal intubation and
mechanical ventilation), and plan for Respiratory system management asPriority.
Interventions
While caring for patient with stroke, the care providers must ensure the following:
A. Cardiac and Respiratory System:
• Ensure patent airway, Call for resuscitation team/shout for help, Perform
pulse oximetry (SP02) and oxygen therapy as urgency to maintain adequate
oxygenation.
• Obtain IV access.
• Monitor and maintain normal BP and other vital signs, and watch for
hypertension post stroke (Continuous effective monitoring of BP). Eligible to
thrombolysis: BP≤ 185/110 mmHg before and 180/105 mmHg after for at
least 24 hours. Blood pressure should not be treated acutely for patients with
ischemic stroke who are not eligible to thrombolysis, except Hypertension
is extreme, BP >220/120 mmHg. Intravenous agents are recommended for
blood pressure lowering, labetalol& nicardipine as first line , IV Nitroprusside
as second-line therapy.
• Obtain CT scan or MRI immediately, Perform baseline laboratory tests (FBC,
Troponin, INR(International Normalization Rate), etc).
• Proper Positioning of patient head: The appropriate position of the patient
and the head of bed should be respected to prevent the risk of elevated
intracranial pressure and aspiration. The head in neutral alignment with the
body elevation of the head of the bed to 30 degrees are recommended if no
symptoms of shock or injury occur.
• Implement anti-seizure precautions and Anticipate thrombolytic therapy for
ischemic stroke.
• Adjusting fluid intake to the individual needs of the patient, Regulating IV
infusions and calculating intake and output, noting imbalance. Fluid andelectrolyte balance must be controlled carefully: Adequate hydration promotes
perfusion and decreases further brain injury. Adequate fluid intake during
acute care via oral, intravenous (IV), or tube feedings should be 1500 to 2000
mL/day. Over hydration may compromise perfusion by increasing cerebral
edema.
• Monitoring lung sounds for crackles and rhonchi (pulmonary congestion) and
monitoring heart sounds for murmurs.
• Monitoring and Management of blood glucose levels: Hypoglycemia can
cause focal neurologic deficits mimicking stroke, therefore check the blood
sugar and rapidly correct low serum glucose (<60 mg/dL /3.3 mmol/L).
Hyperglycemia in diabetic patients or stress hyperglycemia is associated with
poor functional outcome. Hyperglycemia may augment brain injury by several
mechanisms including increased tissue acidosis from anaerobic metabolism,
free radical generation, and increased blood brain barrier permeability.
• Check for fever and other signs and symptoms of infection: Meningitis,
subdural empyema, brain abscess, and infective endocarditis need to be
excluded as the etiology of fever if acute neurologic deterioration
• After stroke, patient is at risk for deep vein thrombosis related to immobility,
loss of venous tone, and decreased muscle pumping in leg, most effective
prevention is keeping the patient moving, and encourage ambulation.
B. Musculoskeletal and Integumentary system: Goal is to maintain optimal
function:
• Prevention of joint contractures and muscular atrophy: Range-of-motion
exercises and positioning are important. Paralyzed or weak side needs
special attention when positioning.
• Avoidance of pulling the patient by the arm to avoid shoulder displacement
• Good skin hygiene, Early mobility, ambulation and Change position of the
patient because the stroke patient is susceptible to skin breakdown related to
Loss of sensation, Decreased circulation, Immobility compounded by patient
age, poor nutrition, dehydration, oedema, and incontinence
C. Gastrointestinal system:
• Patients may be placed on stool softeners.
• Physical activity promotes bowel function.
• Implement a bowel management program for problems with bowel control,
constipation, incontinence
D. Urinary system:
• Promote normal bladder function.
• Avoid the use of indwelling catheters as much as you can.
E. Nutrition:
• Nutritional needs require quick assessment and treatment.
• May initially receive IV infusions to maintain fluid and electrolyte balance
• May require nutritional support
• First feeding should be approached carefully, and always test swallowing,
chewing, gag reflex, before beginning oral feeding.
• Feedings must be followed by oral hygiene.
• High-fiber diet and adequate fluid intake
F. Antiplatelet drugs are usually the chosen treatment: Aspirin is the most
frequently used as antiplatelet agent. Recombinant Tissue plasminogen
activator: to reestablish blood flow from blocked blood vessel. To be given
3 to 4.5 hours after signs and symptoms of ischemic stroke. Determining
eligibility to IV thrombolytic therapy for patients with acute ischemic stroke: IV
Alteplase is first-line therapy, to be initiated within 4.5 hours of symptom onset
or the time last known to be well. Oral anticoagulation using warfarin is the
treatment of choice for individuals with atrial fibrillation.
G. Surgical interventions might be needed depending on medical diagnosis
and goal of treatment (eg: hematoma evacuation, removing the plaque,opening the blocked artery, anastomosis, etc).
Preventive Strategies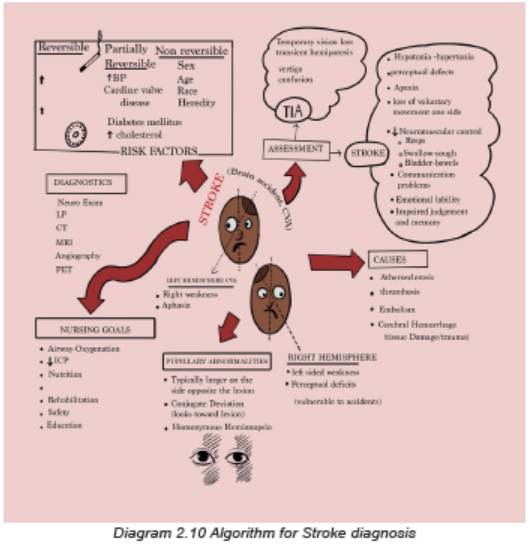
1. Teaching patients and families about all Preventive measures (reduce salt
and sodium intake, Maintain a normal body weight, Maintain a normal blood
pressure, Increase level of physical exercise, Avoid cigarette smoking or
tobacco products, Limit consumption of alcohol to moderate levels, Follow a
diet that is low in saturated fat, total fat, and dietary cholesterol and high in
fruits and vegetables).
2. Teaching patients and families about signs and symptoms, stroke
pathophysiology, complications and when to seek health care for symptoms.
3. Education about hypertension control and adherence to medication,
particularly in persons with known risk factors.
4. Education and management of modifiable risk factors to change lifestyle:
Patients with known risk factors (Diabetes mellitus, Hypertension, Obesity,
High serum lipids, Cardiac dysfunction, etc) require close and effective
management.
Evolution and Complications
Stroke is a significant cause of death and disability. The highest incidence of stroke
occurs among older adults and the people with comorbidities. Stroke can result
in a profound disruption in the life of a person. The ability to perform activities of
daily living may require many adaptive changes because of physical, emotional,
perceptual, and cognitive deficits. There is need to assist the patient and caregiver
in the transition through acute phase of care, rehabilitation, long-term care, and
home care. The needs of the patient, the caregiver, and the family involvement
require ongoing health education.
The most common complications of stroke are:
• Brain edema: swelling of brain post stroke
• Pneumonia: causes breathing problems
• Swallowing problems: that can potentially cause the aspiration pneumonia
• Blood clot or deep vein thrombosis: related to limited range of motion/physical
activity
• Aphasia and speech disorders• Depression and other mood disorders, chronic headache,etc
Self-assessment 2.3
1. Indicate whether the following manifestations of a stroke are more likely
to occur with right brain damage (R) or left brain damage (L).
a. Aphasia
b. Impaired judgment
c. Quick, impulsive behavior
d. Inability to remember words
e. Neglect of the left side of the body
f. Hemiplegia of the right side of the body
2. Four days following a stroke, a patient is to start oral fluids and feedings.
Before feeding the patient, what should the nurse do first?
a. Check the patient’s gag reflex.
b. Order a soft diet for the patient.
c. Raise the head of the bed to a sitting position.
d. Evaluate the patient’s ability to swallow small amounts of crushed ice or
ice water.
3. What is the priority intervention in the emergency department for the
patient with a stroke?
a. Intravenous fluid replacement
b. Administration of osmotic diuretics to reduce cerebral edema
c. Initiation of hypothermia to decrease the oxygen needs of the brain
d. Maintenance of respiratory function with a patent airway and oxygen
administration
4. What is the difference between ischemic and hemorrhagic stroke?
5. Describe different criteria that are assessed to determine the level of
consciousness using Glasgow coma scale
6. List the preventive strategies of stroke for (1) healthy people and
overweight people, and (2) patient with hypertension and diabetes.
7. What therapeutic options are available for the patient with a hemorrhagicand ischemic stroke?
Case studyCarefully read the case study below and answer the following questions:
R.C., a 52-year-old married man, was admitted to the hospital with unconscious
after his family find that he could not wake up in the morning. He was accompanied
by his wife and one daughter 20 years. He had history of hypertension with poor
adherence on captopril and had overweight. He complained of severe headache
associated with epistaxis the day before he became unconsciousness. Vital
signs at arrival at hospital: BP 198/102 mmHg, RR 16 cycles/minute, HR 74
bpm, Temp 36.7°C, SPo2: 82% on room air. His Glasgow Coma Scale score:
9/15. He is not able to open the mouth, unable to sit or stand without support,and has right sided hemiplegia. Blood sugar: 94 mg/dl.
Questions:
1. What will be additional information you will ask the family members toguide in deciding about the diagnosis and the management?
2. What investigations will you advise to be requested to determine the
cause of R.C. unconsciousness? What is the rationale of requestingthose investigations?
3. List all nursing interventions that have the highest priority for R.C. at thisstage of his illness?
4. What should the family be told to expect in terms of R.C. medicalcondition
2.4 END UNIT 2 ASSESSMENT
End of unit 2 assessment
SECTION A: Short Answer Questions
1. Cardiac output is the product of ……………………….. multiplied
by…………………………..
2. Prolonged hypertension can cause significant damage to these four
“target organs”: A)………………… B)…………………………….,
C)…………………………, and D)………………..
3. Discuss in detail several hypotheses about the pathophysiologic basis for
elevated blood pressure.
4. Explain how lifestyle changes and medications can control, not cure,
hypertension.
5. Compare and contrast the different medications used to treat hypertension
and the associated nursing considerations.
6. Compare and contrast a hypertensive crisis with a hypertensive
emergency.
7. List four non modifiable risk factors for stroke.
8. Compare the etiology and symptoms of two types of stroke: ischemic
stroke and hemorrhagic stroke.
9. Describe the focus of nursing interventions when helping a patient recoverfrom an ischemic stroke.
10. Identify the significance of the following laboratory test results when foundin patients with hypertension:
11. A 42-year-old man has been diagnosed with primary hypertension with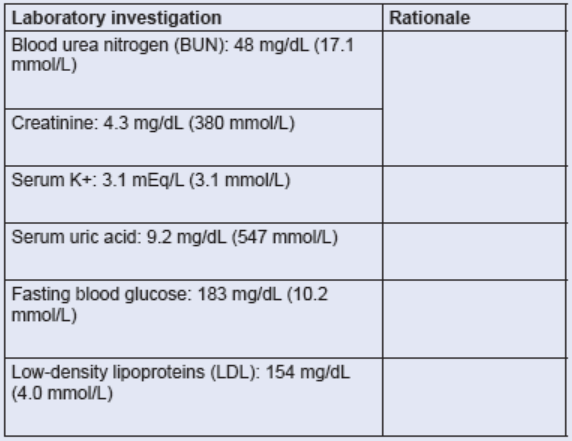
an average blood pressure of 162/92 mm Hg on three consecutive clinic
visits. What are four priority lifestyle modifications that should be exploredin the initial treatment of the patient?
12. Identify two medical therapies that are specific to each of the followingtypes of shock.
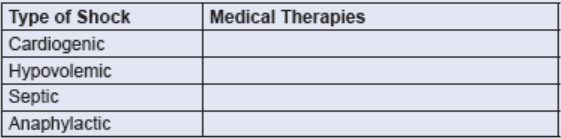
SECTION B: Multiple Choice Questions
1. After taking vital signs, you write down your findings as temperature of
36.6 degree Celsius, Pulse of 66 beats per minute, respiratory rate of 18
cycles per minutes, Blood Pressure of 124/82 mmHg. Which of thesenumbers represents the systolic blood pressure?
a. 36.6
b. 124
c. 82
d. 66
2. Stroke volume of the heart is determined by:
a. The degree of cardiac muscle strength (pre-contraction).
b. The intrinsic contractility of the cardiac muscle.
c. The pressure gradient against which the muscle ejects blood duringcontraction.
d. All of the above factors.
3. The most important factor in regulating the caliber of blood vessels, whichdetermines resistance to flow, is:
a. Hormonal secretion.
b. Independent arterial wall activity.
c. The influence of circulating chemicals.
d. The sympathetic nervous system.
4. Stage 1 hypertension is defined as persistent blood pressure levels in
which the systolic pressure is higher than …………. and the diastolic ishigher than …………….
a. 110/60 mm Hg
b. 120/70 mm Hg
c. 130/80 mm Hgd. 140/90 mm Hg
5. Georgia, a 30-year-old woman, is diagnosed as having secondary
hypertension when serial blood pressure recordings show her average
reading to be 170/100 mm Hg. Her hypertension is the result of renal
dysfunction. The kidneys help maintain the hypertensive state in essential
hypertension by:
a. Increasing their elimination of sodium in response to aldosterone secretion.
b. Releasing renin in response to decreased renal perfusion.
c. Secreting acetylcholine, which stimulates the sympathetic nervous system
to constrict major vessels.
d. Doing all of the above.
6. The first priority of treatment for a patient with altered level of consciousness
is:
a. Assessment of pupillary light reflexes.
b. Determination of the cause.
c. Positioning to prevent complications.
d. Maintenance of a patent airway.
7. The degree of neurologic damage that occurs with an ischemic stroke
depends on the:
a. Location of the lesion.
b. Size of the area of inadequate perfusion.
c. Amount of collateral blood flow.
d. Combination of the above factors.
8. The initial diagnostic test for a stroke, usually performed as emergency is:
a. 12-lead electrocardiogram.
b. Carotid ultrasound study.
c. Non contrasted computed tomogram.
d. Transcranial doppler flow study.
9. How is secondary hypertension differentiated from primary hypertension?
a. Has a more gradual onset than primary hypertension
b. Does not cause the target organ damage that occurs with primaryhypertension
c. Has a specific cause, such as renal disease, that often can be treated by
medicine or surgery
d. Is caused by age-related changes in BP regulatory mechanisms in people
over 65 years of age
10. What is most organ damage in hypertension related to?
a. Increased fluid pressure exerted against organ tissue
b. Atherosclerotic changes in vessels that supply the organs
c. Erosion and thinning of blood vessels from constant pressure
d. Increased hydrostatic pressure causing leakage of plasma into organ
interstitial spaces
11. A 38-year-old man is treated for hypertension with triamterene and
hydrochlorothiazide and metoprolol. Four months after his last clinic
visit, his blood pressure returns to pretreatment levels and he admits he
has not been taking his medication regularly. What is the nurse’s best
response to this patient?
a. “Try always to take your medication when you carry out another daily
routine so you do not forget to take it.”
b. “You probably would not need to take medications for hypertension if you
would exercise more and stop smoking.”
c. “The drugs you are taking cause sexual dysfunction in many patients. Are
you experiencing any problems in this area?
d. “You need to remember that hypertension can be only controlled with
medication, not cured, and you must always take your medication.”
12. What does the nursing responsibility in the management of the patient
with hypertensive urgency often include?
a. Monitoring hourly urine output for drug effectiveness
b. Titrating IV drug dosages based on BP measurements every 2 to 3 minutes
c. Providing continuous electrocardiographic (ECG) monitoring to detect side
effects of the drugs
d. Instructing the patient to follow up with a health care professional within 24hours after outpatient treatment
13. What is included in the correct technique for blood pressure
measurements?
a. Always take the BP in both arms.
b. Position the patient supine for all readings.
c. Place the cuff loosely around the upper arm.
d. Take readings at least two times at least 1 minute apart.
14. A patient comes to the emergency department immediately after
experiencing numbness of the face and an inability to speak but while
the patient awaits examination, the symptoms disappear and the patient
requests discharge. Why should the nurse emphasize that it is important
for the patient to be treated before leaving?
a. The patient has probably experienced an asymptomatic lacunar stroke.
b. The symptoms are likely to return and progress to worsening neurologic
deficit in the next 24 hours.
c. Neurologic deficits that are transient occur most often as a result of small
hemorrhages that clot off.
d. The patient has probably experienced a transient ischemic attack (TIA),
which is a sign of progressive cerebrovascular disease.
15. What are characteristics of a stroke caused by an intracerebral hemorrhage
(select all that apply)?
a. Carries a poor prognosis caused by rupture of a vessel
b. Strong association with hypertension
c. Commonly occurs during or after sleep
d. Creates a mass that compresses the brain
16. A patient is admitted to the hospital with a left hemiplegia. To determine
the size and location and to ascertain whether a stroke is ischemic or
hemorrhagic, the nurse anticipates that the health care provider will
request (select all that apply):
a. Lumbar puncture.
b. Cerebral arteriogram.
c. Magnetic resonance imaging (MRI).d. Computed tomography (CT) scan with or without contrast.
17. Which intervention should the registered nurse delegate to the associate
nurse when caring for a patient following an acute stroke?
a. Assess the patient’s neurologic status.
b. Assess the patient’s gag reflex before beginning feeding.
c. Administer ordered antihypertensives and platelet inhibitors.
d. Teach the patient’s caregivers strategies to minimize unilateral neglect.
18. What is the key factor in describing any type of shock?
a. Hypoxemia
b. Hypotension
c. Vascular collapse
d. Inadequate tissue perfusion
19. Which hemodynamic monitoring description of the identified shock is
accurate?
a. Tachycardia with hypertension is characteristic of neurogenic shock.
b. In cardiogenic shock the patient will have an increased pulmonary artery
wedge pressure (PAWP) and a decreased cardiac output (CO).
c. Anaphylactic shock is characterized by increased systemic vascular
resistance (SVR), decreased CO, and decreased PAWP.
d. In septic shock, bacterial endotoxins cause vascular changes that result in
increased SVR and decreased CO.
20. As the body continues to try to compensate for hypovolemic shock, there
is increased angiotensin II from the activation of the renin-angiotensinaldosterone
system. What physiologic change occurs related to the
increased angiotensin II?
a. Vasodilation
b. Decreased blood pressure (BP) and CO
c. Aldosterone release results in sodium and water excretiond. Antidiuretic hormone (ADH) release increases water reabsorption
21. Progressive tissue hypoxia leading to anaerobic metabolism and
metabolic acidosis is characteristic of the progressive stage of shock.What changes in the heart contribute to this increasing tissue hypoxia?
a. Arterial constriction causes decreased perfusion.
b. Vasoconstriction decreases blood flow to pulmonary capillaries.
c. Increased capillary permeability and profound vasoconstriction lead to the
increased hydrostatic pressure.
d. Decreased perfusion occurs, leading to dysrhythmias, decreased CO, anddecreased oxygen delivery to cells.
UNIT 3 MEDICAL PATHOLOGIES OF DIGESTIVE SYSTEM
Key Unit Competences
To take an appropriate decision on management of common pathologies of digestivesystem.
Introductory activity 3.0
Carefully observe the picture below and answer the following questions:
Figure3.1 Patient with abdominal pain
1. What could be the patient complains?
2. Which body system is affected?3. What could be the possible medical conditions of that patient?
3.1 GASTRITIS
Learning Activity 3.1
Carefully read this below situation and answer the following questions:
A nurse is on day duty and receives Mr. N. J, a 54-year-old man who was
brought to RUBONA Health Center with complaints of epigastric pain (upper
abdominal pain), anorexia, and nausea. The history taking revealed that he is
alcohol dependent and cigarette smoker for 18 years ago. The body temperature
was 36.5 degree Celsius, blood pressure 110/70 mmHg, pulse rate was 74beats
per minute, respiratory rate was 19 breaths per minutes. Mr. N.J was treated with
anti-acid drug named Aluminum Hydroxide 500mg tablet three times a day for
5 days. After 1 day the patient returned with vomiting, general body weakness
and intravenous fluid (Ringer lactate 1litter in 4 hours) was given to him before
being transferred to the district hospital where through physical examination,
the physician noted pallor conjunctiva, complete blood count (CBC) was
performed and revealed white blood cells (WBC) of 105000, Hemoglobin level
of 9 mg/dl, Helicobacter Pylori test was positive. Prescribed medicine included
clarithromycin, omeprazole and flagyl, Vitamin B12 as well as blood transfusion.
Three days after the symptoms disappeared and the patient was encouraged by
the Registered Nurse to quit smoking and alcohol intake to maintain the healthy
state before being discharged to continue the oral treatment at home.
What are abnormal signs and symptoms that patient was presenting?
1. Basing on those signs and symptoms, what could be the medical problem
of this patient?
2. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
3. What was included in the management of this case?4. If not treated, what will be the consequences?
The human stomach has a protective lining of mucus called the mucosa. This lining
protects the stomach from the strong stomach acid that digests food. When something
damages or weakens this protective lining, the mucosa becomes inflamed, causing
gastritis. Gastritis is an inflammation of the stomach lining (gastric mucosa). It can
be classified as acute gastritis (erosive) or chronic gastritis (non-erosive). Erosive
(reactive): Erosive gastritis causes both inflammation and erosion (wearing
away) of the stomach lining. This condition is also known as reactive gastritis.
Causes include alcohol, smoking, nonsteroidal anti-inflammatory drugs (NSAIDs),
corticosteroids, viral or bacterial infections and stress from illnesses or injuries.
Non-erosive: Inflammation of the stomach lining without erosion or compromisingthe stomach lining.
Causes and risk factors of gastritis
Gastritis occurs when something damages or weakens the stomach lining (mucosa).
Different things can trigger the problem including dietary indiscretions; Bile reflux
(reflux of duodenal contents): the liver makes bile to help you digest fatty foods.
“Reflux” means flowing back. Bile reflux occurs when bile flows back into the
stomach instead of moving through the small intestine; Medications: Steady use of
nonsteroidal anti-inflammatory drugs (NSAIDs) such as Aspirin or corticosteroids
to manage chronic pain can irritate the stomach lining, alcohol or caffeine: Chronic
alcohol use can irritate the stomach lining; autoimmune disease: In some people,
the body’s immune system attacks healthy cells in the stomach lining;cigarette
smoking; ingestion of poisons or corrosive substances; food allergies; infection;
and gastric ischemia secondary to vasoconstriction caused by a stress response.
The bacterial infection: Helicobacter pylori may contribute to chronic gastritis,
the bacteria break down the stomach’s protective lining and causes inflammation.
Physical stress: A sudden, severe illness or injury can bring on gastritis. Gastritis
often develops even after a trauma that doesn’t involve the stomach. Severe burns
and brain injuries are the two common causes of gastritis. The risk of developing
gastritis goes up with age. Older adults have thinner stomach linings, decreased
circulation and a slower metabolism of mucosal repair, they are also more likely to
be on drugs that can cause gastritis such as nonsteroidal anti-inflammatory drugs
and other bacteria (staphylococci, streptococci, Escherichia coli), Herpes simplex
virus, cytomegalovirus (in acquired immunodeficiency syndrome; AIDS). In addition
the stress can induce acute gastritis especially for the critically ill patients. There
are other risk factors such as alcohol, caffeine, food containing acids (vinegar and
pepper).Pathophysiology overview
Gastric secretions are highly acidic. Parietal cells in the stomach increase acid
production (hydrochloric acid) in response to seeing, smelling, and eating food. The
release of histamine and acetylcholine by parasympathetic vagus nerve stimulates
the parietal cells. An increasing level of acid triggers the conversion of pepsinogen
to pepsin, creating a chemical mixture strong enough to digest the stomach wall.
However, because mucus protectively coats the stomach lining, pepsin normally
has little effect on the stomach wall. Prostaglandin E, a lipid compound secreted
in the stomach, apparently promotes the production of mucus, which contains
buffering substances and mechanically blocks penetration by stomach acids. Thesubmucosal layers of the stomach can become inflamed, however, when irritating
substances reduce or penetrate the mucous layer. Consequently, the client
experiences epigastric discomfort, often described as heartburn.
Signs and symptoms
Usually, the client complains of epigastric pain, feeling extra full during or after a
meal (fullness), pressure, anorexia (loss of appetite), nausea, and vomiting.
When the cause of gastritis is bacterial or viral, the patient may experience vomiting,
diarrhoea, fever, and abdominal pain. When the causes of gastritis are drugs,
poisons, toxic substances and corrosives, the patient may experience gastric
bleeding. Clients may describe seeing blood in emesis or note a darkening oftheir stool colour (black stool).
The chronic gastritis may be asymptomatic or presenting symptoms similar to mild
indigestion. As many people with gastritis don’t have symptoms, people who do
have symptoms often mistake them for indigestion. Other signs of gastritis include
bloating, loss of weight without meaning to, abdominal discomfort, hematemesis(vomiting blood).
Investigations
A complete blood count (CBC) may reveal anaemia from chronic blood loss.
Stool testing for occult blood often detects the presence of RBCs (Red blood cells)
in the stool. In difficult cases, gastroscopy or colonoscopy may be performed to
visualize the mucosa and obtain specimens, which are examined for pathogens or
cellular abnormalities. Helicobacter pylori test may also be performed to rule outHelicobacter pylori bacterial infection.
Medical diagnosis of gastritis
The health care personnel need to ask the client about the symptoms, conduct
a complete history taking and perform a physical exam, some tests may be also
performed to confirm the diagnosis including blood test which is designed to check
for antibodies titers that fight against H. pylori bacteria, stool test may also be
performed to rule out H. pylori in the patient’s stool. The physician may perform the
Upper endoscopy using an endoscope (a long thin tube with an attached camera)
to see in the patient’s stomach by inserting the scope through the oesophagus to
allow the physician to examine the stomach lining where the biopsy may be taken
from the patient stomach lining to test for infection. The X-ray images may be
taken after barium swallowing during upper gastrointestinal exam.
Treatment plan of gastritis
The treatment of gastritis depends upon its causes; poisons require emergency
treatment. In acute cases, eating is restricted and IV fluids such as Ringer lactate
or normal saline are given to correct dehydration and electrolyte imbalances,
particularly if vomiting is severe. Antiemetics are prescribed to control nausea and
vomiting, and antibiotics such as amoxicillin (Amoxil) and clarithromycin (Biaxin),
which exert bactericidal effects to eradicate H. pylori. Amebicides: Metronidazole
(Flagyl) assists in the eradication of H. pylori may be prescribed to inhibit or destroyinfection.
The usual treatment of chronic gastritis is the avoidance of irritating substances,
such as alcohol and NSAIDs. Some clients may wish to avoid spicy foods, high-fatfoods, and
caffeine, depending on the degree to which these items aggravate their symptoms.
Various drugs, such as antacids, H2- receptor antagonists such as Cimetidine,
and proton pump inhibitors such as Omeprazole may be prescribed to reducethe amount of stomach acid production.
Proton pump inhibitors also treat stomach ulcers and gastroesophageal reflex
disease (GERD). Antacids: example includes Aluminium Hydroxide Al (OH)3,
Magnesium Hydroxide (Mg(OH)3, these drugs initially are used to neutralize
existing stomach acid and provide quick pain relief. A combination of drugs may be
used to treat H. pylori including two antibiotics with an H2 antagonist (Amoxicillinor clarithromycin and Cimetidine).
The nurse monitors the client’s symptoms. Evaluating the client’s response to dietary
modifications and prescribed medications is important. The nurse observes the
colour and characteristics of any vomitus or stool that the client passes. In addition,
he or she teaches about diet, drug therapy, and the need for continued medical
follow-up. For complications such as ulcer formation, refer for better managementof peptic ulcer disease.
The preventive measures of gastritis may be encouraged to the general population
such as practicing good hygiene (hand- washing) to decrease the risk of H. pylori
infection transmission. H. pylori, can be contagious via the fecal-to-oral route. Good
hand washing before handling of foods and proper sanitation (sewer and water
systems) are the first line of defense against spread. Many people can develop
gastritis after being infected with H. pylori bacteria, minimizing indigestion and
heartburn as these conditions are linked to gastritis, avoiding fatty, spicy or acidic
foods, cutting back on caffeine, eating smaller meals throughout the day, managing
stress, not taking NSAIDs, reducing alcohol consumption and not lying down for 2to 3 hours after a meal would be taught to minimize the risk of contracting gastritis.
Evolution and complications
Most cases of gastritis improve quickly with treatment. For most people, medications
relieve gastritis. The healthcare provider will recommend the most appropriate
treatment based on what’s causing gastritis. Antacids reduce stomach acid, while
antibiotics clear up bacterial infections. The client can also make changes likereducing the alcohol consumption and managing pain without NSAIDs.
When the gastritis left untreated, it can lead to serious problems including
Anemia: H. pylori can cause gastritis or stomach ulcers (sores in the stomach)
that bleed, thereby lowering your red blood counts (called anemia). Pernicious
anemia due to the autoimmune gastritis can affect how the body absorbs vitamin
B12, which put the client at risk of pernicious anemia when there is not enough
B12 intake to make healthy red blood cells. Peritonitis may occur when stomach
ulcers are worse. Peritonitis may also be observed when ulcers are broken down
through the stomach wall thus causing stomach contents and spread of bacterial
to be found in the abdomen, which can lead later to sepsis and even death when
adequate measures are not taken timely. Stomach cancer: Gastritis caused by H.
pylori and autoimmune disease can cause growths in the stomach lining. Thesegrowths increase the patient‘s risk of developing stomach cancer.
Self-assessment 3.1
1. Define the term gastritis
2. Describe the causes and triggering factors contributing to the gastritis
development
3. What are different treatment options for a patient with acute gastritis?
4. State the preventive measures to be taken to prevent gastritis
5. What are possible investigations to be performed to confirm gastritis?6. If acute gastritis is not well treated, what could be the complications?
3.2 DIARRHEA
Learning Activity 3.2
Read carefully this below situation and answer the following questions:
Mr. B.V a 40 -year-old male was admitted to the emergency department of
RUHANGO Hospital where you are working as an Associate nurse. He came with
complains of headache, abdominal pain, discomfort and cramps (mesogastric
pain and epigastric pain), tiredness, anorexia, nausea, thirst, frequent watery
stool elimination with fats containing 5time a day. The history taking revealed
that he is from abroad where he took uncleaned food and drinks on the street
and bought water two days ago at the same area. Vital signs on admission were
as follows: body temperature was 36.5 degree Celsius, blood pressure 70/35
mmHg, pulse rate was 123bpm, and respiratory rate was 18 breaths per minutes.
Mr. B.V was urgently given ringer lactate 2litters bolus through intravenous and
the following investigations were performed: stool examination which revealed
amoebic infection, blood smear was negative. The patient was given loperamide
and oral rehydration salts to be taken home after intravenous rehydration.
1. What are the abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
4. What was included in the management of this case?5. What could be the appropriate topics of health education for this case?
In differentiating normal from abnormal, the consistency of stools and the comfort
with which a person passes them are more reliable indicators than is the frequency
of bowel elimination. The type and amount of food a person consumes greatlyaffect stool consistency.
Diarrhea is loss of watery stools (or bloody) for more than 3 times a day (more than
5 times a day for the neonates and small infants) or Diarrhea is the frequent passage
of larger-than-normal amounts of liquid or semiliquid stool (more than three bowel
movements per day). There are actually several different ways to classify diarrhea.
These types of diarrhea include:
• Acute diarrhea is loose watery diarrhea that lasts one to two days. This type
doesn’t need treatment and it usually goes away after a few days.
• Persistent diarrhea is a type of diarrhea that generally persists for severalweeks (two to four weeks).
• Chronic diarrhea is a diarrhea that lasts for more than four weeks or comesand goes regularly over a long period of time is called chronic diarrhea.
Causes and risk factors
Diarrhea is a common problem that can come suddenly or be a chronic complaint.
Some possible causes of diarrhea include food poisoning, infections, food allergies
or intolerances, and medication. There are also some conditions that cause chronic
diarrhea that run in families or, rarely, have a genetic basis.
Many different things can cause diarrhea in human gastro-intestinal tract in differentforms.
Acute diarrhea
Bacterial infections: Several types of bacteria consumed through contaminated
food or water can cause diarrhea. Common cause includes Campylobacter,
Salmonella, Shigella, and Escherichia coli (E. coli). If you eat something that
was improperly cooked or contaminated after cooking, the infection is called food
poisoning. Diarrhea, cramps, and vomiting are common with food poisoning.
Viral infections: Many viruses cause diarrhea, including rotavirus, Norwalk virus,
cytomegalovirus, herpes simplex virus, and viral hepatitis.
Food intolerances (maldigestion and or malabsorption syndrome): Some
people are unable to digest food components such as lactose; the sugar found in
milk, infants can also have milk-protein allergies.
Parasites: Parasites can enter the body through food or water and settle in the
digestive system. Parasites that cause diarrhea include Giardia lamblia, Entamoeba
histolytica.
Reaction to medicines (Medication): Antibiotics, cancer drugs (chemotherapy),
and antacids containing magnesium can all cause diarrhea, laxatives, digitalis,
metformin, cholesterol lowering agents, Lithium, Theophylline, Thyroid hormone
and colchicine.
Intestinal diseases: Inflammatory bowel disease, colitis, Crohn’s disease,
congenital aganglionic megacolon often lead to diarrhea.
Functional bowel disorders: Diarrhea can be a symptom of irritable bowel
syndrome
Too much caffeine or alcohol: there is a need to cut back on one or both to see if
that does the trick.
Toxins: such as insecticides, psychedelic mushrooms and arsenic cause diarrheatoo.
A digestive problem: this could be lactose intolerance, celiac disease or pancreaticproblems
A number of non-infectious medical conditions that may cause diarrhea including
inability to digest certain foods, including lactose intolerance (difficulty digesting
sugar found in dairy products); celiac disease (an immune reaction to consuming
gluten, a protein found in wheat, barley, and rye); and pancreatic problems, such as
those caused by cystic fibrosis, which interfere with production of important digestive
substances. Surgery to remove part of your small intestine. A shortened small
intestine may be unable to absorb all the substances you eat.
This is referred to as short-bowel syndrome. Surgical removal of the gallbladder.
An increase in bile in the colon may result in watery stools. Certain diseases of the
endocrine (hormonal) system, including overactive thyroid disease, diabetes,
adrenal disease, and Zollinger-Ellison syndrome. Certain rare tumors
(including carcinoid tumor and pheochromocytoma) that produce diarrhea-causing
substances (hormones). Inflammation in the intestinal tract, which can result in
chronic diarrhea. If you have inflammatory bowel disease (such as ulcerative colitis,
Crohn’s disease, or microscopic colitis), you will have regular bouts of diarrhea
during a flare-up of your disease. Irritable bowel syndrome, which may cause
alternating bouts of diarrhea and constipation. Ischemic bowel disease, which
can be caused by blocked arteries. Symptoms might include abdominal pain withbloody diarrhea.
Chronic diarrhea
Diarrhea that persists longer than 4 weeks is considered to be chronic
Major Causes of Chronic Diarrhea according to predominantpathophysiologic mechanism.
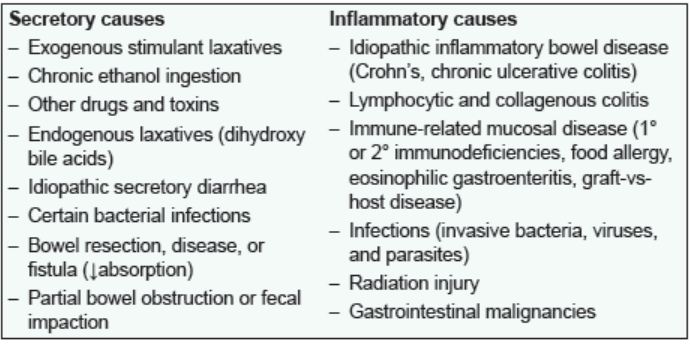
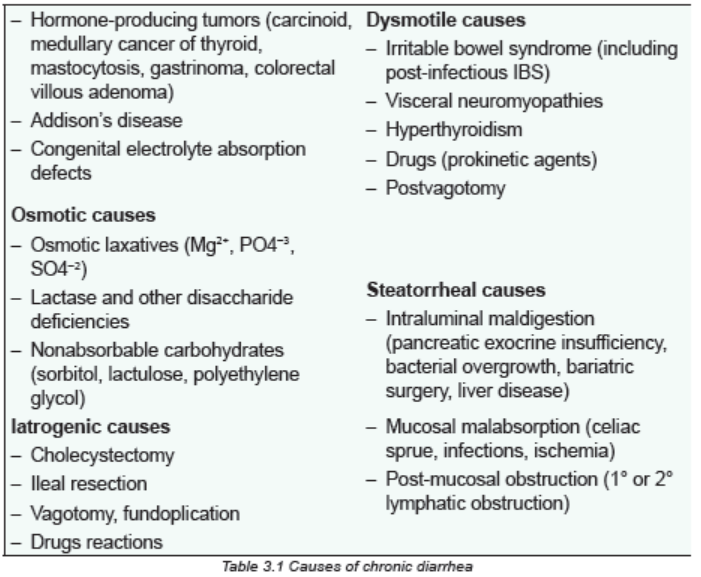
Pathophysiology overview
Diarrhea results from increased peristalsis, which moves fecal matter through the GI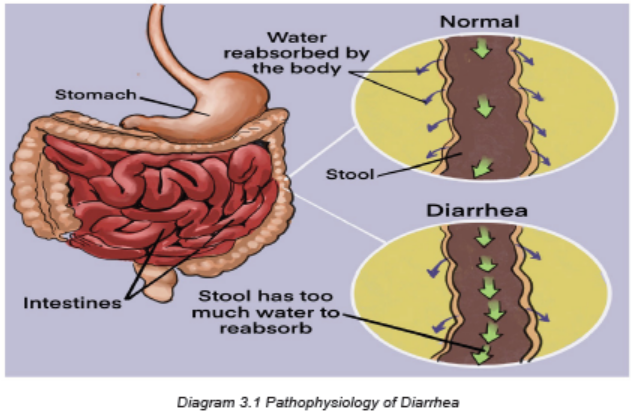
tract much more rapidly than normal. The swift velocity causes intestinal cramping
and decreases the time available for water to be absorbed from stool in the largeintestine. Consequently, the stool is either very soft or liquid.
Osmotic Diarrhea
Absorption of water in the intestines is dependent on adequate absorption of
solutes. If excessive amounts of solutes are retained in the intestinal lumen, water
will not be absorbed and diarrhea will result. Osmotic diarrhea typically results from
one of two situations: Ingestion of a poorly absorbed substrate, Malabsorption:
inability to absorb certain carbohydrates is the most common deficit in this categoryof diarrhea, but it can result virtually any type of malabsorption.
A common example of malabsorption, afflicting many adults humans and pets is
lactose intolerance. In such cases, a moderate quantity of lactose is consumed
(usually as milk), but the intestinal epithelium is deficient in lactase, and lactose
cannot be effectively hydrolyzed into glucose and galactose for absorption. The
osmotically-active lactose is retained in the intestinal lumen, where it “holds” water.
To add insult to injury, the unabsorbed lactose passes into the large intestine where
it is fermented by colonic bacteria, resulting in production of excessive gas.
A distinguishing feature of osmotic diarrhea is that it stops after the patient is fastedor stops consuming the poorly absorbed solute.
Secretory Diarrhea
Large volumes of water are normally secreted into the small intestinal lumen,
but a large majority of this water is efficiently absorbed before reaching the large
intestine. Diarrhea occurs when secretion of water into the intestinal lumen exceeds
absorption. Example in case of cholera, the Vibrio cholerae, produces cholera
toxin, which strongly activates adenylyl cyclase, causing a prolonged increase in
intracellular concentration of cyclic AMP within crypt enterocytes. This change results
in prolonged opening of the chloride channels that are instrumental in secretion of
water from the crypts, allowing uncontrolled secretion of water. Additionally, cholera
toxin affects the enteric nervous system, resulting in an independent stimulus of
secretion. Exposure to toxins from several other types of bacteria (e.g. E. coli
heat-labile toxin) induce the same series of steps and massive secretory diarrhea
that is often lethal unless the person or animal is aggressively treated to maintainhydration.
Inflammatory and Infectious Diarrhea
The epithelium of the digestive tube is protected from insult by a number of
mechanisms constituting the gastrointestinal barrier, but like many barriers, it can
be breached. Disruption of the epithelium of the intestine due to microbial or viral
pathogens is a very common cause of diarrhea in all species. Destruction of the
epithelium results not only in exudation of serum and blood into the lumen but often
is associated with widespread destruction of absorptive epithelium. In such cases,absorption of water occurs very inefficiently and diarrhea results.
The immune response to inflammatory conditions in the bowel contributes
substantively to development of diarrhea. Activation of white blood cells leads them
to secrete inflammatory mediators and cytokines which can stimulate secretion, in
effect imposing a secretory component on top of an inflammatory diarrhea. Reactive
oxygen species from leukocytes can damage or kill intestinal epithelial cells, which
are replaced with immature cells that typically are deficient in the brush border
enyzmes and transporters necessary for absorption of nutrients and water. In thisway, components of an osmotic (malabsorption) diarrhea are added to the problem.
Diarrhea Associated with Deranged Motility
In order for nutrients and water to be efficiently absorbed, the intestinal contents
must be adequately exposed to the mucosal epithelium and retained long enough
to allow absorption. Disorders in motility than accelerate transit time could decrease
absorption, resulting in diarrhea even if the absorptive process per se was
proceeding properly. Alterations in intestinal motility (usually increased propulsion)are observed in many types of diarrhea.
Signs and symptoms
The signs and symptoms of diarrhea depend on the cause. Symptoms and signs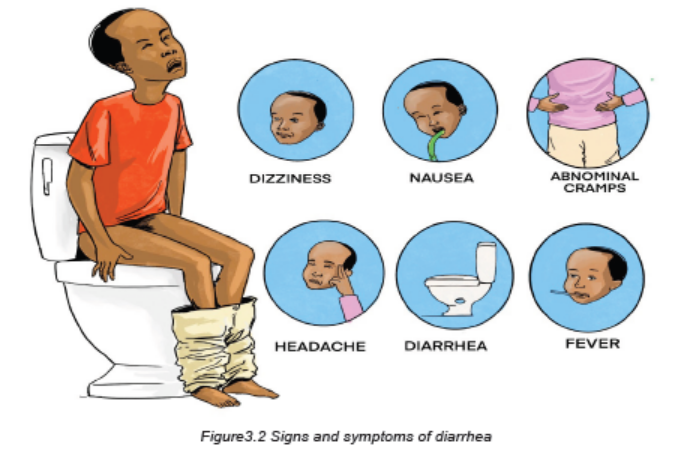
that often accompany with diarrhea may include: loose or watery stools for 4
weeks or longer in chronic diarrhea. The stools may be any color. The diarrhea
may appear even green in color, because stool passes through the intestines faster
than usual. Red stools indicate intestinal bleeding, so it may be a sign of a more
serious infection, bloating and gas, more frequent bowel movements, a sense of
urgency to pass stools, abdominal cramps, nausea, a burning sensation, fever,
dehydration. If diarrhoea causes dehydration, it is a sign of possibly severe health
issues. Some signs of dehydration are dark urine, dizziness and shakiness,
tiredness, fever, fatigue, dry mucous membranes, increased heart rate, a
headache, light-headedness, increased thirst, decreased urination, dry mouth.
In severe cases, blood and mucus pass with the stool. The client usually experiences
urgency (tenesmus) and abdominal discomfort. Bowel sounds are hyperactive.
Skin around the anus may become excoriated from contact with fecal matter
and products of the digestive process (e.g., gastric acid, bile salts). Fever may
be present. Infectious diarrhea typically has a sudden onset, with accompanyinggeneralized malaise.
Diarrhea in very young people is a serious condition. Seek urgent medical care
if any of the following symptoms apply to the child: diarrhea for 24 hours or more,
stools that contain blood, fever of 102°F (39°C) or higher, stools that contain pus,
stools that are black and tarry, signs and symptoms of dehydration (Dry mouth,
a headache, fatigue, a lack of tears when crying, dry skin, sunken eyes, Sunkenfontanel, sleepiness, irritability, decreased urination).
Investigations
Routine stool cultures are obtained to identify bacterial infections as the cause for
infectious diarrhea. Stool specimens obtained to identify parasites and their ova
are placed in special preservatives and analysed separately by the microbiology
department. Several samples may be needed because parasites are not typically
shed with each stool. Routine ova and parasite analysis may identify amoebic
infections; however, such infections may require serologic (blood) tests.
Blood in the stool may be common with certain infections and disease processes.
Nurses typically test stool specimens, collecting a specimen from the client (e.g.,
Hemoccult testing).
A proctosigmoidoscopy or colonoscopy may be performed to identify chronic
inflammation or alteration in the mucosal layer of the large intestine. These studies
often are carried out to identify the cause of chronic inflammation. An upper GI
series with small-bowel follow-through allows for radiologic examination of the
small bowel and identification of inflammation. Upper GI endoscopy allows foridentification of malabsorptive disorders such as celiac disease.
Adequate Medical Diagnosis
For the majority of mild diarrhea cases, there is no need for medical attention.
These cases are self-limited (only lasts for a fixed amount of time) and get better
without medical intervention. The key to mild diarrhea is supportive therapy –
staying hydrated and eating a bland diet. More serious cases of diarrhea may
require medical attention. In these situations, there are a few diagnostic tests that
the health care provider may order to determine the diagnosis. These tests can
include:
• Discussing a detailed family history, as well as physical and medical conditions,
the travel history, and any sick contacts the client may have.
• Doing a stool test on a collected stool sample to check for blood, bacterial
infections, parasite and inflammatory markers.
• Doing a breath test for lactose or fructose intolerance checkup and bacterial
overgrowth.
• Doing blood work to rule out medical causes of diarrhea such as a thyroid
disorder, celiac sprue (immune reaction to eating gluten, a protein found in
wheat, barley and rye) and pancreatic disorders.
• Doing endoscopic evaluations of the upper and lower digestive tract to ruleout organic abnormalities (ulcers, infections, neoplastic process).
Treatment plan
Treatment of diarrhoea that is mild or of short duration, such as that caused by
dietary changes or acute illness, involves resting the bowel by limiting intake to
clear liquids for one or two meals and gradually advancing to a regular diet. When
diarrhoea persists and stools are frequent and large, or if the person is very young,
elderly, or debilitated, medical treatment may include one or more of the followingmeasures:
• Administration of an antidiarrheal agent, such as diphenoxylate hydrochloride
with atropine sulfate (Lomotil), loperamide hydrochloride (Imodium), or a
combination product such as kaolin and pectin (Kaopectate)
• Fluid and electrolyte replacement by either the oral or intravenous (IV) route
• Dietary adjustments, which may involve eliminating foods that cause diarrhea.
Foods such as mashed potatoes, pasta, bread made with white flour, white
rice, and low fiber cereals are easy to tolerate. Yogurt is usually well tolerated
and contains probiotics that promote the growth of healthy GI bacteria. Milk
should be avoided for a few days because lactose intolerance may occur
during periods of acute diarrhea.
• Encourage potassium-rich foods as tolerated. Examples include bananas,
canned apricots and peaches, apricot nectar, orange juice, grapefruit juice,
tomato juice, fish, potatoes, and meat. Encourage client to withhold foods
until the acute attack subsides. Withholding food rests, the bowel and slows
peristalsis.
• Total parenteral nutrition (TPN) if diarrhea is severe and prolonged and if the
introduction of oral fluid and food results in another episode of diarrhea
• Reintroducing food after a bout of diarrhea usually calls for a diet low in
insoluble fiber to reduce the volume of stool. Insoluble fiber is found mostly
in whole grains, high-fiber cereals, raw vegetables, corn, nuts, seeds, and
the skins and seeds of fruit. Foods high in soluble fiber help slow GI motility;
examples include oatmeal, ripe bananas, and applesauce.
• Give clear liquids as tolerated, but limit high-sugar drinks. Drinking clear
liquids prevents dehydration; high-sugar drinks have high osmolality, which
may aggravate diarrhea.
• Advance oral intake as tolerated, initially offering foods high in soluble fiber
such as oatmeal, ripe bananas, and applesauce. Soluble fiber helps slow GI
motility.
• Teach client to avoid foods high in insoluble fiber, such as whole grain bread
and cereals, bran cereals, and raw vegetables. Caffeinated and carbonated
beverages should also be avoided. Such items stimulate GI motility.
• Encourage the intake of yogurt. Yogurt contains probiotics that help promotethe growth of healthy GI bacteria.
• Administer antidiarrheal medications as ordered for prolonged diarrhea.
These medications slow intestinal motility and inhibit peristalsis.
• Encourage client to rest in a comfortable position with legs bent toward the
abdomen. This position relaxes abdominal muscles and reduces discomfort.
• Advise client to avoid carbonated beverages or drinking with a straw. These
increase volume of swallowed air, which in turn increases gas and cramping.
The treatment of diarrhea focuses of signs and symptoms, etiology (antibiotics if
needed, etc) and aiming at preventing complications.
Preventive measures
The general preventive measures for diarrhea includes:
Improving sanitation mainly drinking water and sanitation lead to decreased risks
of diarrhea. Such improvements might include for example use of water filters,
provision of high-quality piped water and sewer connections.
Hand washing: Basic sanitation techniques can have a profound effect on the
transmission of diarrheal disease. The implementation of hand washing using soap
and water, for example, has been experimentally shown to reduce the incidence of
disease by approximately 30–48.
Vaccination: Immunization against the pathogens that cause diarrheal disease is a
viable prevention strategy, however it does require targeting certain pathogens for
vaccination such as Rotavirus vaccine.
Nutrition: dietary deficiencies in developing countries can be combated by
promoting better eating practices. Zinc supplementation proved successful showing
a significant decrease in the incidence of diarrheal disease compared to a control
group.
Breastfeeding practices have been shown to have a dramatic effect on the
incidence of diarrheal disease in poor populations. Studies across a number of
developing nations have shown that those who receive exclusive breastfeeding
during their first 6 months of life are better protected against infection with diarrheal
diseases.
Evolution and complications of diarrhea
Diarrhea is extremely common, but that doesn’t mean it can’t be dangerous. In
extreme cases of diarrhoea, a patient with diarrhoea can become very dehydrated
and this can lead to serious complications including hypovolemic choc and death
if poorly managed. Dehydration is one of the most dangerous side effects of
diarrhea. In the very young infants, small children and the very old this can haveserious consequences.
Diarrhea is a life-threatening condition because of dehydration and electrolyte
loss. The following are severe signs of dehydration: low blood sugar, fever and
chills, changes in breathing patterns, altered mental state, skin that when pinched
doesn’t immediately go back into place. If severe dehydration persists or is poorly
managed, it can lead to kidney failure, loss of consciousness, shock, coma, anddeath.
Self-assessment 3.2
1. Distingwish acute from chronic diarrhea.
2. State at least any five causes of diarrhoea disease development
3. What are treatment options for a patient with diarrhoea disease?
4. State at least three preventive measures to be taken to prevent diarrhoea
disease
5. What are possible investigations to be performed to rule out diarrhoeadisease?
3.3 CONSTIPATION
Learning Activity 3.3
Read carefully this below situation and answer the following questions:
A 40-year-old woman reports having infrequent bowel movements and bloating.
For many years, she typically has had bowel movements of hard, pellet-like stools
every two or three days. Over the last year, they have decreased in frequency to
every three or four days and are preceded by bloating and discomfort in the left
lower quadrant. The patient also usually strains excessively to pass stools. Vital
signs on admission were as follows: body temperature was 36.5 degree Celsius,
blood pressure 100/70 mmHg, pulse rate was 80bpm, and respiratory rate was
18 breaths per minutes. She was put on laxative drugs such as busacodyl as
stool softeners and encouraged fiber food intake and doing regular physicalexercise.
1. What are the abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What was included in the management of this case?
4. What could be the appropriate topics of health education for betterprevention of the above medical condition?
Constipation is known as difficulty in evacuation of faeces that may be accompaniedby the inability to defecate.
Causes and risk factors of constipation
• Irregular bowel habits, ignoring the need to defecate
• Chronic illness; e.g. Parkinson disease
• Low fibre diet and high animal fat intake
• Lack of fluid intake
• Stress
• Lack of physical exercises
• Colon cancer
• People depending on heavy laxative drugs
• Old age
Pathophysiology
Constipation is a condition in which stool becomes dry, compact, and difficult and
painful to pass. Normally, fecal matter collects in the rectum and presses on the
internal anal sphincter, creating an urge to defecate (eliminate stool). Peristalsis
and distention of the colon facilitate the signal to release stool. The gastrocolic
reflex facilitates stool passage by accelerating peristalsis. This reflex is most active
after eating, particularly after the first meal of the day. A diet low in fiber predisposes
people to constipation because the stools produced are small in volume and dry.
The lower GI tract propels low-volume stools more slowly. Whenever stool remains
stationary in the large intestine, moisture continues to be absorbed from the residue.
Consequently, retention of stool for any number of reasons, causes stool to become
dry and hard.
Rectal bleeding may result as the tissue stretches and tears while the person tries
to pass the hard, dry stool. When a practitioner inserts a gloved and lubricated
finger in the rectum, the stool may feel like small rocks, a condition referred to as
scybala (hardened masses of feces). Sometimes, if the client has been constipated
for a long time, he/she may begin passing liquid stool around an obstructive stool
mass (encopresis), a phenomenon sometimes misinterpreted as diarrhea. The
liquid stool results from dry stool stimulating nerve endings in the lower colon and
rectum, which increases peristalsis. The increased peristalsis sends watery fecesfrom higher in the bowel than the retained stool.
Signs & Symptoms
– Abdominal pain
– Bloating
– Staining during defecation
– No stool for 3 consecutive days or solid stool of inadequate volume...
– Fewer than three bowel movements a week
– Hard, dry, or lumpy stools
– Straining when using the bathroom
– Taking a long time to pass stools
– Feeling like having not passed all the stool
– Distention (bloating) of the belly
– Traces of liquid or clay-like stool in your child’s underwear—this can be a sign
that the stool is backed up in the rectum
– Blood on the surface of hard stool
– Fussiness and crying in infants in children
– Decreased appetite in infants and children
– Other odd behavior in infants and children
Investigations
A thorough history and physical examination (including digital rectal exam)
are necessary to determine the underlying cause and need for further diagnostic
testing. Frequently the diagnosis is based on findings of the history and physicalexamination, precluding the need for a more aggressive approach.
Abdominal radiography helps determine the extent of the constipation. A barium
enema is performed if a structural abnormality is suspected. In defecography, a
thick barium paste is inserted into the rectum. Radiographs are taken as the client
expels the barium to determine whether there are any anatomic abnormalities or
problems with the muscles surrounding the anal sphincter.
Colonic transit or marker studies are used to determine how long it takes for food
to travel through the intestines. For one or more days, clients swallow capsules
or solutions that contain radiographically visible plastic particles. After some days,
radiographs are taken to determine whether any particles are left and if so, where
they are. The location of the particles can help determine whether there is colonic
inertia related to muscle and/or nerve impairment or pelvic floor dysfunction.
Anorectal motility and/or colonic motility studies may be performed to confirm
a motility disorder. These studies use flexible catheters with sensors that measure
the pressure of muscle contractions.
Lower gastrointestinal (GI) endoscopy, sigmoidoscopy, and Colonoscopy
that represents the current criterion standard can also be done.
Other investigations to be considered are complete blood count (CBC), thyroid
function tests, blood glucose, serum electrolytes (sodium, potassium,
calcium, and magnesium).
Adequate Medical diagnosis
Functional constipation is clinical diagnosis that can generally be made on the basis
of typical history and an essentially normal physical examination including one of
the rectal examination is a key part of the initial evaluation.
Treatment plan of Constipation
Treating the cause provides the best relief. For quick symptomatic relief, the
physician prescribes an enema or a laxative in oral or suppository form, followed by
prophylactic administration of a stool softener. Diet therapy: encourage fibre food
intake (green vegetables, fruits like papaya), fluid intake, advice physical exercises,
enema (cleansing) may be required, laxative: e.g. Oral polyethylene glycol is better
tolerated.
Evolution and complications
Short term constipation typically does not cause complications and can usually
be treated with self-care. For example, if a patient is simply constipated due to a
change in the diet, he/she may feel full or bloated, but will not have any long-termcomplications. However chronic constipation can cause complications:
Hemorrhoids: are swollen and inflamed veins in the rectum or anus. They can
occur inside or outside and are usually not serious. External hemorrhoids may
cause itchiness or pain when having a bowel movement. Internal hemorrhoids
typically do not cause pain and, instead, you may see bright red-streaked stool in
the toilet.
Anal Fissures: are usually the result of some form of trauma to the anus, like hard
stool. Anal fissures are usually painful and may also cause itching. Client may also
notice blood on the toilet tissue or on the stool.
Rectal prolapse: occurs when the last portion of the colon, the rectum, protrudes
beyond the anus and is visible on the outside of the body. It is not necessarily
painful, and in many cases will go away without treatment. It should be evaluated
by the healthcare provider, though.
Faecal impaction: is a state of prolonged constipation. It occurs when the
stool is so hard that it cannot pass with a normal bowel movement. It can cause
abdominal pain and cramping, among other symptoms. It often must be treated with
medications or procedures such as enemas or water irrigation. Chronic constipation
can lead to fecal impaction and fecal incontinence. They state that in severe cases,
fecal impaction can cause stercoral ulcerations, intestinal obstruction, or bowel
perforation. If left untreated, these complications can be life-threatening.
Self-assessment activity 3.3
A 37-year-old woman comes to your clinic for “constipation,” that she had since
childhood. She states that a work-up by her paediatrician turned up nothing. She
reports intermittent crampy abdominal pain that reaches 8 out of 10 in severity
and is relieved “mostly” by a bowel movement. She has a bowel movement
nearly every day, but her stools are usually hard. When the pain occurs, her
stools are “really hard”. She was recently laid off from her job and has noted an
increase in her abdominal pain and hard stools.
1. What additional questions would you ask to learn more about her
symptoms?
2. What is constipation?
3. State at least any five causes of constipation disease development
4. What are possible investigations to be performed to rule out constipation
disease?
5. What are treatment options for a patient with constipation disease?
6. State at least three preventive measures to be taken to prevent constipation
disease.7. What are the complications of chronic constipation?
3.4 END UNIT 3 ASSESSMENT
End of unit assessment
1. Nursing management of the patient with chronic gastritis includes teaching
the patient to
a. Take antacids before meals to decrease stomach acidity.
b. Maintain a nonirritating diet with six small meals a day.
c. Eliminate alcohol and caffeine from the diet when symptoms occur.
d. Use nonsteroidal antiinflammatory drugs (nsaids) instead of aspirin for
minor pain relief.
2. A nurse is doing a nursing assessment on a patient with chronic constipation.
What data obtained during the interview may be a factor contributing to the
constipation?
a. Taking methylcellulose (Citrucel) daily
b. High dietary fiber with high fluid intake
c. History of hemorrhoids and hypertension
d. Suppressing the urge to defecate while at work
3. Which method is preferred for immediate treatment of an acute episode of
constipation?
a. An enema
b. Increased fluid
c. Stool softeners
d. Bulk-forming medication
4. A patient is admitted to the emergency department with acute abdominal
pain. What nursing intervention should the nurse implement first?
a. Measurement of vital signs
b. Administration of prescribed analgesics
c. Assessment of the onset, location, intensity, duration, and character of
the pain
d. Physical assessment of the abdomen for distention, bowel sounds, and
pigmentation changes
5. A 22-year-old patient calls the outpatient clinic complaining of nausea and
vomiting and right lower abdominal pain. What should the nurse advise the
patient to do?
a. Use a heating pad to relax the muscles at the site of the pain.
b. Drink at least 2 quarts of juice to replace the fluid lost in vomiting.
c. Take a laxative to empty the bowel before examination at the clinic.
d. Have the symptoms evaluated by a health care provider right away.
6. The appropriate collaborative therapy for the patient with acute diarrhea
caused by a viral infection is to:
a. Increase fluid intake.
b. Administer an antibiotic.
c. Administer antimotility drugs.
d. Quarantine the patient to prevent spread of the virus.
7. What are the preventive strategies of constipation?
8. What are the investigations to request for a patient with constipation?
9. What are the investigations to request for diagnosing gastritis?
10. What must be included into the treatment plan of gastritis?
11. What are the treatment modalities of diarrhea?
12. Discuss different risk factors of gastritis.
13. Referrring to pathophysiology, differentiate the osmotic, secretory andinflammatory diarrhea.
UNIT 4 MEDICAL PATHOLOGIES OF UROGENITAL SYSTEM
Key Unit Competencies
To take an appropriate decision on management of different common medicalpathologies of urogenital system.
Introductory activity 4.0
Observe the image below and answer the questions that follow.
Figure 4.1 Urinary tract infection
1. What do you observe on the picture?
2. What do you think will happen if the microorganisms enter in the urinary
system?3. How do you think the microorganisms can enter in the urinary system?
4.1 URINARY TRACT INFECTION (UTI)
Learning Activity 4.1
Carefully read the case below and answer the following questions:
A.K., man of 45 years old was brought at Muhima Hospital in a private car with
his knees bent and drawn to his abdominal area. In the history, he reported to
have unprotected sex 3 days ago with a person whom he doesn’t know. He
appears restless and keeps moving from back to side in an effort to reduce his
discomfort. At arrival, the vital signs were blood pressure 156/70 mmHg, Pulse
108 beats per minute, respiratory rate 24 cycles per minute, temperature 37.4° C,
O2 saturation 96% on room air. He was awake, alert, and oriented. Lungs were
clear on auscultation. The abdomen not distended with positive bowel sounds in
all 4 quadrants and no rebound tenderness. He had costovertebral tenderness
and mild pain when palpating the hypogastric pain (lower parts of the abdomen).
He was voiding small amounts (pollakyuria) of chocolate urine with aromatic odor
and had burning during urination (dysuria). From the investigations done, the
patient had elevated white blood cells of 13000, and the abdominal ultrasound
and urine culture were pending. The health care provider prescribed opioids forpain management, IV fluids and admitted A.K for further management.
1. Basing on case described, what are the abnormal signs and symptoms the
patient was presenting?
2. What are the investigations that have been requested to that patient? What
were their rationales?
3. What was the medical problem that the patient was presenting?
4. From the case study and what you know, what are all possible causes or
risk factors to develop that medical condition?
5. What must be included into the management plan of that medical condition?
6. If not treated, what might be the consequences?
Adequate kidney function is essential to the maintenance of a healthy body. The
upper urinary system consists of two kidneys and two ureters. The lower urinary
system consists of a urinary bladder and a urethra. Urine is formed in the kidneys,
drains through the ureters to be stored in the bladder, and then passes from the
body through the urethra.
The kidneys have also many other functions including excreting excess water andnitrogenous waste products of protein metabolism, assisting in maintenance of acid
base and electrolyte balance, producing the enzyme renin, which helps regulate
blood pressure, and producing the hormone erythropoietin, which stimulates
red blood cell production. The remainder of the urinary system is involved in thetransport (ureters), storage (bladder), and excretion (urethra) of urine.
Renal and urologic disorders encompass a wide spectrum of problems. The
diverse causes of these disorders may involve infectious, immunologic, obstructive,
metabolic, collagen, vascular, traumatic, congenital, neoplastic, and neurologicmechanisms.
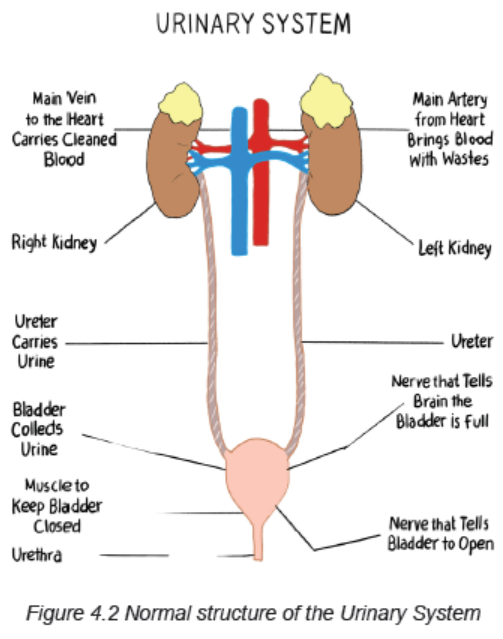
Urinary tract infection (UTI) is an inflammation of the urinary epithelium in response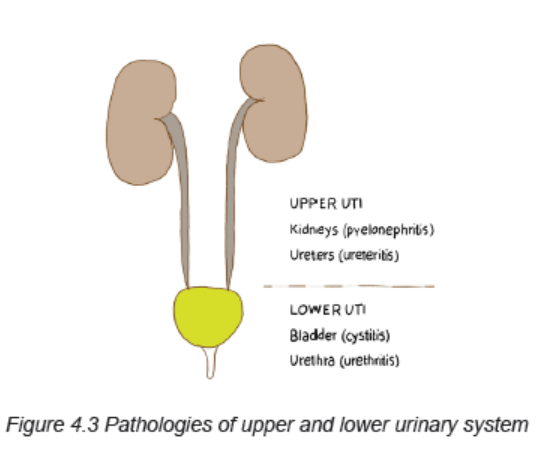
to colonization from a pathogen. The urinary tract infections can be classified as
complicated or uncomplicated. Uncomplicated UTI occur in a normal urinary tract
and usually involve only the bladder. Complicated UTI include those infections with
coexisting obstruction, stones, or catheters, diabetes or neurologic diseases, or
pregnancy-induced changes. The term Complicated UTI also applies to a recurrent
infection. The individual with a complicated infection is at risk for pyelonephritis,
uro-sepsis, and renal damage.
The most common urologic disorders are infectious and inflammatory conditions.
Those that affect the kidneys are extremely dangerous because damage to the
nephrons can result in permanent renal dysfunction.
The bladder is usually free from bacteria and the urinary tract above the urethra is
normally sterile. Several mechanical and physiologic defense mechanisms assist
in maintaining sterility and preventing urinary tract infection (UTI). These defenses
include normal voiding with complete emptying of the bladder, ureterovesical
junction competence, and ureteral peristaltic activity that propels urine toward the
bladder. Antibacterial characteristics of urine are maintained by an acidic pH (less
than 6.0), high urea concentration, and abundant glycoproteins that interfere with
the growth of bacteria. An alteration in any of these defense mechanisms increasesthe risk for a UTI.
Types of UTI
– Uncomplicated (isolated) UTI is either a 1st infection or an infection that
occurs at least 1 year after any prior UTI.
– Recurring UTI is diagnosed when the person experiences an initial infection
that is successfully treated, followed by reappearance of the infection no
sooner than 5 to 10 days after resolution of the original episode.
– Persistent UTI is persistence of infection despite at least 3 days of treatment
with an antibiotic.
Causes and risk factors
Inflammation of the urinary tract may be caused by a variety of disorders, but
bacterial infection is the most common.
The organisms that usually cause UTI are introduced via the ascending route from
the urethra and originate in the perineum.
The commonest causes of UTI are:
– Bacteria which are the most common cause of UTI (Escherichia coli, Neisseria
gonorrhea, Chlamydia trachomatis, Klebsiella, Proteus, Staphylococcus,
mycoplasma, Pseudomonas)
– Fungi (Candida albicans)
– Viruses
– Parasites (e.g. Trichomonas Vaginalis)
Another common factor contributing to ascending infection is urologic instrumentation
(e.g., catheterization, cystoscopic examinations). This instrumentation allows
bacteria that are normally present at the opening of the urethra to enter into the
urethra or bladder.
Sexual intercourse promotes “milking” of bacteria from the vagina and perineum
and may cause minor urethral trauma that predisposes women to UTI.
Rarely the UTI result from a hematogenous route, where blood-borne bacteria
secondarily invade the kidneys, ureters, or bladder from elsewhere in the body.
There must be prior injury to the urinary tract, such as obstruction of the ureter,
damage caused by stones, or renal scars, for a kidney infection to occur from
hematogenous transmission.
Other risk factors of UTI are premature infants, sexually active women, women using
a diaphragm and spermicide, individuals with diabetes mellitus, individuals with
advanced HIV or immunosuppressive disorders, people with recent instrumentation
of urinary system or indwelling catheterization, people with obstruction of the lower
urinary tract.
Pathophysiology overview
A UTI occurs when a pathogen overwhelms the host’s defense mechanisms and
colonizes the urinary system with proliferation of bacteria, fungi, or parasite and
the person raises a response to this invasion. The ability of the bacteria to adhere
(attach) to the uro-epithelium influences its virulence. Adherence enhances bacterial
persistence despite micturition that increase the risk for recurring UTI.
Causes of bacterial persistence include bacterial resistance to the antibiotic,
emergence of resistant secondary bacterial strain after the primary microorganism
is eradicated, renal insufficiency causing poor excretion of the antibiotic in the urine,a foreign body such as stone acting as a harbor for bacteria, and papillary necrosis.
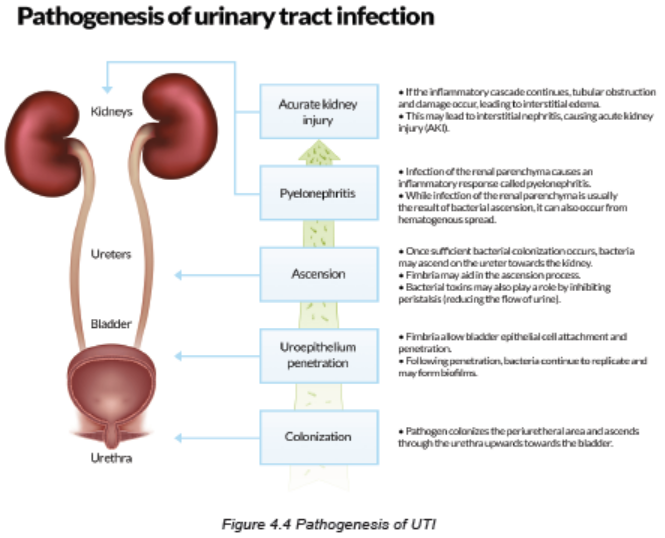
Signs and Symptoms
Lower urinary tract symptoms are experienced in patients who have UTI of the
upper urinary tract, as well as those confined to the lower tract. Symptoms are
related to either bladder storage or bladder emptying. These symptoms include
dysuria, frequent urination (more than every 2 hours), urgency, and suprapubic
discomfort or pressure. The urine may contain grossly visible blood (hematuria) or
sediment, giving it a cloudy appearance. Flank pain, chills, and fever indicate an
infection involving the upper urinary tract (pyelonephritis). People with significant
bacteriuria may have no symptoms or may have nonspecific symptoms such as
fatigue or anorexia.
The UTI symptoms are often absent in older adults as they tend to experience
non localized abdominal discomfort rather than dysuria and suprapubic pain. In
addition, they may have cognitive impairment or generalized clinical deterioration.
The older adults are less likely to experience a fever with a UTI, the value of body
temperature as an indicator of a UTI is unreliable.
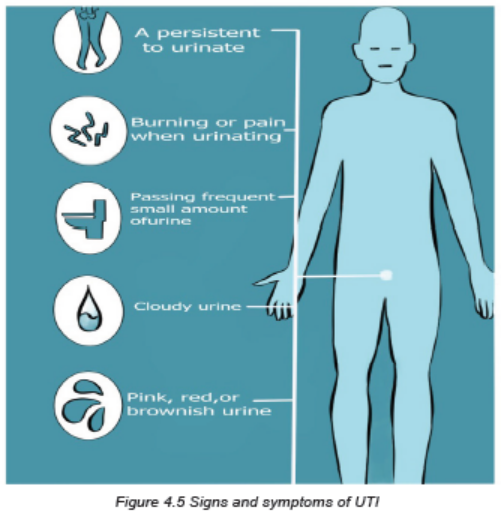
Investigations
In a patient suspected of having a UTI:
• Initially obtain a dipstick urinalysis to identify the presence of nitrites
(indicating bacteriuria), white blood cells (WBCs), and leukocyte esterase (an
enzyme present in WBCs indicating pyuria). These findings can be confirmed
by microscopic urinalysis.
• After confirmation of bacteriuria and pyuria, a urine culture may be obtained.
A urine culture is indicated in complicated UTI, persistent bacteriuria, or
frequently recurring UTI (more than two or three episodes per year). Urine
may also be cultured when the infection is unresponsive to empiric therapy
or the diagnosis is questionable. A urine culture is accompanied by sensitivity
testing to determine the bacteria’s susceptibility to a variety of antibiotic drugs.
• Imaging studies of the urinary tract like intravenous pyelogram (IVP),
cystoscopy, ultrasound can be performed. A computed tomography (CT)
urogram or ultrasound may be obtained when obstruction of the urinary
system is suspected or UTI occurs.
Adequate medical diagnosis
Most patients with urinary tract infection (UTI) can be managed as outpatients.
Indications for hospitalization include clinical uro-sepsis, immunocompromised
patient, vomiting or inability to tolerate oral medication, lack of outpatient followup,
and failure to respond to outpatient therapy. Empiric antimicrobial therapy
immediately after appropriate urine collection is warranted from patients with a high
probability of UTI based on the clinical and laboratory data available. Definitive
therapy is based upon the results of urine culture and sensitivities. There are other
investigations that must be performed like imaging.

Treatment plan
The goals of treatment of UTI include:
• Elimination of infection and prevention of uro-sepsis
• Relief of acute symptoms (eg, fever, dysuria, frequency)
• Prevention of recurrence and long-term complications including hypertension,
renal scarring, and impaired renal growth and function.
• Treatment to be effective should be oriented to both people if it is a couple
Interventions that must be carried out to meet those goals are:
• Ensuring adequate fluid intake if it is not contraindicated. Maintaining
adequate fluid intake may be difficult because of the patient’s perception that
fluid intake will worsen the discomfort and urinary frequency associated with
a UTI. Tell patients that fluids will increase frequency of urination at first but
will also dilute the urine, making the bladder less irritable. Fluids will help flush
out bacteria before they have a chance to colonize in the bladder. Caffeine,
alcohol, citrus juices, chocolate, and highly spiced foods or beverages should
be avoided because they are potential bladder irritants.
• Application of local heat to the suprapubic area or lower back may relieve the
discomfort associated with a UTI. Advise the patient to apply a heating pad
(turned to its lowest setting) against the back or suprapubic area. A warm
shower or sitting in a tub of warm water filled above the waist can also provide
temporary relief.
• Instruct the patient about the prescribed drug therapy, including side effects.
Emphasize the importance of taking the full course of antibiotics. Often
patients stop antibiotic therapy once symptoms disappear. This can lead to
inadequate treatment and recurrence of infection or bacterial resistance to
antibiotics.
• Instruct the patient to monitor for signs of improvement (e.g., cloudy urine
becomes clear) and a decrease in or cessation of symptoms. Teach patients
to promptly report any of the following to their health care provider: (1)
persistence of bothersome UTI beyond the antibiotic treatment course, (2)
onset of flank pain, or (3) fever.
• Antibiotic medications are necessary for the UTI. For treatment of uncomplicated
UTI, oral (by mouth) antibiotics are usually adequate. However, for major
complications such as sepsis or pyelonephritis, intravenous (IV) antibiotics
may be typically necessary. The antibiotics usually used are Nitrofurantoin
(Macrobid), Fosfomycin (Monurol), Trimethoprim-Sulfamethoxazole (Bactrim
and others), Cefixime, Cefuroxime, Cefotaxime or Ceftriaxone, Gentamicin,
Ciprofloxacin (Cipro) or Levofloxacin (Levaquin). Doxycicline or Erythromycin
can also be provided. Metronidazole will be needed in case of Trichomonas
infection or Nystatine in case of candida infection. The choice of regimen
depends on Antimicrobial spectrum and susceptibility, where the ultimate
choice of antimicrobial therapy is based upon the susceptibilities of the
organism isolated. Cephalosporins are the first-line oral agent in the treatment
of UTI among patients without genitourinary abnormalities. Amoxicillin and
ampicillin are not routinely recommended for empiric therapy because of the
high rate of resistance of E. coli.
• Inpatient parenteral therapy: this will require hospitalisation and the parenteral
therapy generally is indicated for the following cases: <2 months, clinical
urosepsis (eg, toxic appearance, hypotension, poor capillary refill), immune
compromise, vomiting or inability to tolerate oral medication, lack of adequate
outpatient follow-up (eg, no telephone, live far from hospital, etc), failure to
respond to outpatient therapy.
• Adjunctive therapies might be used to reduce the renal parenchymal
inflammation which if not treated leads to renal scarring. The therapies used
are anti-inflammatory drugs like Dexamethasone, Prednisolone, etc.
Evolution and complications
If all prescribed regimen are respected, the outcome is very good. Without treatment,
UTI can cause major health problems. Severe effects of a UTI that can develop
include:
• Pyelonephritis (acute or chronic): An infection involving the kidneys
• Sepsis: A dangerous, systemic, whole-body infection
• Renal scarring: due to chronic inflammation of renal parenchyma
• Hypertension: related to ineffective Angiotensin-Renin-Aldosteron
Self-assessment 4.1
1. What are all possible causes or risk factors to develop the urinary tract
infections?
2. What are the signs and symptoms of urinary tract infections?
3. What are the investigations that should be requested to make the diagnosis
of urinary tract infections?
4. What are their rationales?
5. What must be included into the management plan of that medical condition?
6. If not treated, what are the complications of UTIs?
4.1.1 URETHRITIS
Learning Activity 4.1.1
Carefully read the case below and answer the following questions:
A male patient aged around 25 years came to our hospital with the complaints
of discharge per urethra since 2 days. He also had burning micturition since
10 days which was followed 12 hours later by foul smelling white discharge
from urethra which continued to be present till the day he visited the hospital.
He also gave history of unprotected sexual intercourse with a commercial sex
worker 2 days prior to the onset of all symptoms. On examination, there was
mucopurulent discharge from urethra.
The meatus was cleaned using gauze soaked in saline. The discharge was
collected using a sterile swab under aseptic precautions. It was processed
for Gram staining and showed many pus cells and intracellular gram negative
diplococci, with adjacent sides concave (Kidney shaped). On chocholate agar
colonies were small, round, slightly raised and greyish white. Gram staining was
done from the colonies which showed gram negative diplococci. He was treated
with ciprofloxacin 500mg two times a day for 10 days, metronidazole 2gr single
dose and doxycycline 100mg two times a day and ibuprofen 400mg three times
a day for 3 days.
1. What are the possible medical conditions of this patient?
2. What are the signs and symptoms of this medical condition?
3. What are the causes of this above medical condition?
4. What are the investigations that should be used to diagnose that medical
condition?
5. Propose the treatment plan regarding this medical condition
6. If the patient is not well treated what are possible complications?
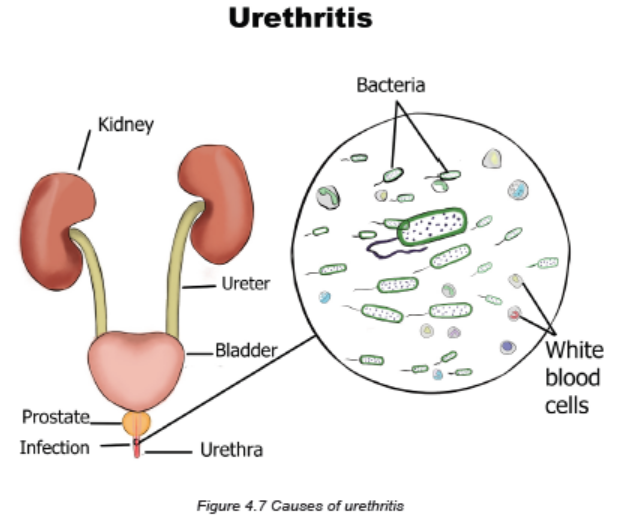
Urethritis is an inflammation of urethra that is the tube that carries urine from the
bladder to outside the body.
Causes and risk factors
Urethritis is an inflammatory condition that can be infectious or posttraumatic
in nature. Infectious causes of urethritis are typically sexually transmitted and
categorized as either gonorrhoea urethritis (ie, due to infections with Neisseria
gonorrhoeae) or non-gonorrhoea urethritis (eg, due to infections with Chlamydia
trachomatis, Ureaplasma urealyticum, Mycoplasma hominis, Mycoplasma
genitalium, or Trichomonas vaginalis). Bacteria that normally are present cause
no difficulty unless these tissues are traumatized, usually after instrumentation
such as catheterization or cystoscopic examination. Other causes of nonspecific
urethritis in men include irritation during vigorous intercourse, rectal intercourse, or
intercourse with a woman who has a vaginal infection.
Urethritis is seen more commonly in men than in women. In women, urethritis may
accompany cystitis but also may be secondary to vaginal infections. Soaps, bubble
baths, sanitary napkins, or scented toilet paper also may cause urethritis. In men, a
common cause of urethritis is infection with Chlamydia trachomatis or Ureaplasma
urealyticum, which causes an STI. The distal portion of the normal male urethra is
not totally sterile.
Pathophysiology
The pathogenesis of urethritis depends on the causative pathogen. N.
gonorrhea is usually transmitted via the genital tract to the human host. Following
attachment to host cell, which is mediated by pili, gonococci become engulfed
in a process known as parasite-directed endocytosis. This organism will survive
inside the vacuoles and replicate. Among non-gonorrheal causes, Chlamydia
trachomatis is the most common. The infectious process begins with cell surface
attachment and phagocytosis by the host cell. The pathogen survives inside
the cell by debilitating the cellular lysosomes and replicating as elementary bodies
which is considered as the infective form of the pathogen.
Signs and symptoms
Infection of the urethra results in discomfort on urination varying from a slight
tickling sensation to burning or severe discomfort and urinary frequency. Fever is
not common, but fever in the male client may be due to further extension of the
infection to areas such as the prostate, testes, and epididymis.
Urethritis can cause itching, pain, or discomfort when a person is not urinating, pain
during sexual intercourse, discharge from the urethral opening or vagina, in men
there can be blood in the semen or urine.
Investigations
The diagnosis of urethritis relies on:
• Physical examination that includes the genitals, abdomen, and rectum.
• Urine tests and culture for gonorrhea, chlamydia, or other bacteria.
• Examination of any discharge under a microscope
• Blood tests may be done in certain situations.
Adequate medical diagnosis
The client’s history and symptoms often provide a tentative diagnosis. In men,
a urethral smear is obtained for culture and sensitivity to identify the causative
microorganism. In women, a urinalysis (clean-catch midstream specimen) may
identify the causative microorganism.
Treatment plan
Treatment includes appropriate antibiotic therapy (doxycycline, azithromycin,
ceftriaxone, etc), liberal fluid intake, analgesics, warm sitz baths, and improvement
of the client’s resistance to infection by a good diet and plenty of rest. If urethritis is
due to an STI, it is treated with appropriate antibiotic therapy. Oral Antibiotic treatment
for 1-2 weeks (Men 2 weeks recommended). Urethritis due to trichomonas infection
(called trichomoniasis) is usually treated with an antibiotic called metronidazole
(Flagyl). Tinidazole (Tindamax) is another antibiotic that can treat trichomoniasis.
The nurse reinforces the need to complete antibiotic therapy, drink plenty of fluids,
and take warm sitz baths and analgesics for pain. Urethritis may be seen in clients
with indwelling urethral catheters. To prevent or decrease urethritis, the nurse needs
to be vigilant with sterile technique, as well as to exercise gentleness when changing
catheters. It also is essential to provide frequent perineal care, especially if the
client is incontinent of faeces. In addition to washing around the anus and buttocks,
the nurse also cleans the meatus and labia of the female client. When cleaning the
anal area, wiping away from the urethra ensures that there is no contamination. If
cotton pledgets are used, the nurse wipes from the urethral meatus to the anus in a
single stroke and discards the pledget. Client teaching information about prevention
include: avoid having intercourse with multiple partners, use condoms every time
you have unsafe sex, get tested regularly, protect others if you find out you have an
STI, inform others who are also at risk of an infection.
Evolution and complications
Failure to seek treatment for gonococcal urethritis may result in a urethral stricture
in men. Medication can often treat urethritis quickly. If the infection goes untreated,
however, the effects can be lasting and quite serious. For example, the infection
may spread to other parts of the urinary tract, including the ureters, kidneys, and
bladder. These infections can be painful on their own. While they can be treated
with more intensive rounds of antibiotics, they can cause damage to the organs if
left untreated for too long. These untreated infections can also spread to the blood
and result in sepsis, which can be deadly.
In addition, the STIs that frequently cause urethritis can damage the reproductive
system. Women may develop pelvic inflammatory disease (PID), which is painful
and can result in infertility, ongoing pelvic pain, or pain during sex. Women with
untreated STIs are also at a higher risk for ectopic pregnancies, which can be lifethreatening.
Men may develop painful inflammation or infection of the prostate
gland, or the narrowing of a section of the urethra due to scarring, leading to painful
urination. Major complications of urethritis are: pyelonephritis, pre-term delivery,
urinary retention, recurrent UTI, prostatitis, sepsis, renal abscess.
Self-assessment 4.1.1
1. What are all possible causes or risk factors to develop the urethritis?
2. What are the signs and symptoms of urethritis?
3. What are the investigations that should be requested to make the diagnosis
of urethritis?
4. What are their rationales?
5. What must be included into the management plan of the urethritis?
6. If not treated, what are the complications of urethritis?
4.1.2 CYSTITIS
Learning Activity 4.1.2
Carefully read the case below and answer the following questions:
A 27-year-old woman presents to her primary care physician with a report of
urinating more frequently and pain with urination. She denies blood in her urine,
fevers, chills, flank pain, and vaginal discharge. The nurse reports the cloudy
urine with a strong bad odor, after some days of hospitalization patient complains
the fever, pain or burning sensation while urinating, cramps or pressure in lower
middle abdomen and back, the results of laboratory test show red blood cells in
urine and E.coli. The physician prescribed for her the antibiotics (ciprofloxacin
500mg two times a day during 7 days) and painkillers (ibuprofen 400mg three
times a days for 5 days and buscopan 20mg two times a day for 5 days) and
nurse continued to monitor vital signs and drugs administration.
She reports having experienced similar symptoms a few years ago and that they
went away after a course of antibiotics. The patient has no other past medical
problems. Pertinent history reveals that she has been sexually active without
using condoms.
1. What are the abnormal signs and symptom that the patient was presenting?
2. What is the medical condition was the patient having?
3. What are the possible causes and risk factors of that medical condition as
stipulated in this case?
4. What are the investigations for diagnosing that medical condition?
5. Propose the treatment plan for this patient.6. What are possible complications if the patient is not well treated?
Cystitis is an inflammation of the urinary bladder usually caused by the bladder
infection. Although it is usually able to be treated on an outpatient basis, it is
common type of UTIs that are potential source of ore complex problems requiring
invasive treatment.
Causes of cystitis
Cystitis can be either acute or interstitial:
Bacterial cystitis:
UTIs typically occur when bacteria outside the body enter the urinary tract through
the urethra and begin to multiply. Most cases of cystitis are caused by a type of
Escherichia coli (E. coli) bacteria. Bacterial bladder infections may occur in women
as a result of sexual intercourse. But even sexually inactive girls and women are
susceptible to lower urinary tract infections because the female genital area often
harbors bacteria that can cause cystitis.
Non-infectious cystitis:
Although bacterial infections are the most common cause of cystitis, a number
of noninfectious factors also may cause the bladder to become inflamed. The
causes include urologic instrumentation (e.g., cystoscopy, catheterization), faecal
contamination, prostatitis, or benign prostatic hyperplasia, indwelling catheters,
pregnancy, and sexual intercourse. Some examples include:
• Interstitial cystitis: The cause of this chronic bladder inflammation, also
called painful bladder syndrome, is unclear. Most cases are diagnosed in
women. The condition can be difficult to diagnose and treat.
• Drug-induced cystitis: Certain medications, particularly the chemotherapy
drugs cyclophosphamide and ifosfamide, can cause inflammation of your
bladder as the broken-down components of the drugs exit your body.
• Radiation cystitis: Radiation treatment of the pelvic area can cause
inflammatory changes in bladder tissue.
• Foreign-body cystitis: Long-term use of a catheter can predispose you
to bacterial infections and to tissue damage, both of which can cause
inflammation.
• Chemical cystitis: Some people may be hypersensitive to chemicals
contained in certain products, such as bubble bath, feminine hygiene sprays
or spermicidal jellies, and may develop an allergic-type reaction within the
bladder, causing inflammation.
• Cystitis associated with other conditions: Cystitis may sometimes occur
as a complication of other disorders, such as diabetes, pregnancy, kidney
stones, an enlarged prostate or spinal cord injuries.
Pathophysiology
The inflammation usually is caused by a bacterial infection. Bacteria can invade
the bladder from an infection in the kidneys, lymphatics, and urethra. Because the
urethra is short in women, ascending infections, or microorganisms from the vagina
or rectum are more common.
The lining of the bladder provides a natural resistance to most bacterial invasions
by preventing an inflammatory reaction from occurring. If bacteria do survive in the
bladder, however, they adhere to the mucosal lining of the bladder and multiply. The
surface of the bladder becomes edematous and reddened, and ulcerations may
develop. When urine contacts these irritated areas, the client experiences pain and
urgency, which is magnified in the presence of even slight bladder distention.
Signs and Symptoms
The symptoms of cystitis include urgency (feeling a pressing need to void although
the bladder is not full), frequency, low back pain, dysuria, perineal and suprapubic
pain, and hematuria, especially at the termination of the stream (terminal hematuria).
If bacteremia is present, the client also may have chills, fever, dark urine, cloudy
or strong smelling. When the disease/infection becomes severe, the patient will
experience some systemic signs and symptoms: nausea, vomiting, loss appetite,
weakness, etc. Chronic cystitis causes similar symptoms, but usually they are less
severe.
Investigations
Microscopic examination of the urine reveals an increase in the number of red
and white blood cells.
Culture and sensitivity studies are used to identify the causative microorganism
and appropriate antimicrobial therapy.
If repeated episodes occur, intravenous pyelogram (IVP) or cystoscopy with or
without retrograde pyelograms may be needed to identify the possible cause, such
as chronic prostatitis or a bladder diverticulum (weakening and outpouching of the
bladder wall), which encourages urinary stasis and infection.
Adequate medical diagnosis
The client’s history and symptoms often provide a tentative diagnosis. Culture and
sensitivity studies are used to identify the causative microorganism. Intravenous
pyelogram or cystoscopy may identify the possible cause of cystitis.
Treatment Plan
Medical management includes antimicrobial therapy and correction of contributing
factors. Examples of drugs that may be used include trimethoprim-sulfamethoxazole
(Bactrim) and nitrofurantoin macrocrystals (Macrodantin). Antibiotics like
sulfonamides are drugs commonly used to treat urinary tract infections (UTIs).
Other drugs used are nitrofurantoin macrocrystals (Macrodantin) and nitrofurantoin
(Furadantin), and the acids methenamine mandelate (Mandelamine) and nalidixic
acid (NegGram). An azo dye, phenazopyridine (Pyridium), may be ordered for its
soothing effect on bladder mucosa and often is used in conjunction with urinary
antimicrobial drugs.
Cranberry juice or vitamin C may be recommended to keep the bacteria from
adhering to the wall of the bladder and thus promoting their excretion and enhancing
the effectiveness of drug therapy.
When there is a partial urethral obstruction, no treatment of cystitis is fully effective
until adequate drainage of urine is restored by the removal of the obstruction (see
discussion of urethral strictures).
In some instances, treatment may be prolonged and may need to be repeated.
Advise clients to follow their physicians’ instructions about the medication, such as
drinking extra fluids.
Evolution and complications
When treated promptly and properly, bladder infections rarely lead to complications.
But left untreated, they can become something more serious. Complications may
include:
• Kidney infection: an untreated bladder infection can lead to kidney infection,
also called pyelonephritis. Kidney infections may permanently damage the
kidneys.
• Young children and older adults are at the greatest risk of kidney damage
from bladder infections because their symptoms are often overlooked or
mistaken for other conditions.
• Blood in the urine: with cystitis, the patient may have blood cells in the
urine that can be seen only with a microscope (microscopic hematuria) and
that usually resolves with treatment. If blood cells remain after treatment, the
doctor may recommend a specialist to determine the cause.
• Blood in the urine that the patient can see (gross hematuria) is rare with
typical, bacterial cystitis, but this sign is more common with chemotherapy- or
radiation-induced cystitis
Self-assessment 4.1.2
1. What are all possible causes or risk factors to develop the cystitis?
2. What are the signs and symptoms of cystitis?
3. What are the investigations that should be requested to make the diagnosis
of cystitis?
4. What are their rationales?
5. What must be included into the management plan of the cystitis?
6. If not treated, what are the complications of cystitis?
4.1.3 ACUTE AND CHRONIC PYELONEPHRITIS
Learning Activity 4.1.3
Carefully read the case below and answer the following questions:
S.U. a 38-yr-old woman came at the accident and emergency of Kibungo DH
for a history of painful, frequent urination with passage of small volumes of urine
for 3 days. Had intermittent fever, chills, and back pain during 3 days. She was
frightened when she saw blood in her urine and reports this is her third attack of
painful urination and back pain in 4 months. She is anxious because her father
died of kidney cancer and remembers having many UTIs as a child. She has
had four pregnancies with difficult vaginal deliveries. She complains of bilateral
flank pain and abdominal tenderness to palpation, and severe pain (pain score
of 9/10) while palpating the costovertebral area. Her vital signs are BP: 134/67
mmHg, Pulse: 78 beats/min, respiratory rate of 24 cycles/min, temperature of
38° C. The urinalysis revealed pyuria, hematuria and the presence of white blood
cells in the urine. Urine and blood cultures were still pending and treating team
decided to hospitalize her, gave her the IV fluids (Normal saline 2liters/24hours),
ciprofloxacin tablets 500mg BID for 7 days, and IV paracetamol 100mg as
needed.
1. What are the abnormal signs and symptoms the patient was presenting?
2. What are the risk factors that predispose S.U to develop her medical
condition?
3. What is the medical condition that S.U is presenting?
4. List all investigations that have been ordered to the patient, and all other
helpful investigations based on her medical condition.
5. What was included into her treatment plan?
6. What do you think could be the complications if her medical condition is
poorly managed?
The most common urologic disorders are infectious and inflammatory conditions.
Those that affect the kidneys are extremely dangerous because damage to the
nephrons can result in permanent renal dysfunction and the consequences can
lead to acute or chronic renal failure.
Pyelonephritis is an acute or chronic bacterial infection of the kidney (which
involves one or both kidneys) and the lining of the collecting system (kidney pelvis).
Acute pyelonephritis presents with moderate to severe symptoms that usually
last 1 to 2 weeks. If the treatment of acute pyelonephritis is unsuccessful and the
infection recurs, the chronic pyelonephritis occurs.
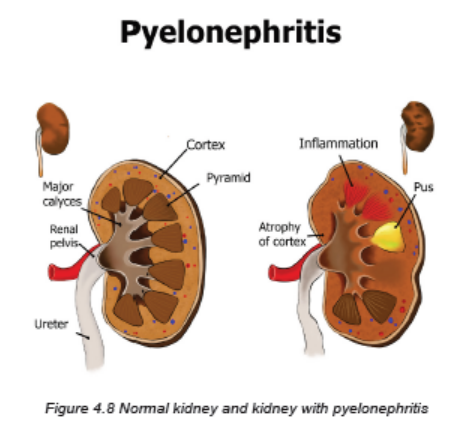
A. ACUTE PYELONEPHRITIS
In acute pyelonephritis, the inflammation causes the kidneys to grossly enlarge.
The cortex and medulla develop multiple abscesses. The renal calyces and pelves
also can become involved. Resolution of the inflammation results in fibrosis and
scarring.
Causes and Risk Factors
Pyelonephritis usually begins with colonization and infection of the lower urinary
tract via the ascending urethral route. Acute pyelonephritis commonly starts in the
renal medulla and spreads to the adjacent cortex. The common causes are:
• Bacteria normally found in the intestinal tract, such as E. coli or Proteus,
Klebsiella, or Enterobacter species, frequently cause pyelonephritis.
• A preexisting condition like vesicoureteral reflux (retrograde, or backward,
movement of urine from lower to upper urinary tract)
• Dysfunction of the lower urinary tract causing the urinary stasis or urinary
obstruction (e.g., obstruction from benign prostatic hyperplasia, tumors, a
stricture, a urinary calculi or stone).
• Instrumentation of urethra and bladder (Urinary tract catheterization,
cystoscopy, urologic surgery) is also a common cause of pyelonephritis and
urosepsis.
• Another important risk factor for acute pyelonephritis is pregnancy-induced
physiologic changes in the urinary system.
• Women with increased sexual activity, who use the diaphragm or spermicide,
who fails to void after intercourse, history of recent urinary infection.
• Men who perform anal intercourse, who has infection with HIV
• Inability to empty the bladder
• Other existing conditions/comorbidities like diabetes mellitus, other renal
disease (polycystic kidney disease), neurogenic bladder (post stroke, multiple
sclerosis, or spinal cord injury)
Pathophysiology
Infection spread by ascending microorganisms along the ureters, and may be also by
bloodstream. The infection causes the inflammation, and the inflammatory process
affects the pelvis, calyces, medulla and tubules. There is medullary infiltration of
white blood cells with renal inflammation, renal edema and purulent urine. In severe
infection, the abscess may be formed in the medulla and extend into the cortex.
The necrosis of renal papillae may develop.
Signs and Symptoms
The clinical manifestations of acute pyelonephritis are acute onset and vary from
mild fatigue to the sudden onset of chills, fever, vomiting, malaise, flank or groin pain,
and the lower UTIs characteristics that include dysuria, urgency, and frequency.
The patient might also have the cloudy or purulent urine.
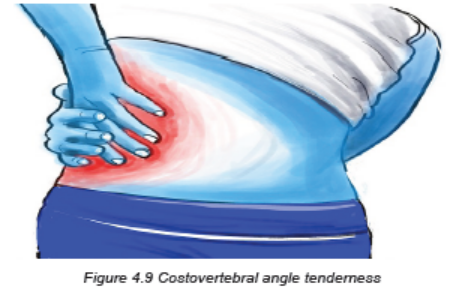
Costovertebral tenderness to percussion (costovertebral angle pain) is typically
present on the affected side. Although the clinical manifestations may subside within
a few days, even without specific therapy, bacteriuria and pyuria usually persist.
Investigations
For investigating the pyelonephritis, the complete history taking and comprehensive
physical examination must be performed first. The most useful investigations are:
• Urinalysis that will indicate pyuria, bacteriuria, and varying degrees of
hematuria. White blood cells casts may be found in the urine indicating
involvement of the renal parenchyma.
• A full blood count ( FBC) shows leucocytosis (increased levels of leukocytes
in the blood)
• Urine cultures must be obtained when pyelonephritis is suspected to detect
the causative agents.
• In patients with more severe illness who are hospitalized, blood cultures
are usually obtained as well.
• Ultrasonography of the urinary system may be performed to identify anatomic
abnormalities, hydronephrosis, renal abscesses, or an obstructing stone.
• Other Imaging investigations include CT scan alone or combined with
Intravenous pyelography, VCUG (a voiding cystourethrogram is a study
used to look at bladder and urethral abnormalities and to determine if you
have ureteral reflux), CT urograms are also used to assess for signs of
infection in the kidney and complications of pyelonephritis such as impaired
renal function, scarring, chronic pyelonephritis, or abscesses.
Adequate Medical diagnosis
The client’s history and symptoms often provide a tentative diagnosis. The physical
examination and most useful investigations such as urinalysis, a full blood count ,
urine culture may contribute to confirm the diagnosis

Treatment Plan
The treatment plan is made basing of severity of signs and symptoms that the
patient is presenting.
Mild Symptoms (Uncomplicated Infection):
• Outpatient management or short hospitalization
• Antibiotics therapy should be for 2 – 3 weeks
• Empirically selected broad-spectrum antibiotics: ampicillin, vancomycin
combined with an aminoglycoside (e.g., tobramycin, gentamicin)
• Switch to sensitivity-guided therapy: trimethoprim/sulfamethoxazole (Bactrim)
when results of urine and blood culture are available
• Fluoroquinolones are helpful too like ciprofloxacin, ofloxacin, norfloxacin,
gatifloxacin
• Adequate fluid intake (oral preferably)
• Nonsteroidal antiinflammatory drugs (NSAIDs) or antipyretic drugs
• Follow-up urine, blood cultures and imaging studies
Severe Symptoms:
• Require Hospitalization
• Antibiotics therapy should be for 2 – 3 weeks
• Parenteral (Intravenous) Antibiotics
• Oral antibiotics (broad spectrum antibiotics, fluoroquinolones, etc) when
patient tolerates oral intake
• Adequate fluid intake (parenteral initially and switch to oral fluids as nausea,
vomiting, and dehydration subside)
• NSAIDs as antipyretic or analgesic drugs to reverse fever and relieve
discomfort
• Follow-up urine, blood culture and imaging studies
Evolution and complications
After the acute phase, healing occurs with deposition of scar tissue and
atrophy of affected tubules. Acute pyelonephritis rarely causes renal failure.
The most common complications of acute pyelonephritis are:
1. Transformation to Chronic pyelonephritis
2. Papillary necrosis due to inflammatory thrombosis of the blood vessels
supplying the renal papilla.
3. Pyonephrosis (filling of the dilated calyces and pelvis by pus due to obstruction
at pelviureteric junction.
4. Perinephric abscess due to spread of the inflammation to the perinephric fat
B. CHRONIC PYELONEPHRITIS
This is a persistent or recurrent infection of the kidney, leading to scarring of the
kidney. One or both kidneys may be involved. In chronic pyelonephritis, the kidneys
become small, atrophic, and shrunken and lose function due to fibrosis (scarring).
Chronic pyelonephritis is usually the result of recurring infections involving the upper
urinary tract. However, it may also occur in the absence of an existing infection,
recent infection, or history of UTIs.
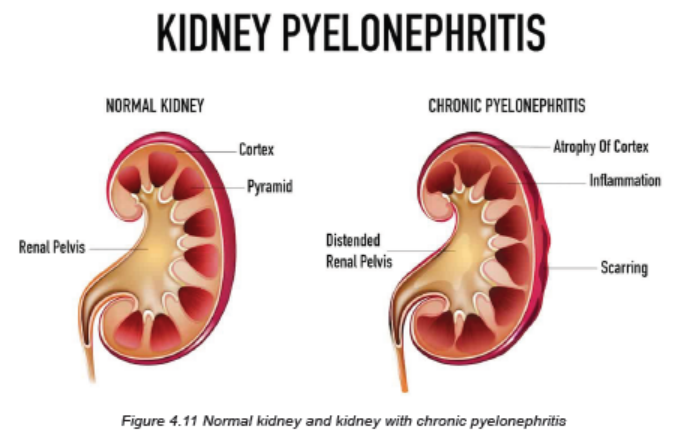
Causes and Risk factors
The most common causes of chronic pyelonephritis are:
• Recurrent episodes of acute pyelonephritis
• Chronic obstruction (e.g., strictures and stones)
• Reflux disorders that allow urine to flow backward up the ureters
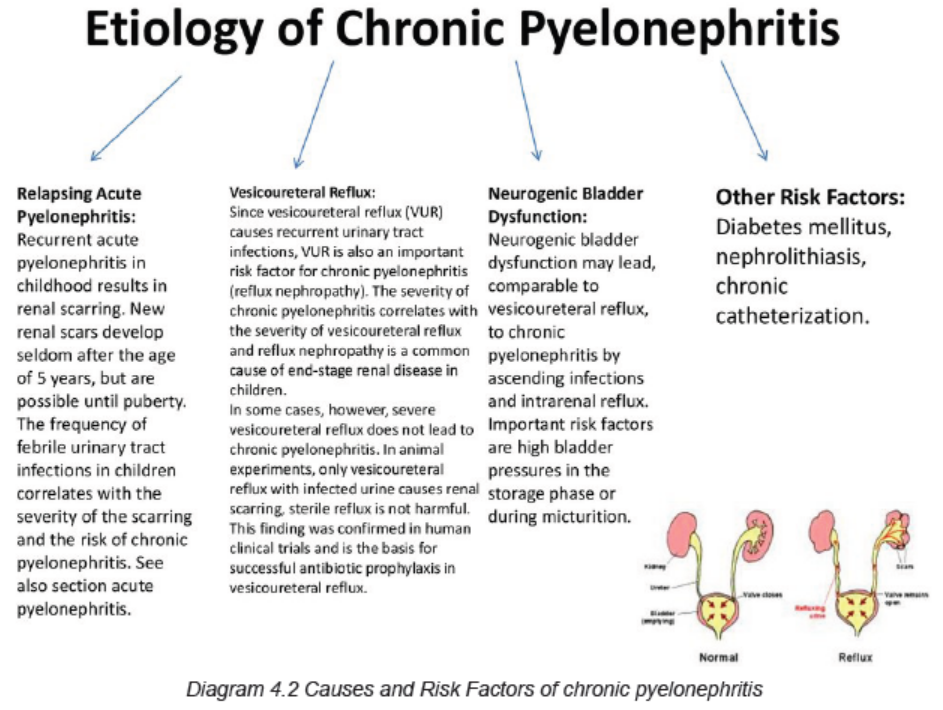
Pathophysiology
There is a process of progressive inflammation, altered renal pelvis and calyces,
destruction of the tubules, atrophy or dilation, and diffuse scarring; and finally
impaired urine- concentrating ability, leading to chronic renal failure.
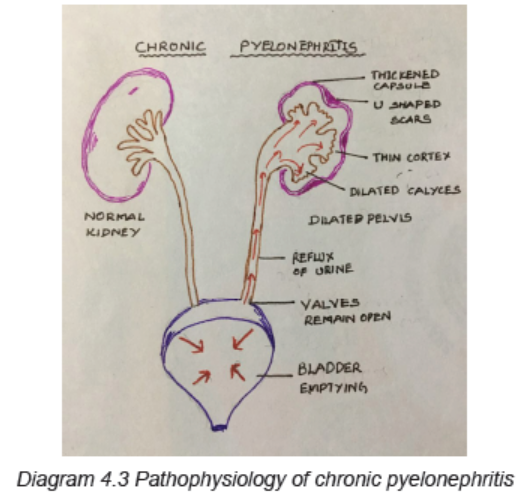
Signs and Symptoms
Repeated acute pyelonephritis leads to chronic pyelonephritis. In exacerbation,
the symptoms are similar to acute pyelonephritis. The general clinical signs and
symptoms are:
– General body weakness, fatigability, headache
– Anorexia/poor appetite
– Polyuria and frequency urine
– Excessive thirst
– Weight loss
– Pain and/or unpleasant sensation at costovertebral region
– Flank pain
– Cloudy urine
– Progressive scarring leads to Renal failure
– Systemic signs: elevated BP (Hypertension), vomiting, diarrhea.
Investigations
Investigations of chronic pyelonephritis are similar to the ones of acute pyelonephritis.
The complete history taking and comprehensive physical examination must be
performed first. Radiologic imaging and a biopsy, rather than clinical features are
used to confirm the diagnosis of chronic pyelonephritis.
The level of renal function in chronic pyelonephritis depends on whether one or
both kidneys are affected, the extent of scarring, and the presence of coexisting
infection.
The most useful investigations are:
• Urinalysis that will indicate pyuria, bacteriuria, and varying degrees of
hematuria. White blood cells casts may be found in the urine indicating
involvement of the renal parenchyma.
• A full blood count ( FBC) shows leucocytosis (increased levels of leukocytes
in the blood)
• Urine cultures must be obtained when pyelonephritis is suspected to detect
the causative agents.
• In patients with more severe illness who are hospitalized, blood cultures
are usually obtained as well.
• Ultrasonography of the urinary system may be performed to identify anatomic
abnormalities, hydronephrosis, renal abscesses, or an obstructing stone.
• Other Imaging investigations include CT scan alone or combined with
Intravenous pyelography, VCUG (a voiding cystourethrogram is a study
used to look at bladder and urethral abnormalities and to determine if you
have ureteral reflux), CT urograms are also used to assess for signs of
infection in the kidney and complications of pyelonephritis such as impaired
renal function, scarring, chronic pyelonephritis, or abscesses.
• Imaging studies reveal a small, fibrotic kidney. The collecting system may be
small or hydronephrotic.
• Renal Biopsy results indicate the loss of functioning nephrons, infiltration of
the parenchyma with inflammatory cells, and fibrosis.
Adequate medical diagnosis
The client` history and symptoms often provide a tentative diagnosis. A comprehensive
physical examination must be performed . The most useful investigations such as
urinalysis, a full blood count, urine culture and ultrasonography may contribute to
confirm the diagnosis.
Treatment plan
The treatment should focus on treating the causes (Obstruction must be relieved)
and treat all risk factors (vesicoureteral reflux, neurogenic bladder dysfunction,
arterial hypertension) and should also include the prolonged Antibiotics for 4-6
weeks.
The patient will require hospitalization, Parenteral (Intravenous) Antibiotics but Oral
antibiotics (broad spectrum antibiotics, fluoroquinolones, etc.) can be preferred
when patient tolerates oral intake. Patient must also receive the adequate fluid intake
(parenteral initially and switch to oral fluids as nausea, vomiting, and dehydration
subside) and NSAIDs as antipyretic or analgesic drugs to reverse fever and relieve
discomfort.
Surgical management (Nephrectomy) is indicated when there is unilateral
manifestation of chronic pyelonephritis with organ dysfunction to control current
UTI or arterial hypertension.
Evolution and Complications
Chronic pyelonephritis often progresses to end-stage kidney (renal) disease
(ESRD) even if the underlying infection is successfully treated.
The most common complications of chronic pyelonephritis are:
• Anemia
• Fluid overload
• Bacteremia
• Hypertension
• Renal stones
• End stage renal disease
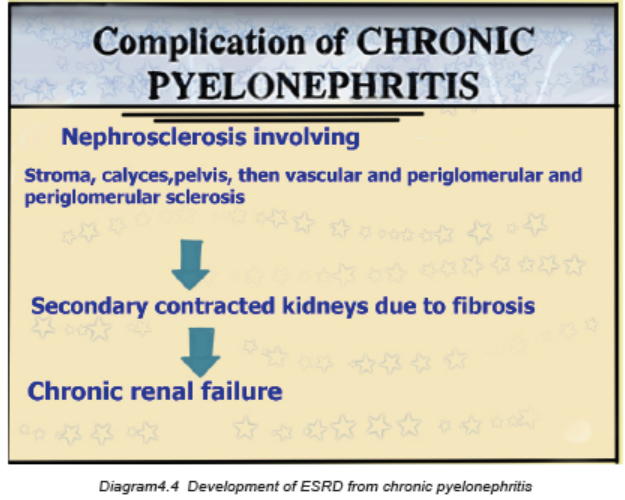
Self-assessment 4.1.3
1. What is the most common cause of acute pyelonephritis resulting from an
ascending infection from the lower urinary tract?
a) The kidney is scarred and fibrotic.
b) The organism is resistant to antibiotics.
c) There is a preexisting abnormality of the urinary tract.
d) The patient does not take all of the antibiotics for treatment of a UTI.
2. Which characteristic is more likely with acute pyelonephritis than with a
lower UTI?
a) Fever
b) Dysuria
c) Urgency
d) Frequency
3. Which test is required for a diagnosis of pyelonephritis?
a) Renal biopsy
b) Blood culture
c) Intravenous pyelogram (IVP)
d) Urine for culture and sensitivity
4. Referring to their causes, differentiate the acute and chronic pyelonephritis
5. What are the investigations and their rationale requested for pyelonephritis?
6. What are the treatment modalities are available for severe form of acute
pyelonephritis?
7. What are the most clinical signs and symptoms that determine the
pyelonephritis?
8. What are the treatment options for chronic pyelonephritis?
9. Referring to RAA system, describe how the pyelonephritis can cause the
hypertension
10. What are the complications of chronic pyelonephritis?
11. Describe how the pyelonephritis can lead to renal failure.
4.1.4 ACUTE AND CHRONIC PROSTATITIS
Learning Activity 4.1.4
Carefully read the case below and answer the following questions:
A 54-year-old man experiences a brief period of dysuria accompanied by some
frequency and urgency. These symptoms occurred after a couple of days where
he didn’t seek medical treatment. Three days later, he suddenly developed fever
(39oC), chills, and worsening, irritating dysuria. Because the fever persisted, he
went to see his physician. Except for the fever, his vital signs were normal. Upon
physical examination, he is found to have extreme tenderness in his prostate
by digital rectal examination. The prostate is palpably tense. He does not have
any noticeable costovertebral angle tenderness and no other notable physical
abnormalities. He says that he has not had any previous incidents that producedsymptoms like the ones he has been experiencing over the past few days.
He was advised to drink plenty of much water, prescribed ciprofloxacine 500mg
BID for 7 days, paracetamol 500mg TDS for 5 days, requested the abdominal
ultrasound and the urine culture that results were still pending.
1. What are abnormal signs and symptoms was the patient having?
2. What is the medical diagnosis is the patient presenting?
3. What are different risk factors to the development of that medical condition?
4. What are all relevant investigations are helpful in confirming that diagnosis?
5. What is the treatment plan of that medical condition?
6. What might be the complications if poorly treated?
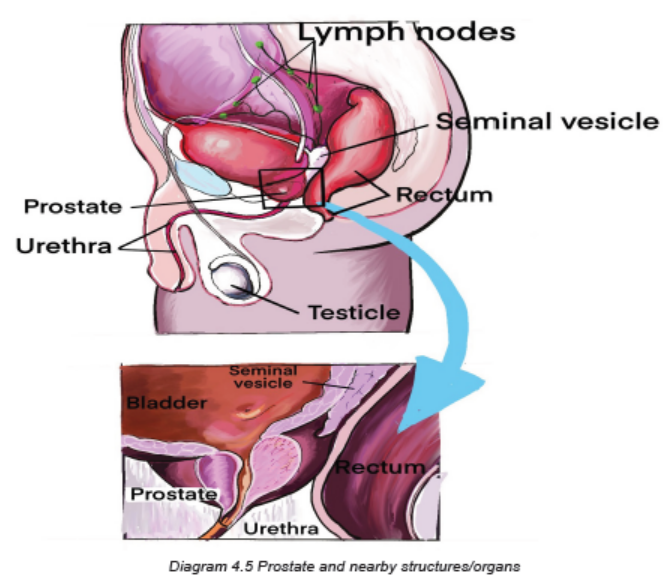
The term prostatitis has been used for various inflammatory conditions affecting
the prostate, including acute and chronic infections with specific bacteria and, more
commonly, instances in which signs and symptoms of prostatic inflammation are
present but no specific organisms can be detected.
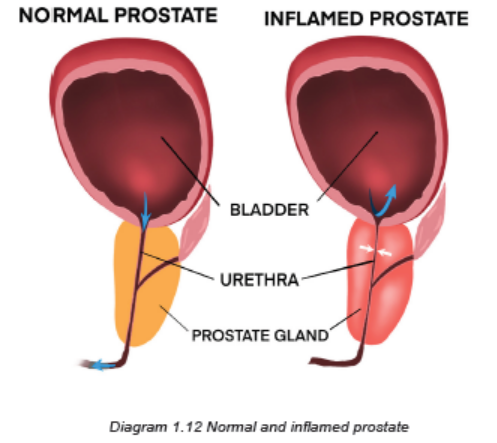
Classification of prostatitis
Prostatitis is classified as:
– Acute bacterial prostatitis
– Chronic bacterial prostatitis
– Nonbacterial prostatitis (Chronic pelvic pain syndrome).
A. ACUTE PROSTATITIS
Acute prostatitis is a sudden inflammation of the prostate gland. It is a rare type of
prostatitis, which is a common prostate problem. When the prostate gland becomes
inflamed, symptoms may be similar to those of an acute UTI. Acute prostatitis
is often caused by a type of bacteria that causes UTIs and sexually transmitted
infections.
Causes and Risk factors
Inflammation can result from bacteria entering the prostate via the blood or an
infection in the area. It can also be caused by urethral stricture and prostatic
hyperplasia. A medical procedure may also lead to bacteria entering the prostate.
Underlying causes of acute prostatitis might also be a blocked urethra or suppressed
immune system. The most common causes of prostatitis are bacteria, fungi or
mycoplasma:
– Escherichia coli
– Enterobacter
– Klebsiella
– Pseudomonas
– Chlamydia trachomatis
The risk factors for acute bacterial prostatitis (all allow bacterial colonization) are
intra-prostatic ductal reflux, phimosis and redundant foreskin, unprotected anal
intercourse, urinary tract infections, acute epididymitis, indwelling foley catheter,
transurethral surgery, altered prostatic secretions, recent transrectal ultrasoundguided
prostate needle biopsy, immunosuppression (patients with underlying
immunosuppression, may be more likely to have prostatic involvement with
organisms other than the usual bacteria that tend to cause urinary tract infection),
etc.
Pathophysiology
The infection stimulates an inflammatory response in which the prostate becomes
enlarged, tender, firm, or boggy (too wet). Acute inflammatory prostatic edema may
cause urinary obstruction with dysuria. The onset of the illness may be acute, or
follow catheterization or cystoscopy.
An inflammation of the prostate gland and surrounding tissue due to an infection
can be acute or chronic. Some physiological factors that contribute to development
of prostatitis are altered prostate secretory functions, decreased zinc, decreased
prostatic antibacterial factor and altered prostatic PH. The prostatitis can also be
due to catheters, urethral instrumentation and transurethral prostatectomy.
Signs and symptoms
Patient with acute prostatitis present with low back pain, perineal pain, high fever
up to 40o C, chills, dysuria, inability to empty the bladder, nocturia, urinary retention,
systemic signs and symptoms of infection (myalgia, arthralgia, fatigue/malaise),
prostatic pain especially when an individual is in upright position, symptoms can
include pain (in the perineum, lower abdomen, testicles, penis, and with ejaculation),
bladder irritation, bladder outlet obstruction, and sometimes blood in the semen,
sexual dysfunction may accompany chronic bacterial prostatitis.
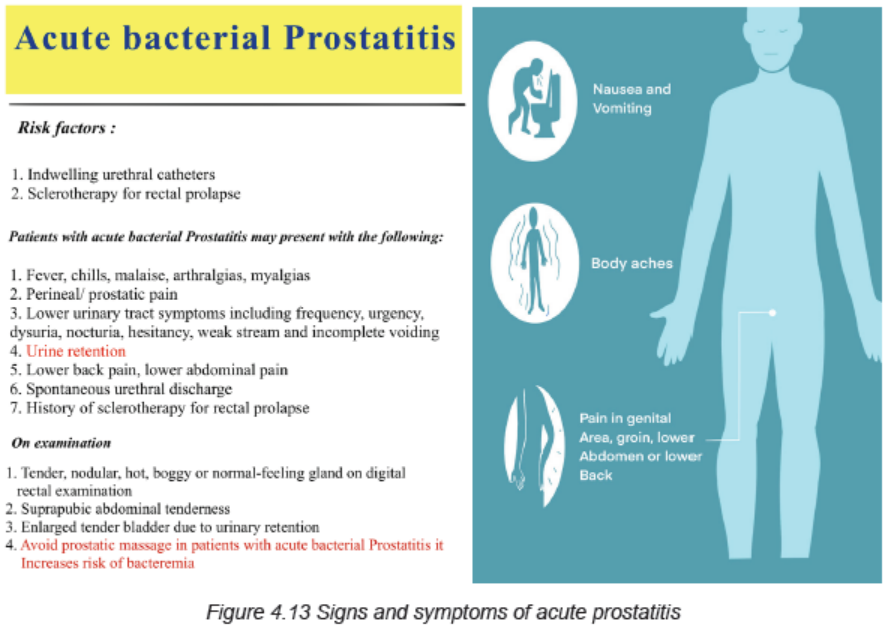
Investigations
The ways of diagnosing the acute prostatitis include:
• Complete history taking
• Complete physical exam that include the Digital rectal examination: there
may be prostatic hypertrophy, tenderness, edema, and nodularity. However,
the prostate exam is frequently normal.
• FBC, Urea and creatinine, PSA (prostatic specific antigen): Laboratory
findings that suggest inflammation or infection like elevated serum
leukocytes or inflammatory markers may be absent. Usually there is an
elevated prostatic specific antigen (>4 ng/mL).
• Urinalysis: Gram stain, culture, bacteriuria (WBC >105 )
• The diagnostic standard for bacterial prostatitis is the finding of bacteria at
higher levels in prostatic fluid compared with urethral and bladder specimens.
It is better to obtaining prostatic specimens for analysis and culture to
confirm the prostate as the site of infection.
• Abdominal ultrasound can also be helpful (demonstrated the prostate
increased in size).
Adequate medical diagnosis
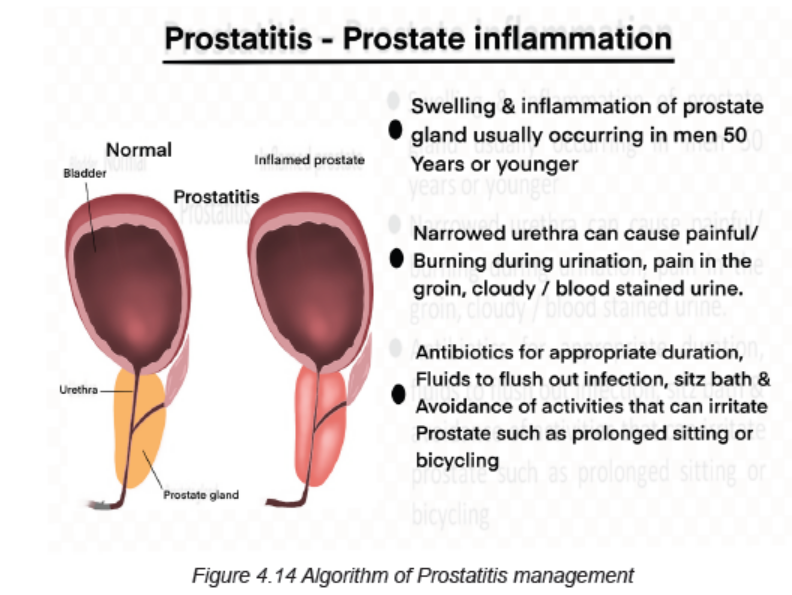
Treatment plan
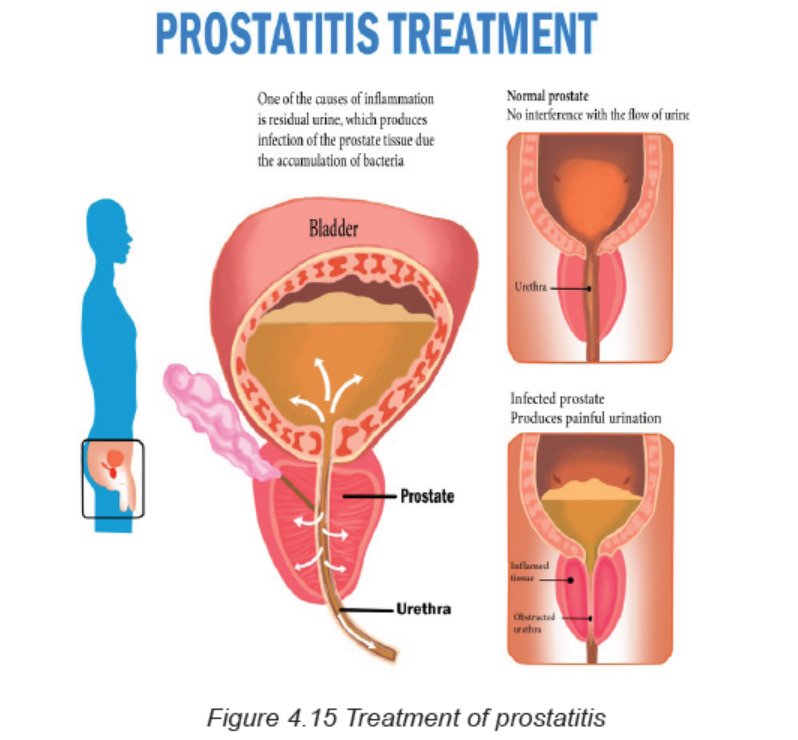
The treatment plan for acute prostatitis includes:
Antibiotics: prolonged antibiotic therapy (for at least six weeks) with an agent that
has good penetration into the prostatic tissue is generally necessary for treatment
of bacterial prostatitis. A fluoroquinolone is generally the drug of choice for both
initial and recurrent episodes. Trimethoprim-sulfamethoxazole is an adequate
alternative regimen. Other agents with good penetration into prostatic fluid and
tissue include tetracyclines and macrolides. In mild case: Oral antibiotics up to 6
weeks, in severe cases: IV Ampicilline+ Gentamycine for 7 days, then 4-6 weeks
oral antibiotics.
Analgesics and Antipyretics
Bed rest and adequate hydration
Addressing urinary obstruction — Symptoms of difficulty urination, a sensation of
incomplete emptying, or post-void dribbling should trigger further investigations.
Alpha-blockers (prazocin, terazocin, etc) may be used to relax the bladder muscles
and reduce discomfort
Most cases of acute prostatitis will clear up with antibiotic treatment. Some
severe cases of infection may require a hospitalisation, and mainly due to failed
outpatients management, inability to tolerate oral intake, evidence of resistance risk
factors (recent fluoroquinolones use, recent transurethral or transrectal prostatic
manipulation), systemically ill patient or septicaemia, urinary retention, etc
In addition to medical interventions, a patient may try to alleviate symptoms with
home remedies like taking warm showers or baths, avoiding activities that put
pressure on the prostate such as bicycling, sitting on a cushion, avoiding alcohol,
reducing or avoiding consumption of spicy foods, drinking plenty of fluids that do
not contain caffeine. There are a variety of lifestyle changes that may reduce the
risks of developing chronic or recurring prostatitis: reducing stress, using protection
during sexual activity, ejaculating at least once a week, avoiding processed foods,
eating a healthful diet, protecting against pelvic trauma, maintaining a healthy
weight.
Evolution and Complications
Most cases of acute prostatitis will clear up with antibiotic treatment. Acute prostatitis
may cause a blockage of the urethra. When this occurs, a person will experience
pain and discomfort in the bladder. If left untreated, a blocked bladder can lead
to permanent kidney damage. Other complications may include residual chronic
prostatitis, inflammation of the epididymis or epididymoorchitis (a coiled tube at
the back of the testicles), bacteremia (a bacterial infection of the blood), prostatic
abscess (a pus-filled pocket in the prostate), semen abnormalities, seminal
vesiculitis, infertility.
B. CHRONIC BACTERIAL PROSTATITIS
The chronic bacterial Prostatitis is characterized by recurrent urinary tract symptoms
and persistence of pathologic bacteria (usually Gram negative) in urine or prostatic
fluid. It is similar to chronic pelvic pain syndrome (CPPS). Chronic prostatitis is the
inflammation or infection of the prostate that lasts at least 3 months.
Causes and risk factors
Chronic bacterial prostatitis is caused by bacteria getting to the prostate through the
urethra. This infection can be caused by an infection originating from the bladder or
contaminated urinary catheter. Some bacterial infections contribute to the formation
of prostate stones that are not expelled during urination. Prostate stones are about
the size of a poppy seed and are not always detectable during physical exam.
Infected prostate stones are a common cause of recurring UTIs and make curing
chronic bacterial prostatitis very difficult.
Pathophysiology
The infection stimulates an inflammatory response in which the prostate becomes
enlarged, tender, firm, or boggy (too wet). Acute inflammatory prostatic edema may
cause urinary obstruction with dysuria.
Signs and symptoms
The signs and symptoms of chronic prostatitis and CPPS are very similar. They
usually start out mild and build in intensity over time. Those signs and symptoms
include: a constant urge to urinate, burning pain when urinating, difficulty starting
urination followed by uneven flow, blood in urine, feeling as if the bladder isn’t fully
emptied after urination, painful ejaculation, pain in following locations: lower back,
lower abdomen, above pubic area, between the testicles and anus, etc. It may also
be accompanied by fever and chills.
Symptoms may be similar to those of prostatic cancer, urinary retention, bladder
stones and those from an acute bladder infection: urgency, frequency, dysuria,
perineal discomfort, low back pain, myalgia, arthralgia and sexual dysfunction.
The prostate may only slightly enlarged or wet, but yet fibrosis because with
repeated infections can cause it to be rigid and irregular in shape.
Investigations
– Complete history taking
– Complete physical exam that include the Digital rectal examination: there
may be prostatic hypertrophy, tenderness, edema, and nodularity. However,
the prostate exam is frequently normal.
– FBC, Urea and creatinine, PSA (prostatic specific antigen): Laboratory
findings that suggest inflammation or infection like elevated serum leukocytes
or inflammatory markers may be absent. Usually there is an elevated prostatic
specific antigen (>4 ng/mL).
– Urinalysis: Gram stain, culture, bacteriuria (WBC >105 )
– The diagnostic standard for bacterial prostatitis is the finding of bacteria at
higher levels in prostatic fluid compared with urethral and bladder specimens.
It is better to obtaining prostatic specimens for analysis and culture to confirm
the prostate as the site of infection.
– Abdominal/pelvic imaging (CT scan, MRI, ultrasound)
– Prostatic massage to express secretions: culture, Gram-stain
– Pelvic X-ray may show prostatic calculi
– Biopsy guided by transurethral or transrectal ultrasonography
Adequate medical diagnosis
Chronic prostatitis is a pelvic condition that needs to be distinguished from other
forms of prostatitis, such as acute and chronic bacterial prostatitis. It is characterized
by pelvic or perineal pain lasting longer than 3 months without evidence of urinary
tract infection. Symptoms include pain that may radiate to the back and perineum
causing discomfort while sitting, dysuria, frequency, urgency, arthralgia, myalgia,
unexplained fatigue, abdominal pain, and burning sensation in the penis may be
present. Post-ejaculatory pain mediated by nerves and muscles is a hallmark of
the condition. Some patients report low libido, sexual dysfunction, and erectile
difficulties. The symptoms of chronic prostatitis appear to result from interplay
between psychological factors and dysfunction in the immune, neurological,
and endocrine systems. The prognosis is good with use of multimodal treatment
including antibiotics use, psychotherapy, pelvic nerve trigger point release, anxiety
control, and chronic pain therapy
Treatment plan
Antibiotics: prolonged antibiotic therapy (for 12 weeks) with an agent that has good
penetration into the prostatic tissue is generally necessary for treatment of bacterial
prostatitis. A fluoroquinolone is generally the drug of choice for both initial and
recurrent episodes. Trimethoprim-sulfamethoxazole is an adequate alternative
regimen. Other agents with good penetration into prostatic fluid and tissue include
tetracyclines and macrolides. In mild case: Oral antibiotics, In severe cases: IV
antibiotics.
Analgesics and Antipyretics (Nonsteroidal anti-inflammatory drugs or corticosteroids)
Bed rest, adequate hydration.
Addressing urinary obstruction — Symptoms of difficulty urination, a sensation of
incomplete emptying, or post-void dribbling should trigger further investigations.
Alpha-blockers may be used to relax the bladder muscles and reduce discomfort
Patients may require the hospitalisation
Treat the underlying cause (e.g.: surgical removal of prostatic stone through
transurethral prostatectomy, surgery to remove scar tissue in the urethra, which
can help urination difficulties)
Muscle relaxants to relieve spasm of the pelvic muscles
Therapy to help with psychological stress and anxiety
Evolution and complications
The prongosis is good with use of multimodal treatment including antibiotics use,
psychotherapy, pelvic nerve trigger point release, anxiety control, and chronic pain
therapy. When chronic prostatitis is caused by a bacterial infection, it can be treated
with antibiotics. When the cause is unknown, treatment of the symptoms may be
the best course of action. If left untreated, a blocked bladder can lead to permanent
kidney damage, inflammation of the epididymis or epididymoorchitis, bacteremia,
prostatic abscess, semen abnormalities, seminal vesiculitis, infertility.
Self-assessment 4.1.4
1. Differentiate the acute and chronic prostatitis
2. Describe briefly the pathogenesis of bacterial prostatitis.
3. What are the signs and symptoms of acute prostatitis?
4. What are the causes of prostatitis?
5. List the risk factors of acute prostatitis
6. Enumerate all investigations needed to diagnose prostatitis and their
rationale.
7. What are the treatment modalities of acute prostatitis?
8. Explain when is surgical interventions needed during the management of
chronic prostatitis.
9. List some complications of acute prostatitis.
10. What is the standard investigation of prostatitis?
11. What are the indications of hospitalisation to a patient with acute prostatitis?
4.2. SEXUAL TRANSMISSIBLE DISEASES (STDs)
Introductory activity 4.2
Observe the picture below and answer the questions that follow.

Figure 4.2.1Relationship between girl and boy
1. What do you see on the picture?
2. What do you think could be the consequences of their act?
Sexually transmitted infections (STIs), also known as Sexually Transmitted Diseases
(STDs), are caused by bacteria, viruses or parasites that are transmitted through
unprotected sex (vaginal, anal, or oral) and skin to skin genital contact. The most
common bacterial infections include chlamydia, gonorrhoea, and syphilis. The viral
infections include genital herpes, Hepatitis B, Human Papillomavirus (HPV) and
Human Immunodeficiency Virus (HIV). Parasites are responsible for trichomoniasis.
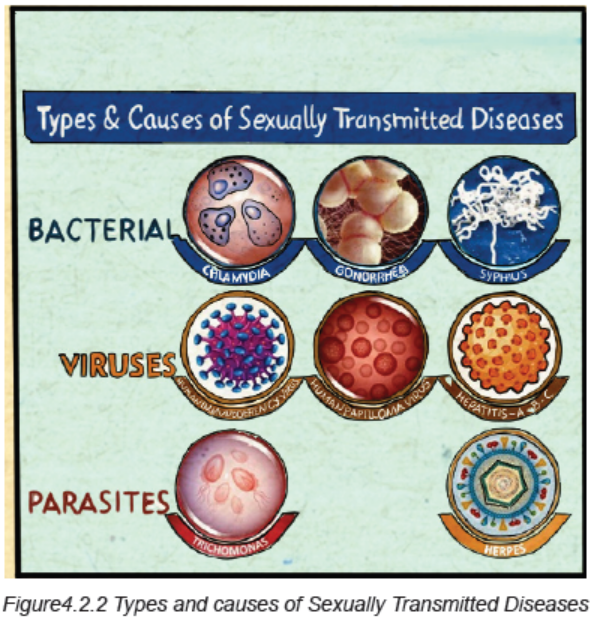
4.2.1 CHLAMYDIA
Learning Activity 4.2.1
Ms A.E, a 20 year old female was worried because she had vaginal discharge
and irritation for three days. The discharge was slight, clear, watery, and nonoffensive,
and she had no abnormal vaginal bleeding. Ms A.E had changed
her sexual partner two months previously. Soon after this she had contracted
genital thrush, which responded to topical clotrimazole. She uses a combined
contraceptive pill and does not use condoms. Ms A.E has no other sexual
partners, and thinks it unlikely her partner has. During the physical examination,
the abnormal finding at vaginal examination was that Ms A.E’s cervix bled
easily when swabbed. A vaginal swab was taken for laboratory examination.
Ms A.E was prescribed doxycycline 200 mg two times a day for seven days and
metronidazole 400 mg three times daily for seven days and sent back home and
waited for results.
A few days later the laboratory reported that chlamydia had been detected. Ms
A.E was called to come back at health facility to be communicated the results.
She was upset to be told that she might have had a sexually transmitted disease
and was unpleasant to go together with her partner.
1. What were the abnormal signs and symptoms was the patient presenting?
2. Basing on those signs and symptoms, what do you think was the medical
diagnosis?
3. What were the risk factors that predisposed her to develop that condition?
4. What were the investigations requested to guide in the confirmation of that
diagnosis?
5. What were the treatment options were available towards that diagnosis?
6. If not well managed, what will be the complications?
Chlamydia is a sexually transmitted disease caused by a bacterium named
Chlamydia trachomatis.
Risk factors
A person is at risk of getting infected of STIs if he/she drinks alcohol (it may be difficult
to convince a drunken partner to use a condom or use one condom correctly). If the
partner uses drugs, it may also make it easier for them to pressure a person into
engaging in unsafe sexual behaviours. Having one STI frequently is a risk to getting
more infections. If the skin is swollen, or scorched, it is easy for another pathogen
to cause infection.
Pathophysiology
Disease pathogenesis due to Chlamydia trachomatis is a complicated process that
involves: (1) exposure to the organism and infectivity; (2) survival within the host
cell; (3) virulence associated with specific strain types; (4) innate and acquired
immunity, and (5) host genetic susceptibility to infection and disease.
Most female and male infections are asymptomatic, which provides an ongoing
opportunity for silent transmission and the development of disease. In addition,
repeat and persistent infections are common among at risk adolescent and young
adult populations. Even with appropriate detection, there is increasing evidence
for antibiotic resistance to the common drugs used to treat Chlamydia trachomatis.
Consequently, the inability to adequately prevent, diagnose, treat, and eradicate
infection provides the opportunity for pathogenicity and disease.
Chlamydia are intracellular bacterial pathogens, which means they are unable to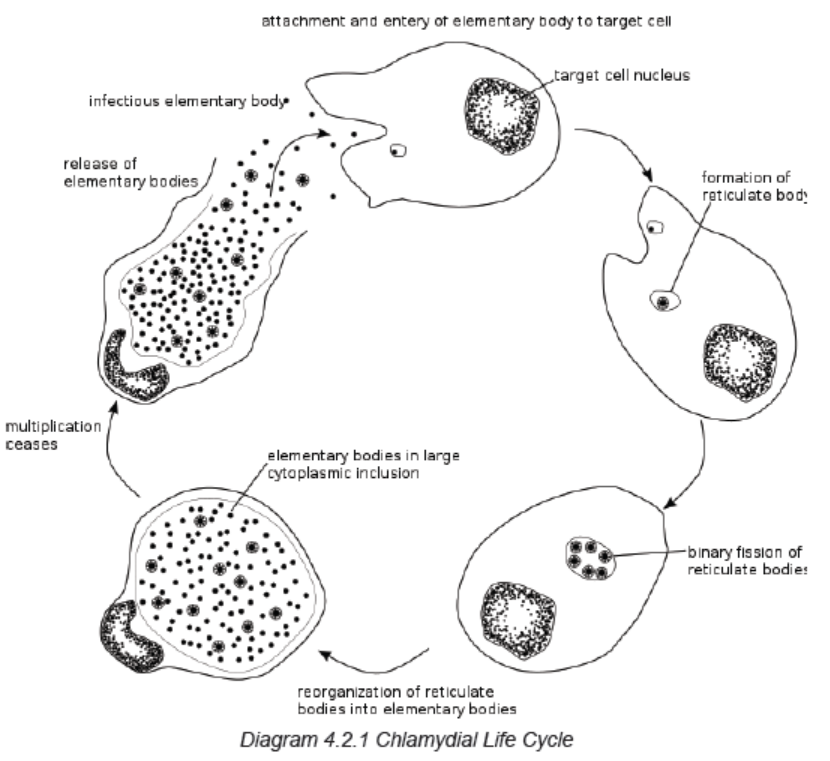
replicate outside of a host cell. However, to disseminate effectively, these pathogens
have evolved a distinct biphasic life cycle wherein they alternate between twofunctionally and morphologically distinct forms.
The elementary body (EB) is infectious, but metabolically inert (much like a spore),
and can survive for limited amounts of time in the extracellular milieu. Once the
EB attaches to a susceptible host cell, it mediates its own internalization through
pathogen-specified mechanisms (via type III secretion system) that allow for therecruitment of actin with subsequent engulfment of the bacterium.
The internalized EB, within a membrane-bound compartment, immediately
begins differentiation into the reticulate body (RB). RBs are metabolically active
but non-infectious; in many regards, they resemble normal replicating bacteria.
The intracellular bacteria rapidly modify its membrane-bound compartment into
the so-called chlamydial inclusion so as to prevent phagosome-lysosome fusion.
The inclusion is thought to have no interactions with the endocytic pathway
and apparently inserts itself into the exocytic pathway as it retains the ability tointercept sphingomyelin-containing vesicles.
The mechanism by which the host cell protein is trafficked to the inclusion through
the exocytic pathway is not fully understood. As the RBs replicate, the inclusion
grows as well to accommodate the increasing numbers of organisms. Through
unknown mechanisms, RBs begin a differentiation program back to the infectious
EBs, which are released from the host cell to initiate a new round of infection.
Because of their obligate intracellular nature, Chlamydiae have no tractable genetic
system, unlike E. coli, which makes Chlamydiae and related organisms difficult to
investigate.
Signs and symptoms
Chlamydia is the most common curable bacterial STD. The symptoms may not be
noticed, or they may be vague and nonspecific. Some people experience no health
effects at all. Chlamydia Symptoms are burning or itching of the genitals, discharge
from the penis or vagina, and pain during sex or urination. Those symptoms can
appear within days or weeks. It infects the cervix in women which is the opening to
the uterus or womb and the penile urethra in men. Chlamydia infections can also
develop in the rectum and throat.
Investigations
Screening and diagnosis of chlamydia is relatively simple. Tests include:
A urine tests: a sample of the urine is analyzed in the laboratory for presence of
this infection.
A swab: for women, your doctor takes a swab of the discharge from your cervix
for culture or antigen testing for chlamydia. This can be done during a routine Pap
test/smear. Some women prefer to swab their vaginas themselves, which has been
shown to be as diagnostic as doctor-obtained swabs. For men, the doctor inserts a
slim swab into the end of the penis to get a sample from the urethra. In some cases,
the doctor will swab the anus
Adequate medical diagnosis
In females, Chlamydia trachomatis most commonly affects the cervix. The majority
of infected females are asymptomatic, although some may present with the typical
findings of cervicitis, including vaginal discharge, abnormal vaginal bleeding, and
purulent endocervical discharge on exam.
The most concerning complication of untreated cervical chlamydial infection is
pelvic inflammatory disease, which in turn can lead to infertility, ectopic pregnancy,
or chronic pelvic pain.
In males, C. trachomatis is a common cause of nongonococcal urethritis. The
majority of infected males are asymptomatic. When present, symptoms include
a mucoid or watery urethral discharge and dysuria. C. trachomatis is a frequent
cause of acute epididymitis in males younger than 35 years of age and may be an
etiology in some cases of chronic prostatitis.
The diagnostic test of choice for chlamydial infection of the genitourinary tract is
nucleic acid amplification testing (NAAT) of vaginal swabs for females or urine for
males. NAAT should also be used on rectal swabs to diagnose chlamydial infection.
If non-NAAT-based testing is used for diagnosis or if adequate follow-up cannot be
insured, patients with signs and symptoms consistent with chlamydia should be
treated empirically before diagnostic test results return.
Treatment plan
Chlamydia can be easily cured with antibiotics. HIV-positive persons with chlamydia
should receive the same treatment as those who are HIV-negative.
Persons with chlamydia should abstain from sexual activity for 7 days after single
dose antibiotics (metronidazole, doxycycline, etc) or until completion of a 7-day
course of antibiotics, to prevent spreading the infection to partners. It is important
to take all the medications prescribed to cure chlamydia. Chlamydial infection in
infants can be treated with antibiotics.
Preventive strategies
It is important to practice proper self-hygiene, for instance, shower regularly, clean
the toilet and bathroom with disinfectants, detergent, and clean water, because one
can easily get an infection from a dirty toilet.
To ensure protection during sexual intercourse, when the client thinks he/she is at
risk of STIs, he/she should go for instant check-up and seek treatment when the
infection is suspected. However, both partners should be treated.
Also, it is urgent to see a doctor immediately if the person is sexually active and may
have been exposed to an STI, or when signs and symptoms of an STI are present.
Evolution and complications
If left untreated, chlamydia can cause permanent damage to the reproductive system
in both males and females. It can cause infertility by blocking the reproductive tract
in men and women. Chlamydia can do a lot of damage to the body in the long run.
Repeated infection with chlamydia is common. Women whose sex partners have
not been appropriately treated are at high risk for re-infection. Having multiple
chlamydial infections increases a woman’s risk of serious reproductive health
complications, including pelvic inflammatory disease and ectopic pregnancy.
Women and men with chlamydia should be retested about three months after
treatment of an initial infection, regardless of whether they believe that their sex
partners were successfully treated. In addition, the infants infected with chlamydia
may develop ophthalmia neonatorum (conjunctivitis) and/or pneumonia.
Self-assessment 4.2.1
1. Name the bacteria that is responsible of chlamydia.
2. What are the signs and symptoms of chlamydia?
3. What are the necessary tests performed to diagnose the infection of
chlamydia?
4. Explain the treatment plan of chlamydia
5. What are the preventive measures?
6. What are the complications of chlamydia in women and men?
4.2.2 SYPHILIS
Learning Activity 4.2.2
Carefully read the case below and answer the following questions:
A 39-year-old woman presented to the emergency department reporting several
weeks of generalized weakness, headache, nausea, and arthralgia. The patient
had unprotected sexual intercourse with a man whom the past 6 months physical
examination revealed a painful ulcerated plaque on the upper lip, a macular rash
with painless lesions (considered to be healing chancres) on the glans, a nonpruritic
hyperkeratotic palmar rash and bilateral submandibular lymphadenopathy.
Results of laboratory testing included a positive reactive syphilis immunoglobulin
G (IgG) enzyme immunoassay and a positive rapid plasma reagin (RPR) test.
The human immunodeficiency virus (HIV) testing was negative, and serologic
testing demonstrated prior immunization to hepatitis B virus. Given the clinical
presentation and laboratory findings, she was treated with benzathine penicillin
G 2.4 million units intramuscularly.
1. Basing on the scenario above, what are the signs and symptoms the
patient was presenting.
2. What is the medical diagnosis is the patient presenting?
3. What are different risk factors and causes of that medical condition?
4. What are different investigations used to diagnose that medical condition?
5. What are different treatment modalities for that medical condition?
6. If not properly treated, what might be some complications?
Syphilis is a chronic bacterial disease that is contracted mainly by infection during
sexual intercourse, but also congenitally by infection of a developing foetus.
Causes and Risk Factors
Syphilis is mainly caused by the bacteria called Treponema pallidum. It is a common
and dangerous infection that is spread from person to person through sexual contact.
It is an infection that is transmitted by direct contact with a syphilitic sore via skin
and mucous membranes such as the vagina, anus, rectum, lips and mouth, most
commonly during oral, anal or vaginal sexual activity. In rare occasions syphilis
spread during kissing.
Treponema pallidum also crosses the placenta, thereby resulting in fetal infection
(Congenital syphilis). This congenital syphilis is generally acquired through
transplacental transmission of spirochetes in the maternal bloodstream or,
occasionally, through direct contact with an infectious lesion during birth
The acquisition of syphilis through transfused blood is very rare because all donors
are screened and T. pallidum cannot survive longer than 24 to 48 hours under blood
bank storage conditions.
While syphilis can affect anyone, there are a number of risk factors (related to
sexual behaviors, while others are associated with characteristics that can place an
entire population at risk) that can increase your likelihood of infection: inconsistent
condom use is the main cause of transmission in all groups, and Men who have sex
with men (due to physiological vulnerabilities such as the fragility of rectal tissues),
multiple sex partners place you at risk simply by providing you a greater opportunity
for exposure, injecting drug use that can impair judgment and increase the risk of
sexual violence or the exchange of sex for drugs, risk attitude and behaviors of
avoidance of STIs screening mainly among those people who have multiple sex
partners.
Pathophysiology
The pathogenesis of Syphilis is explained through different following stages:
• Early local infection: T. pallidum initiates infection when it gains access to
subcutaneous tissues via microscopic abrasions. The spirochete evades
early host immune responses and establishes the initial ulcerative lesion, the
chancre. During the period of early local replication, some organisms establish
infection in regional draining lymph nodes, with subsequent dissemination.
Early syphilis comprises primary and secondary syphilis, which typically occur
within weeks to months after initial infection, as well as early latent syphilis
(asymptomatic infection that was acquired within the previous 12 months).
• Late infection: The prolonged latent period that is characteristic of most
types of late syphilis suggests that immune mechanisms may be involved in
one of two ways. Waning immunity with aging may facilitate recrudescence
of a small number of treponemes that had survived in sequestered sites.
Alternatively, a partially immune hypersensitive host may react to the
presence of treponemes, engendering a chronic inflammatory response. Late
benign syphilis often involving the skin, viscera, or other tissues (eg, bone,
brain, abdominal viscera), are characterized pathologically by the presence
of granulomas, a finding that is consistent with a cellular hypersensitivity
reaction.
If left untreated, syphilis will go through five stages of infection: primary, secondary,
early latent, late latent, and tertiary. The risk and mode of transmission can vary by
the stage:
• During primary syphilis, the disease is passed by coming into contact with
a chancre.
• During secondary syphilis, the disease can be passed by coming into
contact with the secondary rash.
• During early latent syphilis, secondary symptoms can sometimes relapse
and increase the risk of transmission.
• During late latent or tertiary syphilis, the disease is considered noncontagious.
Syphilis cannot be passed via toilet seats, casual contact, or the shared use of
utensils or personal care items. This is because T. pallidum has a fragile shell that
lacks the lipoproteins needed to sustain life outside of the body for very long.
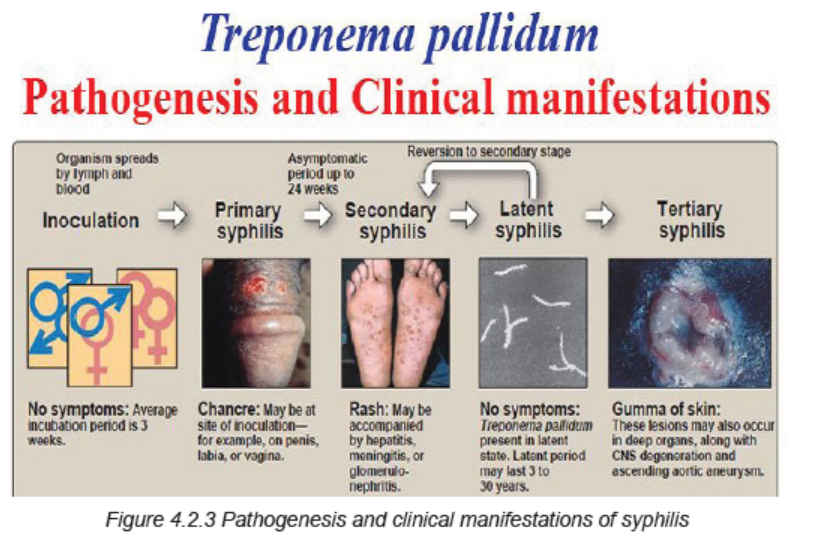
Signs and Symptoms
Patients with syphilis can present with a wide range of symptoms depending on
the stage of disease. Others will have serologic evidence of syphilis based upon
laboratory testing, but will not have symptoms (mainly in latent syphilis).
The clinical manifestations depend upon the stage of disease. The signs and
symptoms of syphilis are related to the stage of the infection. The first involves a
painless sore on the genitals, rectum, or mouth. After that heals, the second stage
will begin and usually produce a rash. After a long period with no symptoms (stage
three), the fourth stage can suddenly develop, causing extensive damage to the
brain, nerves, eyes, or heart.
Primary syphilis (Stage 1): is the first stage of infection. It will typically start with
the appearance of an ulcer called a chancre between 10 to 90 days after the initial
exposure; the average is 21 days. The sore will develop at the point of contact,
most commonly on the cervix, vagina, penis, anus, rectum, or mouth. There may
be one or more lesions. Because the sores are painless, they can be missed if they
are located internally.
Sometimes swollen lymph nodes can develop near the site of the infection. These
are small glands that, among other things, contain white blood cells that help fight
infection called lymphocytes. Without treatment, a chancre will heal in three to six
weeks.
Secondary Syphilis (Stage 2): If left untreated, a primary infection will progress
to secondary syphilis. Symptoms typically appear within two to eight weeks of the
appearance of the chancre. During this stage, a person may experience general
symptoms of illness such as fever, sore throat, fatigue, weight loss, headache,
muscle ache. They may also experience symptoms that may be a bit more telling:
unexplained hair loss (syphilitic alopecia), cracked lesions on the corner of the
mouth (fissure cheilitis), generalized swelling of the lymph nodes, widespread, nonitchy
rash on the palms and soles of the feet, the trunk, or the limbs.
Rarely, secondary syphilis affects the liver, kidneys, bones, and central nervous
system and may produce associated symptoms and complications. The symptoms
of secondary syphilis typically resolve without treatment within weeks or months.
Latent Syphilis (Stage 3): Latent syphilis is the third, so-called “hidden” stage of
infection. It is marked by the relative absence of symptoms and positive blood tests.
This stage is further divided into two stages:
• Early latent syphilis is the period within a year of the initial infection.
Secondary symptoms can sometimes relapse during the early latent phase.
• Late latent syphilis is the period a year after the initial infection. It can last
for years and even decades with no signs of disease.
Tertiary Syphilis (Stage 4): Tertiary syphilis is the most serious stage of this
infection and it is characterized by three major complications:
• Gummatous syphilis causes the formation of soft, tumor-like lesions called
gummas. These noncancerous lesions can cause large ulcerative sores on
the skin and mouth, and erode tissues of the heart, liver, muscles, bones, and
other vital organs. Symptoms typically develop between 3 and 10 years after
a person is first infected.
• Cardiovascular syphilis can cause severe inflammation of the aorta and
swelling and weakening of the aortic wall (aortic aneurysm). It generally
occurs 10 to 30 years after the initial infection.
• Neurosyphilis affects the central nervous system and usually develops
within four to 25 years after the initial infection. While some people will
not develop symptoms, others may experience severe issues such as
General signs and Symptoms of Syphilis include: fever, general ill feeling, joint
pain, loss of appetite, moist warty patches (called condylomata lata) in the genitals
or skin folds, muscle aches, skin rash usually on the palms of the hands and soles
of the feet, sores called mucous patches in or around the mouth, vagina or penis.
Investigations
The diagnosis of syphilis relies on:
Physical examination and clinical manifestations– a doctor or nurse will
ask to examine your genitals (and inside the vagina for women) or other parts
of your body to look for growths or rashes that may be caused by syphilis.
Blood test (Rapid plasma regain: RPR, Venereal Disease Research Laboratory:
VDRL, T. pallidum particle agglutination assay: TPPA, T. pallidum enzyme
immunoassay: TP-EIA, Polymerase chain reaction: PCR): can show whether you
have syphilis or have had it in the past; repeating the test a few weeks later may
be recommended if it’s negative, in case it was too early to give an accurate result.
Swab test – a swab is used to take a small sample of fluid from any sores, so it can
be checked for syphilis.
CSF (cerebro-spinal fluid) testing to detect neurosyphilis is strongly recommended
in patients with tertiary syphilis or with neurological signs or symptoms consistent
with neurosyphilis and in patients without symptoms whose serologic titers do not
decline appropriately after being treated with recommended therapy.
Adequate medical diagnosis
Syphilis is a sexually transmitted infection (STI) caused by a spiral-shaped
bacterium called Treponema pallidum. The infection is typically transmitted through
contact with a sore during a sexual encounter with an infected person, although a
mother can pass to her child during pregnancy. During the initial phase of infection,
the organism disseminates widely, setting the stage for subsequent manifestations.
If untreated, syphilis can have a number of significant late manifestations, including
cardiovascular, gummatous, and neurologic complications. The investigations
should be obtained just before initiating therapy (ideally, on the first day of treatment).
Penicillin is the treatment of choice for all stages of syphilis. Patients should be
monitored clinically and with serologic testing after treatment to ensure they are
responding appropriately to therapy.
Treatment plan
While syphilis infection can still be treated during the tertiary stage, any damage
caused to the heart, kidneys, and other organs may be permanent and can lead
to end-stage organ failure. Treatment is determined by the type and extent of the
damage.
A single intramuscular injection of long acting Benzathine penicillin G (2.4 million
units administered intramuscularly) will cure a person who has primary, secondary
or early latent syphilis.
Three doses of long acting Benzathine penicillin G (2.4 million units administered
intramuscularly) at weekly intervals is recommended for individuals with late
latent syphilis or latent syphilis of unknown duration. Treatment will kill the syphilis
bacterium and prevent further damage, but it will not repair damage already done.
In the treatment of late syphilis by weekly injections, missing a dose of penicillin for
a period of 10-14 days does not require restarting the entire course of injections.
The exception to this is in the case of pregnant women in whom there is no latitude
for missing a dose of penicillin.
Doxycycline is the best alternative for treating early and late latent syphilis. Syphilis
associated with HIV infection does not require any enhanced antimicrobial therapy.
For patients who are allergic to penicillin, alternative agents include tetracyclines,
cephalosporins (ceftriaxone, etc) and macrolides (azithromycin, etc). However, we
only use azithromycin if no other options are available due to concerns of treatment
failure associated with macrolide resistance
Prevention of syphilis: avoid having sex with multiple partners, avoid sharing
sex toys, get screened for sexually transmitted infections and talk to your partners
about their results, syphilis can also be transmitted through shared needles. Avoid
sharing needles if you’re going to use drugs.
Evolution and complications
Early diagnosis and initiation of treatment provides good outcome to patients with
syphilis. At its beginning stage, syphilis will cause sores called chancre in the body.
Chancres are seen mostly in genital areas of the body. Syphilis can also cause rash,
mild fever, fatigue, headache, sore throat, patchy hair loss, and swollen glands
through the body. If left untreated, syphilis can spread to all areas of the body.
If it is untreated, syphilis can cause serious long-term health
problems such as arthritis, brain damage, and blindness.
During the tertiary stage of syphilis, small, rubbery lesions may develop on the
bones, skin, nervous system tissue, and/or arteries of the heart or the brain. Due to
these lesions and other health complications, these individuals are susceptible to
heart attack, paralysis, blindness, stroke, numbness, dementia.
Complications in new-borns if the syphilis is left untreated, the symptoms may
include:
• Liver and spleen enlargement
• Purplish skin spots caused by ruptured capillaries (petechiae)
• Profuse nasal drip with highly infectious mucus discharge (known as syphilitic
“snuffles”)
• Neurosyphilis
• Lung inflammation
• Yellowing of the skin and eyes (jaundice)
• Seizures
By age 2, the child may have characteristic facial or physical deformities and
significant sensory impairment, including:
• Blunted upper front teeth (known as Hutchinson’s teeth)
• A collapse of the bony part of the nose (saddle nose)
• A protruding jawbone and foreshortened upper jaw
• A protruding frontal bone of the skull (frontal bossing)
• Swollen knees
• Bowing of the shin bones (saber shins)
• Inflammation and scarring of the cornea, the clear cover over the front of the
eye (interstitial keratitis)
• Glaucoma, a disease that damage’s the optic nerve and can cause bliness
• Deafness
• Developmental delays
Self-assessment 4.2.2
1. What is the cause of syphilis?
2. Can you list some risk factors to syphilis development?
3. Differentiate different phases/stages of syphilis.
4. Describe briefly the pathogenesis of congenital syphilis.
5. What are different investigations used to diagnose syphilis and their
rationale?
6. What are the preventive strategies for syphilis?
7. What are the treatment options are for a patient with syphilis?
8. What are the complications of syphilis?
4.2.3 GONORRHEA
Learning Activity 4.2.3
Read carefully this below situation and answer the following questions:
Mr. B.E is a 54-year-old male patient who visited RUHENGERI Hospital with
complaints of a purulent white discharge from the penis accompanied by
itching and burning sensation when urinating, painful and the physical examination
(palpation and inspection) revealed swollen testicles on palpation. The history
taking revealed that he is performed unprotected sexual intercourse with a sex
worker met in a hotel two days ago after missing condom. Body temperature
was 36.5 degree Celicius, blood pressure was 110/70 mmHg, pulse rate was
74beats per minute, respiratory rate was 19 breaths per minutes. Mr. B.E was
treated with Doxycycline tablet 100mg two times a day for 7 days associated
with a single dose of Ciprofloxacin 500mg and ibuprofen 400mg two times per
day for 3 days. After taking medication given from health center, the signs and
symptoms persisted despite the adherence of health care provider’s provided
instructions and decided to re-visit the hospital where the pus culture was
done and revealed Neisseria Gonorrhea bacterium, antibiogram showed that
the bacteria can respond to Azithromycin only among others. Other laboratory
investigations were performed and revealed white blood cells (WBC) of 150000.
1. What are abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
4. What was included in the management of this case at different levels of
health care settings he visited?
5. If not treated, what will be the consequences?
Gonorrhea is an infection caused by a sexually transmitted bacterium that
infects both males and females. It can cause infections in the genitals (the urethra,
rectum and throat). In females, gonorrhea can also infect the cervix. This sexually
transmitted disease (STD) or sexual transmission infection (STI) is a very common
infection, especially among young people ages 15-24 years.
Causes and risk factors
Gonorrhea is caused by Neisseria Gonorrhea, any sexually active person can get
gonorrhea through unprotected vaginal, anal, or oral sex. If a patient is sexually
active, must have an honest and open talk with the health care provider and ask
whether he/she should be tested for gonorrhea or other STDs. A sexually active
man who is gay, bisexual, or who has sex with men, should be tested for gonorrhea
every year. A sexually active woman younger than 25 years or an older woman
with risk factors such as new or multiple sex partners, or a sex partner, who has a
sexually transmitted infection, should be tested for gonorrhea every year.
A pregnant woman, who has gonorrhea, can give the infection to the baby during
delivery. This can cause serious health problems for the baby. If the patient is
pregnant, it is important that she talks to the health care provider so that she get
the correct examination, testing, and treatment, as necessary. Treating gonorrhea
as soon as possible will make health complications for your baby less likely.
Pathophysiology
The infection is caused by a bacterium, Neisseria gonorrhoea, which can be
transmitted heterosexually or homosexually. The microorganism invades the
urethra, vagina, rectum, or pharynx, depending on the nature of sexual contact;
it can spread throughout the body. In untreated men, the localized infection may
spread to the prostate, seminal vesicles, and epididymis. Urethral strictures may
develop, requiring periodic dilation of the urethra or, possibly, reconstructive urethral
surgery. In women, the infection may progress upward to the cervix, endometrium,
and fallopian tubes, and symptoms of pelvic inflammatory disease (PID) may
develop. Gonorrhoea also can be transmitted to an infant’s eyes at the time of birth.
Signs and symptoms of gonorrhea
In men, symptoms usually appear 2 to 6 days after infection. Urethritis with a purulent
discharge and pain on urination are the most common signs and symptoms. A small
proportion of men are asymptomatic.
More than half of infected women experience no symptoms. When symptoms do
occur, women have a white or yellow vaginal discharge, intermenstrual bleeding due
to cervicitis, and painful urination. Other symptoms may include burning or frequent
urination, yellowish vaginal discharge, redness and swelling of the genitals, and a
burning or itching of the vaginal area. If untreated, gonorrhea can lead to severe
pelvic infections and even sterility. Even when a woman has symptoms, they are
often mild and can be mistaken for a bladder or vaginal infection. Women with
gonorrhea are at risk of developing serious complications from the infection, even if
they don’t have any symptoms. Symptoms in women can include painful or burning
sensation when urinating; increased vaginal discharge; vaginal bleeding between
periods.
An anal infection is accompanied by painful bowel elimination and a purulent rectal
discharge; the throat is sore when the pharynx is infected. If the microorganism
disseminates (scatters) throughout the body, the client may manifest a skin rash,
fever, and painful joints. Men with gonorrhea may have a yellowish discharge from
the penis accompanied by itching and burning.
Complications in later life can include inflammation of the heart valves, arthritis, and
eye infections. Gonorrhea can also cause eye infections in babies born of infected
mothers.
Some men with gonorrhea may have no symptoms at all. However, men who do
have symptoms may have a burning sensation when urinating; a white, yellow, or
green discharge from the penis; painful or swollen testicles (although this is less
common).
Rectal infections may either cause no symptoms or cause symptoms in both men
and women that may include discharge; anal itching; soreness; bleeding; painful
bowel movements.
The client should be examined by the doctor if he/she notices any of these symptoms
or if his/her partner has an STD or symptoms of an STD, such as an unusual sore,
a smelly discharge, burning when urinating, or bleeding between periods.
Investigations
Swabs from pus or discharge must be sent for analysis and identify the germ
Specimens of drainage from infected tissue are examined microscopically
immediately after they are collected or are inoculated on a culture medium and
incubated to reveal the causative organism.
Other laboratory blood tests (FBC, electrolytes, Renal and liver function tests,
etc) might be helpful to look for other existing conditions.
Medical diagnosis
The medical diagnosis of gonorrhea is based on the clinical manifestation of the
clients as well as the history taking and laboratory findings where possible.
Most of the time, urine can be used to test for gonorrhea. However, if the client has
had oral and/or anal sex, swabs may be used to collect samples from the throat
and/or rectum. In some cases, a swab may be used to collect a sample from a
man’s urethra (urine canal) or a woman’s cervix (opening to the womb).
Treatment plan
The microorganism N. gonorrhoea has become increasingly resistant to penicillin,
tetracycline, and fluoroquinolones.
Therefore, currently CDC (2006) recommendation for treating gonorrhoea is a
single intramuscular dose of a broad-spectrum cephalosporin such as ceftriaxone
(rocephin) or oral dosing with cefixime (suprax). Coinfection with chlamydia
is common; therefore, clients also are given a single dose of oral azithromycin
(zithromax) or oral doxycycline (vibramycin) for 7 to 10 days. Clients with complicated
gonococcal infections, as in PID or disseminated infection, are hospitalized and
treated with IV multiple-drug therapy.
The nursing management and client teaching are similar for those clients other
STDs. However, when a culture is collected from a woman, the vaginal speculum
is moistened with water rather than lubricated, because lubricant may destroy the
gonococci and cause inaccurate test results.
Evolution and complications
Untreated gonorrhoea can cause serious and permanent health problems in both
men and women.
In women, untreated gonorrhoea can cause pelvic inflammatory disease (PID).
Some of the complications of PID are formation of scar tissue that blocks fallopian
tubes external icon, ectopic pregnancy (pregnancy outside the womb external
icon), infertility (inability to get pregnant); long-term pelvic/abdominal pain,
untreated gonorrhea may also increase your chance of getting HIV, the virus that
causes AIDS.
In men, gonorrhoea can cause a painful condition in the tubes attached to the
testicles. In rare cases, this may cause a man to be sterile. Rarely, untreated
gonorrhoea can also spread to your blood or joints. This condition can be life-threatening.
Self-assessment 4.2.3
1. What is gonorrhoea?
2. Describe the causes and triggering factors contributing to the gonorrhoea
development.
3. What are different treatment options for a patient with gonorrhoea?
4. State the preventive measures to be taken to prevent gonorrhoea
5. What are possible investigations to be performed to confirm gonorrhoea?
6. If acute gonorrhoea is not well treated effetely, what could be the
complications?
4.2.4 HIV Infection (Human Immunodeficiency Virus Infection)
Learning Activity 4.2.4
Carefully read the case study below and answer the following questions:
The patient M.V a 24-year-old female who had spent 6 months in Matimba/
Biryogo consulted Muhima hospital for repetitive flu like syndrome, episode
of fevers and generalized body weakness with fatigue. A few weeks ago she
became ill with general body weakness, lymphadenopathy and fever of 39.2 o
C. All laboratory investigations requested (blood smear negative, FBC normal)
were normal and was given paracetamol 1g TDS for 5 days. During the current
visit she was further examined and denied recent sexual contacts, her marital
status is single and lives alone in a house. She reported to be unemployed
and stated that it is very difficult to find living means. Laboratory tests as FBC,
Urea and creatinine, ASAT and ALAT, HIV test and blood culture were ordered
and the health care professionals decided to hospitalise her and put her on IV
paracetamol 100mg TDS for 3 days and IV ceftriaxone 1gr BID for 7 days while
waiting for all results. The results became as normal FBC and a positive ELISA
test for HIV.
As the counselling was not done for HIV prior testing, they proceeded on
counselling and retested for HIV using rapid test to be able to communicate
results. The HIV rapid test became positive too and counselling for possible
initiation of antiretroviral drugs started. During this counselling, she reported
that she get living means from selling her sex and this was also known by her
neighbours. As she was unstable, they waited until to be stable for CD4 control
to decide on initiation of ARV drugs.
1. What was the medical diagnosis the patient was presenting?
2. What were the risks factors that exposed her to develop that medical
condition?
3. What must be considered before initiating the treatment to that condition?
4. What are different investigations are useful to decide on the management
of that medical condition?
5. What are different drugs you know that are used to treat that medical
condition?
6. What are the possible complications related to that medical condition?
HIV (human immunodeficiency virus) is a virus that attacks the immune system,
the body’s natural defence system. Without a strong immune system, the body
has trouble fighting off disease. Both the virus and the infection are called HIV.
White blood cells are an important part of the immune system. HIV infects and
destroys certain white blood cells called CD4+ cells. If too many CD4+ cells are
destroyed, the body can no longer defend itself against infection. The last stage of
HIV infection is AIDS (Acquired Immunodeficiency Syndrome). People with AIDS
have a low number of CD4+ cells and get infections or cancers that rarely occur in
healthy people. These can be deadly. But having HIV doesn’t mean you have AIDS.
Causes and Risk Factors
HIV infection is caused by the human immunodeficiency virus. HIV doesn’t
survive well outside the body, therefore it can’t be spread by casual contact like
kissing or sharing drinking glasses with an infected person. The patient can’t
catch HIV or AIDS by hugging, kissing, dancing or shaking hands with someone
who has the infection. HIV isn’t spread through the air, water or insect bites.
The HIV can be contaminated/transmitted from contact with infected blood, semen,
or vaginal fluids. This can happen in several ways:
By having sex: Infection comes if there is unprotected sexual intercourse being
vaginal, anal or oral with an infected partner whose blood, semen or vaginal
secretions enter your body. The virus can enter the body through mouth sores or
small tears that sometimes develop in the rectum or vagina during sexual activity.
By sharing needles: Sharing contaminated used IV drug materials (needles and
syringes) puts a person at high risk of HIV and other infectious diseases, such
as hepatitis. Health care professionals can get the HIV infections when not being
careful while giving injections or through blood sample collection due to needle
stick injuries while caring for HIV patients.
From blood transfusions: In some cases, the virus may be transmitted through
blood transfusions.
During pregnancy or delivery or through breast-feeding: Infected mothers can
pass the virus on to their babies. Mothers who are HIV-positive and get treatment
for the infection during pregnancy can significantly lower the risk to their babies.
The virus can also be passed from a mother to her baby during pregnancy, birth, or
breastfeeding.
The other greatest risk of HIV/AIDS are:
Have unprotected sex: Anal sex is more risky than is vaginal sex; and the risk
of HIV increases if there are multiple sexual partners.
Have an STI: Many STIs produce open sores on the genitals, and those sores act
as doorways for HIV to enter your body.
Pathophysiology
HIV destroys CD4+ cells in 3 ways: Viral replication leaves the holes in the cell
membranes, Infected cells fuse with other cells, Antibodies against HIV bind to the
infected cells and activate the complement system, which destroy the infected cells.
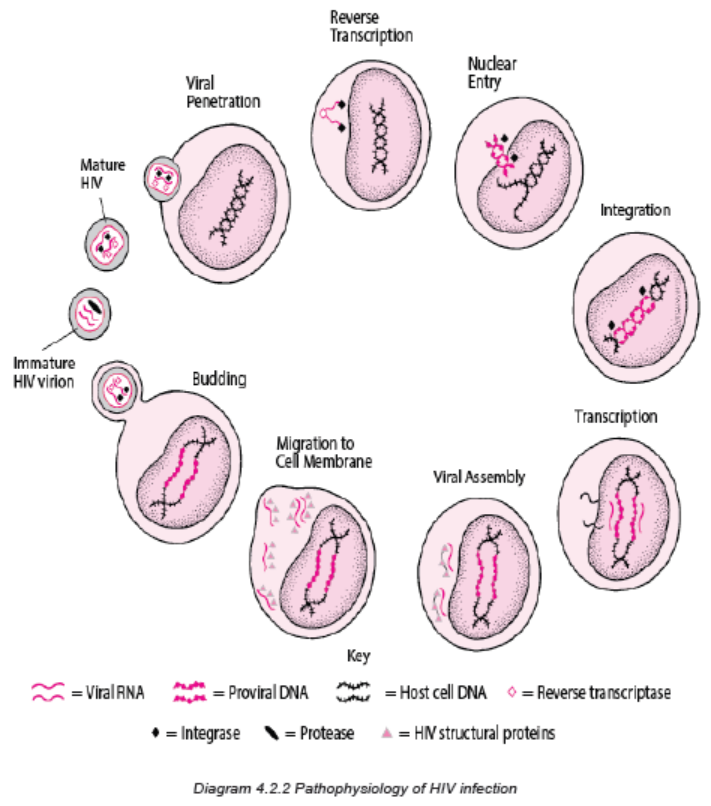
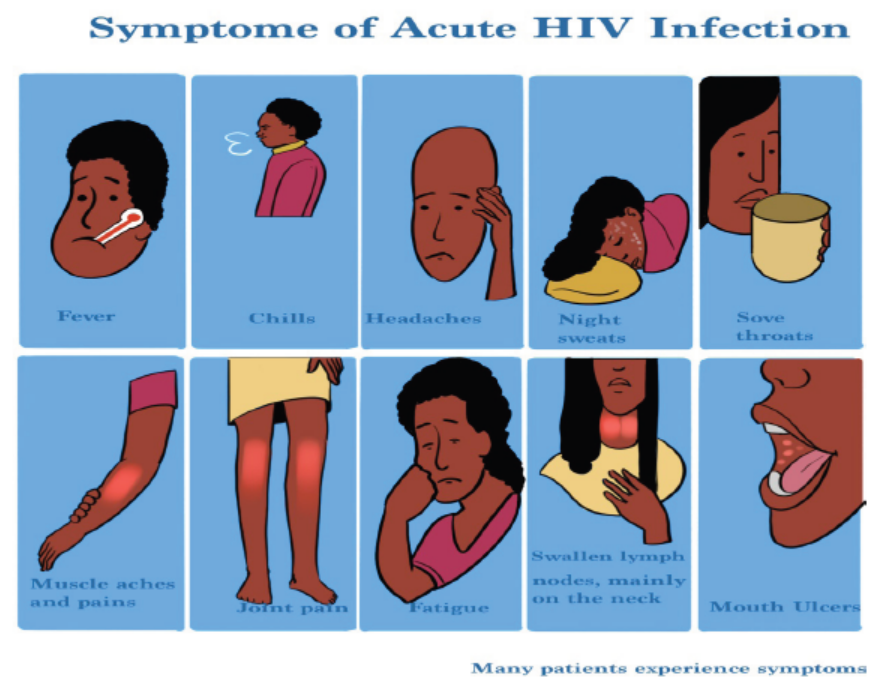
Figure4.2.4 Signs and symptoms of HIV infection
The symptoms of HIV and AIDS vary depending on the phase of infection:
Primary infection (Acute HIV): Some people infected by HIV develop a flu-like
illness within two to four weeks after the virus enters the body. This illness, known
as primary (acute) HIV infection, may last for a few weeks. Possible signs and
symptoms include fever, headache, muscle aches and joint pain, rash, sore throat
and painful mouth sores, swollen lymph glands, mainly on the neck, diarrhea,
weight loss, cough, night sweats.
These symptoms can be mild that the patient might not even notice them. However,
the amount of virus in your bloodstream (viral load) is quite high at this time. As a
result, the infection spreads more easily during primary infection than during the
next stage.
Clinical latent infection (Chronic HIV): In this stage of infection, HIV is still
present in the body and in white blood cells. However, many people may not have
any symptoms or infections during this time. This stage can last for many years if
the patient is not receiving antiretroviral therapy (ART). Some people develop more
severe disease much sooner.
Symptomatic HIV infection: As the virus continues to multiply and destroy the
immune cells (the cells in your body that help fight off germs) may develop mild
infections or chronic signs and symptoms such as fever, fatigue, swollen lymph
nodes often one of the first signs of HIV infection, diarrhea, weight loss, oral yeast
infection (thrush), shingles (herpes zoster), pneumonia.
Progression to AIDS: Untreated, HIV typically turns into AIDS. When AIDS occurs,
the immune system has been severely damaged. The patient is more likely to
develop opportunistic infections or opportunistic cancers or diseases that wouldn’t
usually cause illness in a person with a healthy immune system. The signs and
symptoms of some of these infections may include sweats, chills, recurring fever,
chronic diarrhea, swollen lymph glands, persistent white spots or unusual lesions
on your tongue or in your mouth, persistent or unexplained fatigue, weakness,
weight loss, skin rashes or bumps.
Investigations
Diagnosing HIV should be done basing on:
Clinical suspicion: due to the wide range of symptoms associated with acute
HIV infection, the possibility of HIV infection should be considered in patients who
present with the more typical signs and symptoms, including an ill-defined febrile
illness, heterophile-negative mononucleosis-like syndrome, heterophile positive
mononucleosis in an unusual host (for example, an older adult patient), and/or
aseptic meningitis. Certain clinical features, such as a rash, mucocutaneous ulcers,
diarrhea, or lymphadenopathy, should heighten the suspicion for HIV infection
HIV can be diagnosed through blood or saliva testing. During the use of blood
test to diagnose HIV infection, If the test is positive (meaning that HIV antibodies or
antigens are found), a test to detect HIV DNA or RNA will be done to be sure. HIV
antibodies may show up in the blood as early as 2 to 4 weeks after contact but can
also take as long as 3 to 6 months to show up in the blood.
When the possibility of acute or early HIV infection is being considered, we perform
the most sensitive screening immunoassay available (ideally, a combination
antigen/antibody immunoassay) in addition to an HIV virologic (viral load) test. We
favor using an RT-PCR based viral load test, if available. A positive HIV virologic
test is generally indicative of HIV infection
Available tests include:
• Antigen/antibody tests: These tests usually involve drawing blood from a
vein. Antigens are substances on the HIV virus itself and are usually detectable
— a positive test — in the blood within a few weeks after exposure to HIV.
• Antibodies are produced by the immune system when it’s exposed to HIV.
It can take weeks to months for antibodies to become detectable. The
combination antigen/antibody tests can take two to six weeks after exposure
to become positive.
• Antibody tests: These tests look for antibodies to HIV in blood or saliva.
Most rapid HIV tests, including self-tests done at home, are antibody tests.
Antibody tests can take three to 12 weeks after the patient is exposed to
become positive.
• Nucleic acid tests (NATs): These tests look for the actual virus in your
blood (viral load). They also involve blood drawn from a vein. If you might
have been exposed to HIV within the past few weeks, the doctor may
recommend NAT. NAT will be the first test to become positive after exposure
to HIV
• In addition to these tests, there is need of general screening to look for
hemodynamic and physiological status of a person suspected (FBC, Urea,
Creatinine, electrolytes, ASAT and ALAT and any other helpful investigation
depending on patient condition).
Once the patient thinks that he/she has been exposed to HIV but the test is negative,
should get tested again. A repeat test can be done after a few weeks to be sure he/
she is not infected.
After the confirmation of diagnosis of HIV/AIDS, several tests can help the clinician
to determine the stage of the disease and the best treatment:
CD4 T cell count: CD4 T cells are white blood cells that are specifically targeted
and destroyed by HIV. Even if the patient doesn’t have symptoms, HIV infection
progresses to AIDS when the CD4 T cells count below 200.
Viral load (HIV RNA): This test measures the amount of virus in your blood.
After starting HIV treatment the goal is to have an undetectable viral load. This
significantly reduces your chances of opportunistic infection and other HIV-related
complications.
Drug resistance: Some strains of HIV are resistant to medications. This test helps
the clinician to determine if the specific form of the virus has resistance and guides
treatment decisions.
Treatment plan
The standard treatment for HIV is a combination of medicines called antiretroviral
therapy or ART or ARV drugs. Antiretroviral medicines slow the rate at which the
virus multiplies. Taking these medicines can reduce the amount of virus in the body
and help to stay healthy.
Preventive strategies
There’s no vaccine to prevent HIV infection and no cure for AIDS. But you can
protect yourself and others from infection.
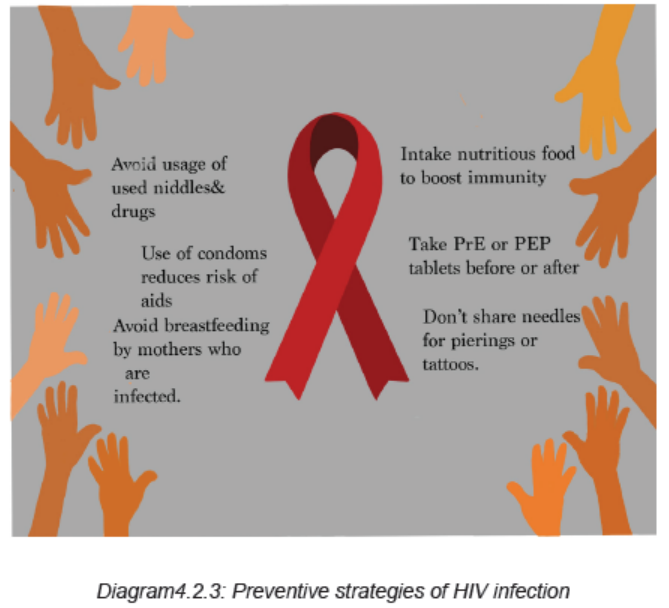
To help to prevent the spread of HIV:
Use treatment as prevention: If living with HIV, taking HIV medication can keep
the partner from becoming infected with the virus. If the viral load stays undetectable
(a blood test doesn’t show any virus) the patient will not transmit the virus to anyone
else. This requires taking the medication exactly as prescribed and getting regular
check-ups.
Use post-exposure prophylaxis (PEP) after being exposed to HIV: If exposed
through sex, needles or in the workplace, contact the doctor or go to the emergency
department or HIV clinic. Taking PEP as soon as possible within the first 72 hours
can greatly reduce the risk of becoming infected with HIV. Patient will need to take
medication for 28 days.
Use a new condom every time having sex: Use a new condom every time client
has anal or vaginal sex. Women can use a female condom. If using a lubricant,
make sure it’s water based. Oil based lubricants can weaken condoms and cause
them to break.
Consider Pre-exposure prophylaxis (PrEP): The combination drugs emtricitabine
plus tenofovir (Truvada) and emtricitabine plus tenofovir alafenamide (Descovy)
can reduce the risk of sexually transmitted HIV infection in people at very high
risk. PrEP can reduce the risk of getting HIV from sex by more than 90% and from
injection drug use by more than 70%, according to the Centers for Disease Control
and Prevention. Client will need an HIV test before start taking PrEP and then every
three months as long as he/she is taking it. The doctor will also test the kidney
function before prescribing Truvada and continue to test it every six months. These
PrEP drugs don’t prevent other STIs, so patient still need to practice safe sex. If
client has hepatitis B or C, he/she should be evaluated for any infectious disease or
liver disease before beginning therapy.
Tell the sexual partners if client has HIV: It›s important to tell all the current and
past sexual partners that client is HIV-positive. They›ll need to be tested.
Use a clean needle: If using a needle to inject drugs, make sure it›s sterile and
don›t share it. Take advantage of needle-exchange programs in the community.
Consider seeking help for the drug use.
If client is pregnant, get medical care right away: If client is HIV-positive, she
may pass the infection to the baby. But if she receives treatment during pregnancy,
she can significantly cut the baby›s risk.
Consider male circumcision: There›s evidence that male circumcision can help
reduce the risk of getting HIV infection.
Adequate medical diagnosis
A variety of symptoms and signs may be seen in association with acute HIV
infection, known as the acute retroviral syndrome. The most common findings are
fever, lymphadenopathy, sore throat, rash, myalgia/arthralgia, and headache.
The diagnosis of acute HIV infection requires a high level of clinical suspicion and
should be considered in patients who present with consistent signs and symptoms,
including an ill-defined febrile illness, heterophile-negative mononucleosis-like
syndrome, and/or aseptic meningitis. Early HIV infection should also be considered
in patients who have had a recent high-risk exposure or those who have had a
recent sexually transmitted infection regardless of the presence of symptoms or
signs. When the possibility of acute or early HIV infection is being considered, we
perform the most sensitive immunoassay available (ideally, a combination antigen/
antibody immunoassay) in addition to an HIV virologic (viral load) test. A positive
virologic test indicates HIV infection.
All patients with suspected or confirmed acute or early HIV infection should be
counseled to adopt behaviors that guard against HIV transmission, including
consistent and correct condom use and avoidance of sharing injection drug use
equipment and develop other positive behaviors towards other people.
There is no cure of HIV but the standard treatment for HIV is a combination of
medicines called antiretroviral therapy or ART or ARV drugs. Antiretroviral medicines
slow the rate at which the virus multiplies. Taking these medicines can reduce the
amount of virus in your body and help you stay healthy.
Evolution and Complications
There’s no vaccine to prevent HIV infection and no cure for it. Taking the ART
medicines can reduce the amount of virus in the body and help to stay healthy.
There is also need of protecting yourself and others from infection.
HIV infection weakens the immune system, making the person much more likely to
develop many infections and certain types of cancers:
Infections common to HIV/AIDS:
Pneumocystis pneumonia (PCP): This fungal infection can cause severe illness.
Although it›s declined significantly with current treatments for HIV/AIDS, the PCP is
still the most common cause of pneumonia in people infected with HIV.
Candidiasis (thrush): Candidiasis is a common HIV-related infection. It causes
inflammation and a thick, white coating on the mouth, tongue, esophagus or vagina.
Tuberculosis (TB): In resource-limited nations, TB is the most common
opportunistic infection associated with HIV. It›s a leading cause of death among
people with AIDS.
Cytomegalovirus: This common herpes virus is transmitted in body fluids such as
saliva, blood, urine, semen and breast milk. A healthy immune system inactivates
the virus, and it remains dormant in the body. If the immune system weakens, the
virus resurfaces causing damage to the eyes, digestive tract, lungs or other organs.
Cryptococcal meningitis: Meningitis is an inflammation of the membranes and
fluid surrounding the brain and spinal cord (meninges). Cryptococcal meningitis is a
common central nervous system infection associated with HIV, caused by a fungus
found in soil.
Toxoplasmosis: This potentially deadly infection is caused by Toxoplasma gondii,
a parasite spread primarily by cats. Infected cats pass the parasites in their stools,
which may then spread to other animals and humans. Toxoplasmosis can cause
heart disease, and seizures occur when it spreads to the brain.
Cancers common to HIV/AIDS:
Lymphoma: This cancer starts in the white blood cells. The most common early
sign is painless swelling of the lymph nodes in the neck, armpit or groin.
Kaposi›s sarcoma: A tumor of the blood vessel walls, Kaposi›s sarcoma usually
appears as pink, red or purple lesions on the skin and mouth. In people with darker
skin, the lesions may look dark brown or black. Kaposi›s sarcoma can also affect
the internal organs, including the digestive tract and lungs.
Other complications related to HIV infection:
Wasting syndrome: Untreated HIV/AIDS can cause significant weight loss, often
accompanied by diarrhea, chronic weakness and fever.
Neurological complications: HIV can cause neurological symptoms such as
confusion, forgetfulness, depression, anxiety and difficulty walking. HIV-associated
neurocognitive disorders can range from mild symptoms of behavioral changes and
reduced mental functioning to severe dementia causing weakness and inability to
function.
Kidney disease: HIV associated nephropathy is an inflammation of the tiny filters
in the kidneys that remove excess fluid and wastes from the blood and pass them
to the urine.
Liver disease: Liver disease is also a major complication, especially in people who
also have hepatitis B or hepatitis C.
Self-assessment 4.2.4
1. Describe briefly the steps of HIV infection pathogenesis
2. What are different classes of ART drugs and their site of actions?
3. Describe different coping skills needed towards HIV preventive strategies
4. Differentiate signs and symptoms depending on the different phases of
HIV
5. Discuss different complications of HIV
4.2.5 Human Papilloma Virus (HPV)
Learning Activity 4.2.5
Read carefully this below situation and answer the following questions:
Mrs. N, V is a 39-year-old female patient who visited MUHIMA Hospital with
complaints of itching, burning, and discomfort of the genital area and the physical
examination (palpation and inspection) revealed large, pink, flat shaped wart
on the vulva. The history taking revealed that she is HIV Positive and treated
on Highly Antiretroviral therapy (HAAT) initiated 2 years ago as she delayed to
get tested for HIV/AIDs. Her vital signs were body temperature of 36.5 degree
Celsius, blood pressure of 100/70 mmHg, pulse rate was 68 beats per minute,
respiratory rate was 19 breaths per minute. The pap smear and DNA tests were
performed from vulva and cervical tissues and revealed abnormal cell growth,
the physician encouraged her to adhere to the ARVs treatment and salicylic
acid was prescribed to be applied on the affected area.
1. What are abnormal signs and symptoms that patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been ordered to guide the confirmation
of the medical problem?
4. What was included in the management of this case at different levels of
health care settings he visited?
5. If not treated, what will be the consequences?
Human papillomavirus is an infection caused by human papillomavirus (HPV), a
DNA virus from the papillomaviridae family.
Causes and risk factors
HPV infection occurs when the virus (human papillomavirus: HPV, a DNA virus
from the papillomaviridae family) enters the human body, usually through a cut,
abrasion or small tear in the skin. The virus is transferred primarily by skin-to-skin
contact.
Genital HPV infections are contracted through sexual intercourse, anal sex and
other skin-to-skin contact in the genital region. Some HPV infections that result in
oral or upper respiratory lesions are contracted through oral sex.If a client is pregnant and has an HPV infection with genital warts, it’s possible her
baby may get the infection. Rarely, the infection may cause a noncancerous growth
in the baby’s voice box (larynx).
Warts are contagious. They can spread through direct contact with a wart. Warts
can also spread when someone touches something that already touched a wart.
The Risk factors for HPV infection include number of sexual partners (The
more sexual partners that the client has, the more likely he/she is to contract a
genital HPV infection. Having sex with a partner who has had multiple sex partners
also increases the risk), Age (Common warts occur mostly in children. Genital warts
occur most often in adolescents and young adults), Weakened immune systems
(People who have weakened immune systems are at greater risk of HPV infections.
Immune systems can be weakened by HIV/AIDS or by immune system-suppressing
drugs used after organ transplants).
Other risks are damaged skin (Areas of skin that have been punctured or
opened are more prone to develop common warts), Personal contact (Touching
someone’s warts or not wearing protection before contacting surfaces that have
been exposed to HPV such as public showers or swimming pool might increase the
risk of HPV infection unprotected intercourse, numerous sexual partners and age at
first intercourse), Teens that are sexually active and young adult females are at
a higher risk of contracting the virus, than women and men over 25, the people who
are immunocompromised, such as young adults with HIV, Smokers have higher
rates of HPV infection, Contracting herpes or chlamydia increases the risk of
HPV infection “due to inflammation of the epithelial cells and breaks in the epithelial
layer that allows a pathway for HPV introduction”.
HPV can pass from person to person regardless of whether symptoms are present.
The strains of HPV that cause warts are different from those that increase the risk
of cancer.
In children, HPV can transmit to an infant during birth. However, research suggests
that this risk is relatively low, as the immune system usually takes care of the
infection in this situation. Signs of an HPV infection in an infant include genital warts
or lesions in the mouth. If a young child develops HPV symptoms, it may indicate
child abuse.
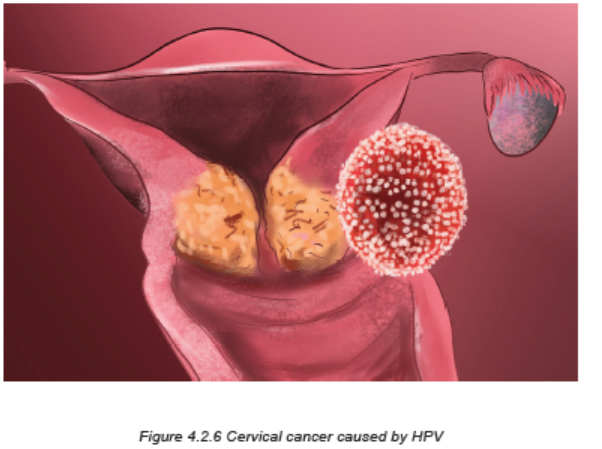
Pathophysiology overview
The HPV virus is a small, non-enveloped, double stranded DNA virus that infects
the mucosal or cutaneous epithelium. Since HPV affects epithelial cells and does
not enter the bloodstream, having an HPV infection in one part of the body should
not cause infection in another part. Once HPV gets into the epithelial cell, the virus
begins to make proteins that can interfere with normal functions in the cell, enabling
the cell to grow in an uncontrolled manner and to avoid apoptosis. HPV modifies
the DNA damage response (DDR) pathways by interacting with many proteins,
including ATM, ATR, MRN, y-H2AX, Chk1, Chk2, p53, BRCA1, BRCA2, RAD51,
etc. The HPV virus can activate and dysregulate DDR pathways throughout various
stages of their life cycles to replicate itself in host cells. Cell biology during a different
periods of a woman’s life can make her more susceptible to contracting the virus.
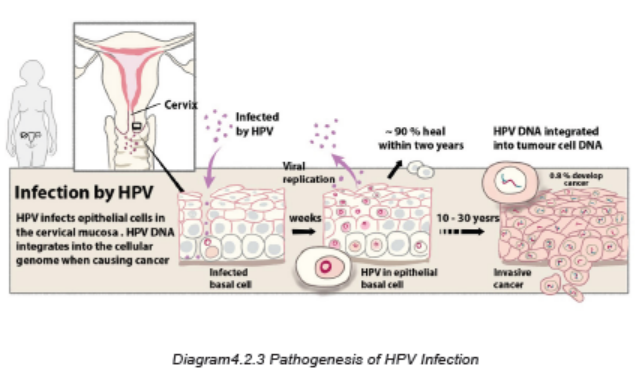
Signs and symptoms
Once infected, many patients remain asymptomatic and most cases resolve on
their own. The virus can remain dormant for years and then appear untriggered.
Appearance of ano-genital warts or abnormal pap smears are signs of likely HPV
infection.
In most cases, the body’s immune system defeats an HPV infection before it creates
warts. Symptoms of HPV may appear years after the initial infection. Some types of
the virus cause warts to form, while others can increase the risk of cancer. A person
may have one small skin bump, a cluster of bumps, or stem-like protrusions. These
warts can range in size and appearance, and they may be large or small, flat or
cauliflower-shaped, white, pink, red, purplish-brown, or skin-colored. The warts can
be formed on the vulva, cervix, penis or scrotum, anus, groin area, face or at any
part of the musculoskeletal system. These warts can cause itching, burning, and
other discomfort. When warts do appear, they vary in appearance depending on
which kind of HPV is involved:
Genital warts: These appear as flat lesions, small cauliflower-like bumps or tiny
stem like protrusions. In women, genital warts appear mostly on the vulva but can
also occur near the anus, on the cervix or in the vagina. In men, genital warts
appear on the penis and scrotum or around the anus. Genital warts rarely cause
discomfort or pain, though they may itch or feel tender.
Common warts: Common warts appear as rough, raised bumps and usually occur
on the hands and fingers. In most cases, common warts are simply unsightly, but
they can also be painful or susceptible to injury or bleeding
Plantar warts: Plantar warts are hard, grainy growths that usually appear on the
heels or balls of the feet. These warts might cause discomfort.
Flat warts: Flat warts are flat-topped, slightly raised lesions. They can appear
anywhere, but children usually get them on the face and men tend to get them in
the beard area. Women tend to get them on the legs. Flat warts are smaller and
smoother than other warts. They generally occur on the face or legs and are more
common in children and teens than in adults.
Female genital warts: Genital warts are a common sexually transmitted infection.
They can appear on the genitals, in the pubic area or in the anal canal. In women,
genital warts can also grow inside the vagina.
Male genital warts: Genital warts are a common sexually transmitted infection.
They can appear on the genitals, in the pubic area or in the anal canal.
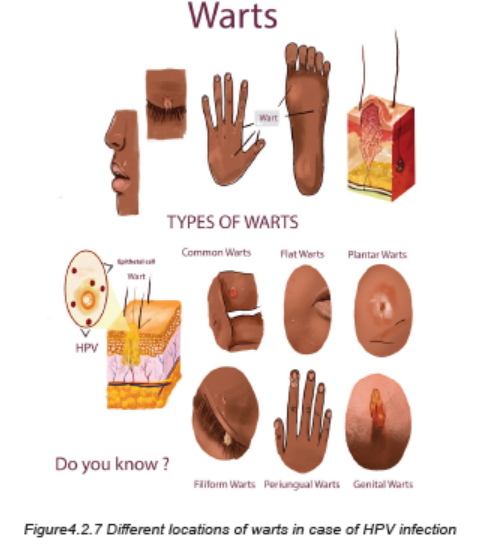
HPV and cervical cancer: nearly all cervical cancers are caused by HPV infections,
but cervical cancer may take 20 years or longer to develop after an HPV infection.
The HPV infection and early cervical cancer typically do not cause noticeable
symptoms. Being vaccinated against HPV infection is the best protection from
cervical cancer.
Because early cervical cancer does not cause symptoms, it is vital that women have
regular screening tests to detect any precancerous changes in the cervix that might
lead to cancer. Current guidelines recommend that women ages 21 to 29 have a
Pap test every three years. Women ages 30 to 65 are advised to continue having a
Pap test every three years, or every five years if they also get the HPV DNA test at
the same time. Women over 65 can stop testing if they have had three normal Pap
tests in a row, or two HPV DNA and Pap tests with no abnormal results.
Investigations
Specimens from cervical tissue are examined microscopically immediately after
they are collected to reveal the abnormal cells growth, vinegar (acetic acid) solution
test. A vinegar solution applied to HPV-infected genital areas turns them white. This
may help in identifying difficult-to-see flat lesions.
Pap test: the doctor collects a sample of cells from your cervix or vagina to send
for laboratory analysis. Pap tests can reveal abnormalities that can lead to cancer.
DNA test: This test, conducted on cells from the suspect’s cervix, can recognize the
DNA of the high-risk varieties of HPV that have been linked to genital cancers. It›s
recommended for women 30 and older in addition to the Pap test.
The WHO recommends 3 different types of screening tests: HPV DNA testing for
high-risk HPV types, Visual inspection with Acetic Acid (VIA), conventional (Pap)
test and liquid-based cytology (LBC).
Adequate medical diagnosis
Human papillomavirus (HPV) is the most common sexually transmitted infection
(STI).
Many people with HPV don’t develop any symptoms but can still infect others
through sexual contact. HPV infection is a viral infection that commonly causes skin
or mucous membrane growths (warts). Symptoms may include warts on the genitals
or surrounding skin. An infection that causes warts in various parts of the body,
depending on the strain. If the warts are not visible, several tests/investigations can
be done to diagnose the HPV infection.
There is no cure for the virus and warts may go away on their own. Treatment
focuses on removing the warts. HPV vaccines work best if administered prior to
exposure to HPV. Therefore, WHO recommends to vaccinate girls, aged between
9 and 14 years, when most have not started sexual activity. A vaccine prevents the
HPV strains most likely to cause genital warts and cervical cancer is recommended
for boys and girls.
The vaccines cannot treat HPV infection or HPV-associated disease, such as
cancer. Because pre-cancerous lesions take many years to develop, screening
is recommended for every woman from aged 30 and regularly afterwards
(frequency depends on the screening test used). For women living with HIV who
are sexually active, screening should be done earlier, as soon as they know their
HIV status. Screening has to be linked to treatment and management of positive
screening tests.
Treatment plan
Medications to eliminate warts are typically applied directly to the lesion and
usually take many applications before they’re successful. Examples include:
Salicylic acid: Over-the-counter treatments that contain salicylic acid work by
removing layers of a wart a little at a time. For use on common warts, salicylic acid
can cause skin irritation and isn’t for use on the face.
Imiquimod: This prescription cream might enhance the immune system›s ability
to fight HPV. Common side effects include redness and swelling at the application
site.
Podofilox: Another topical prescription, podofilox works by destroying genital wart
tissue. Podofilox may cause burning and itching where it›s applied.
Trichloroacetic acid: This chemical treatment burns off warts on the palms, soles
and genitals. It might cause local irritation.
If medications don’t work, surgical management for treatment of pre-cancer
lesions will be used. WHO recommends the use of cryotherapy or thermal ablation/
Burning with an electrical current, Laser susrgery and Loop Electrosurgical Excision
Procedure (LEEP)/surgical removal when available. For advanced lesions,
women should be referred to gynaecologist for further investigations and adequate
management
For abnormal HPV or Pap test, the gynaecologist will perform a procedure called
a colposcopy. Using an instrument that provides a magnified view of the cervix
(colposcope), he/she will look closely at the cervix and take samples (biopsy) of any
areas that look abnormal.
Preventive measures
It’s difficult to prevent HPV infections that cause common warts. If there is a common
wart, prevent the spread of the infection and formation of new warts by not picking
at a wart and not biting your nails.
To reduce the risk of contracting HPV infections that cause plantar warts, wear
shoes or sandals in public pools and locker rooms.
To reduce the risk of developing genital warts and other HPV-related genital lesions,
there is need of being in a mutually monogamous sexual relationship, reducing
the number of sex partners, using a latex condom, which can reduce the risk
of HPV transmission.
HPV vaccine: Gardasil-9 is an HPV vaccine approved and can be used for males
and females to protect against cervical cancer and genital warts. CDC recommends
routine HPV vaccination for girls and boys ages from 9 to 14. It’s ideal for girls
and boys to receive the vaccine before they have sexual contact and are exposed
to HPV. Once someone is infected with HPV, the vaccine might not be as effective
or might not work at all.
Nurses play a key role in education and advocacy for receiving the vaccine. Nurses
must focus their care and health education on STI screenings, reproductive health
needs, lifestyle modifications, and primary prevention, and risk reduction education.
Evolution and complications
The human papilloma virus may cause oral and upper respiratory
lesions. Some HPV infections cause lesions on the tongue, tonsils, soft palate, or
within the larynx and nose.
Genital warts that go untreated may eventually cause abnormal urine flow in men (if
warts are present in the urethra); bleeding from the urethra, vagina, or anus; or
vaginal discharge.
The Pap test and HPV tests can detect cervical changes at an early stage, so that
cervical cancer can be avoided, in most cases. The HPV types that cause genital
warts are not linked to cancer, but some other types of HPV that also infect the
mucous membranes are linked to cancers. While most of those HPV infections
never cause any symptoms, some cause changes in the cells that eventually can
lead to cancer. High-risk types of HPV can cause these different types of cancers:
cervical cancer, vulvar cancer, vaginal cancer, penile cancer, anal cancer, cancer
of the back of the throat. There are no screening tests for the other types of
cancer caused by HPV, so it’s important to notice any changes in appearance,
lumps, skin changes, pain, abnormal bleeding, or any other abnormalities in the
areas potentially infected with HPV
Self-assessment 4.2.5
1. What is Human Papilloma virus?
2. Describe the causes and triggering factors contributing to the human
Papilloma Virus development
3. What are different treatment options for a patient with Human Papilloma
virus infection?
4. State the preventive measures to be taken to prevent Human Papilloma
Virus
5. What are possible investigations to be performed to diagnose HPV?
6. If HPV is not well treated effetely, what could be the complications?
4.2.6 HEPATITIS B
Learning Activity 4.2.6
Carefully read the case scenario below and answer the following
questions
A 28-year-old female presents to the clinic with a 10-day history of flu-like
symptoms, including anorexia and malaise. She does not report any pertinent
prior medical history or surgeries. She takes no medications. Her family history
is non-contributory, and she reports no sick contacts. She is sexually active with
multiple partners and has used oral contraceptives regularly for the past 12
years.
On physical examination, she is alert and oriented, in no acute distress. Her vital
signs are temperature of 38 degree celsius, pulse 78 beats/minute, respirations of
18 cycles/minute, and blood pressure of 121/78 mmHg. Her extraocular muscles
are intact; however, mild scleral icterus is noted. Heart sounds are regular rate
and rhythm without murmurs, and lungs are clear to auscultation bilaterally. The
abdomen is soft and not tender, except the liver that is tender when palpated and
extends 8 cm below the costal margin, with a smooth edge.
Initial laboratory testing is performed and shown Complete blood count
(CBC) that is within normal limits. Liver function tests are performed, and the
significant findings are Alanine aminotransferase (ALT) 3817 U/L (Normal 7-55
U/L), Aspartate aminotransferase (AST) 2152 U/L (Normal 8-48 U/L), Alkaline
phosphatase (ALP) 176 U/L (Normal 45-115 U/L), Albumin 3.4 g/dL (Normal 3.5-
5 g/dL), Total protein 6.7 g/dL (Normal 6.3-7.9 g/dL), Total bilirubin 8.5 mg/dL
(Normal 0.1-1.2 g/dL). Viral Serology for Hepatitis B revealed HBsAg Positive
(hepatitis B surface antigen), HBeAg (hepatitis B envelope antigen) Positive,
IgM Anti-HB core Positive, Ig (immunoglobulin) G Anti-HBe Negative, IgG Anti-
HBs Negative, Hepatitis B Virus-DNA Positive
1. Given the clinical case, what were the abnormal signs and symptoms the
patient was presenting?
2. What is mostly the medical diagnosis?
3. What are the causes and risk factors of developing the medical condition
described above?
4. What are different possible treatments of that medical condition?
5. What are the complications related to that medical condition?
Hepatitis B is a potentially life-threatening liver infection caused by the hepatitis
B virus (HBV). It can cause chronic infection and puts people at high risk of death
from cirrhosis and liver cancer. Hepatitis B is a serious liver infection caused by the
hepatitis B virus (HBV). For some people, hepatitis B infection becomes chronic,
meaning it lasts more than six months. Having chronic hepatitis B increases your
risk of developing liver failure, liver cancer or cirrhosis a condition that permanently
scars of the liver.
Hepatitis B infection may be either short-lived (acute) or long lasting (chronic).
Acute hepatitis B infection lasts less than six months. The immune system likely
can clear acute hepatitis B from the body, and patient should recover completely
within a few months. Most people who get hepatitis B as adults have an acute
infection, but it can lead to chronic infection.
Chronic hepatitis B infection lasts six months or longer. It lingers because the
immune system can›t fight off the infection. Chronic hepatitis B infection may last
a lifetime, possibly leading to serious illnesses such as cirrhosis and liver cancer.
Causes and risk factors
Hepatitis B infection is caused by the hepatitis B virus (HBV). The virus is passed
from person to person through blood, semen, or other body fluids. It does not spread
by sneezing or coughing.
Common ways that HBV can spread are:
Sexual contact: when having unprotected sex with someone who is infected. The
virus can be transmitted if the person’s blood, saliva, semen, or vaginal secretions
enter someone’s body.
Sharing of needles or Accidental needle sticks: HBV easily spreads through
needles and syringes contaminated with infected blood. Hepatitis B is a concern for
health care workers and anyone else who meets human blood.
Mother to child: Pregnant women infected with HBV can pass the virus to their
babies during childbirth. However, the newborn can be vaccinated to avoid getting
infected in almost all cases.
The hepatitis B virus can survive outside the body for at least 7 days. During this
time, the virus can still cause infection if it enters the body of a person who is not
protected by the vaccine. The incubation period of the hepatitis B virus ranges from
30 to 180 days. The virus may be detected within 30 to 60 days after infection and
can persist and develop into chronic hepatitis B, especially when transmitted in
infancy or childhood.
Pathophysiology
The hepatitis B virus is constructed of an outer capsule containing HBsAg (hepatitis
B surface antigen), an inner core containing HBcAg (HBV core antigen), and
the HBeAg (hepatitis Be antigen). As the blood becomes exposed to HBV, the
body mounts a cell-mediated immune response by sending cytotoxic T cells and
natural killer cells to the virus and release inflammatory cytokines. The greater the
immune response, the greater the chance of fighting the virus. As the hepatocytes
are attacked and infiltrated by the HBV, they appear to have a ground glass look
under histological exam due to the HBsAg infiltrating the cell’s cytoplasm – this is
a differentiator for HBV versus other forms of hepatitis. Because hepatocytes are
continually proliferating, the virus is constantly being shed into the blood which
contributes to chronic infection.
The liver cell injury during HBV infection occurs per these 3 mechanisms: first,
due to a restricted cytotoxic T cell response directed at HBcAg/HBeAg on HBV
infected hepatocytes (immune mediated cells injury); second, possible mechanisms
is direct cytopathic effect of HBcAg expression in infected hepatocytes (cytopathic);
thirdly, possible mechanism is high level expression and inefficient secretion of
HBsAg.
The process by which the HBV virus replicates occurs in six (simplified) steps:
Attachment: The virus enters the cell using endocytosis by binding to a receptor
on the surface of the cell.
Penetration: The viral membrane merges with the host cell membrane then sends
its DNA and several proteins into the host cell’s cytoplasm.
Uncoating: Unlike other viruses, HBV uses RNA to replicate. HBV has partially
double stranded DNA that must be made into fully double stranded DNA first. Core
proteins separate from the partially double stranded viral DNA and make covalently
closed circular DNA (cccDNA). The cccDNA becomes the transcription template for
four mRNAs.
Replication: The largest of the four mRNA is used to make new copies of the
genetic material.
Assembly: The four mRNA are reprocessed, forming progeny virions that are
returned to the nucleus where they are recycled and make additional virions.
Release: DNA is synthesized via reverse transcriptase and new virus is sent into
the cytoplasm, then towards the cell membrane where it is released.
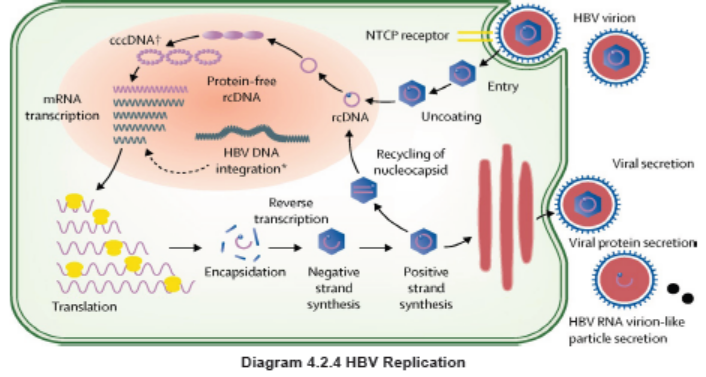
Signs and Symptoms
Most people do not experience any symptoms when newly infected with HBV.
However, some people have acute illness with symptoms that last several weeks,
including yellowing of the skin and eyes (jaundice), dark urine, extreme fatigue,
nausea, vomiting and abdominal pain. People with acute hepatitis can develop
acute liver failure, which can lead to death. Other Hepatitis B signs and symptoms
may include fever, joint pain, loss of appetite, nausea and vomiting, weakness and
fatigue, yellowing of your skin and the whites of your eyes (jaundice). The signs and
symptoms of hepatitis B range from mild to severe. They usually appear about one
to four months after you’ve been infected, although you could see them as early as
two weeks post-infection. Some people, usually young children, may not have any
symptoms.
Investigations
It is not possible on clinical grounds to differentiate hepatitis B from hepatitis caused
by other viral agents; hence laboratory confirmation of the diagnosis is essential.
Several blood tests are available to diagnose and monitor people with hepatitis B.
They can be used to distinguish acute and chronic infections.
The initial evaluation of patients with chronic HBV infection should include:
• A history and physical examination, emphasizing risk factors for coinfection
with hepatitis C virus (HCV), hepatitis delta virus (HDV), and/or HIV; use of
alcohol; family history of HBV infection and hepatocellular carcinoma (HCC);
and signs and symptoms of cirrhosis.
• Laboratory tests, including: a complete blood count with focus on
platelets, liver chemistry tests like aspartate aminotransferase [AST], alanine
aminotransferase [ALT], total bilirubin, alkaline phosphatase, albumin,
international normalized ratio (INR), and tests for HBV replication (HBeAg,
antibody to HBeAg [anti-HBe], HBV DNA). Testing for immunity to hepatitis A
virus (HAV) with HAV immunoglobulin G (IgG) antibody should be performed
in patients who are not known to be immune.
• Evaluation for other causes of liver disease (eg, hemochromatosis, HCV,
HDV) by testing for iron, total iron binding capacity, ferritin, and HCV antibody
in all patients. Other experts suggest one-time screening for HDV in all
patients with chronic hepatitis B.
• Screening for HIV infection in those who have not undergone routine screening,
and in those persons with ongoing risk factors for HIV (eg, injection drug use,
multiple sexual exposures, men who have sex with men).
• Screening for HCC if indicated.
• Screening for fibrosis using noninvasive tests (eg, vibration-controlled
transient elastography, serum fibrosis panel) or liver biopsy. Noninvasive
assessments of liver fibrosis, notably measurements of liver stiffness, are
increasingly used instead of liver biopsies; however, liver stiffness can be
influenced by inflammation as well as fibrosis, and therefore, liver stiffness
measurements may overestimate liver fibrosis in patients with a high ALT
(more than 100 units/L)
• Liver biopsy: Most patients will not need a liver biopsy.
Adequate medical diagnosis
Hepatitis B is a vaccine-preventable liver infection caused by the hepatitis B virus
(HBV).
Hepatitis B is spread when blood, semen, or other body fluids from a person
infected with the virus enters the body of someone who is not infected. This can
happen through sexual contact; sharing needles, syringes, or other drug-injection
equipment; or from mother to baby at birth. Not all people newly infected with HBV
have symptoms, but for those that do, symptoms can include fatigue, poor appetite,
stomach pain, nausea, and jaundice. For many people, hepatitis B is a short-term
illness. For others, it can become a long-term, chronic infection that can lead to
serious, even life-threatening health issues like cirrhosis or liver cancer. The best
way to prevent hepatitis B is to get vaccinated.
Treatment Plan
There is no specific treatment for acute hepatitis B. Therefore, care is aimed at
maintaining comfort and adequate nutritional balance, including replacement
of fluids lost from vomiting and diarrhea. Most important is the avoidance of
unnecessary medications. Acetaminophen, paracetamol, and medication against
vomiting should be avoided.
Chronic hepatitis B infection can be treated with medicines, including oral antiviral
agents. Treatment can slow the progression of cirrhosis, reduce incidence of liver
cancer, and improve long term survival.
In low-income settings, most people with liver cancer die within months of diagnosis.
In high-income countries, patient present to hospital earlier in the course of the
disease and have access to surgery and chemotherapy which can prolong life for
several months to a few years. Liver transplantation is sometimes used in people
with cirrhosis or liver cancer in high-income countries, with varying success.
The goals of antiviral therapy are suppression of HBV DNA, loss of HBeAg (in
patients who were initially HBeAg-positive), and loss of HBsAg. Antiviral agents for
chronic HBV include pegylated interferon (PegIFN) or nucleos(t)ide analogs (eg,
entecavir and tenofovir). WHO recommends the use of oral treatments (tenofovir
or entecavir) as the most potent drugs to suppress hepatitis B virus. Most people
who start hepatitis B treatment must continue it for life. Antiviral agents that are
treatment strategies for chronic HBV typically include interferons or nucleoside
analogs (entecavir and tenofovir):
1. Interferon: the main role of interferon is primarily treatment of young patients
with well compensated liver disease who do not wish to be on long-term
treatment. The advantages of interferon compared to nucleoside analogs are
its finite duration of treatment. Furthermore, interferon should not be used in
pregnant women and patients with decompensated disease or compensated
cirrhosis and portal hypertension.
2. Nucleoside analogs: Several nucleoside analog agents are available. The
available agents include: Entecavir, Tenofovir, Lamivudine, Adefovir and
Telbivudine.
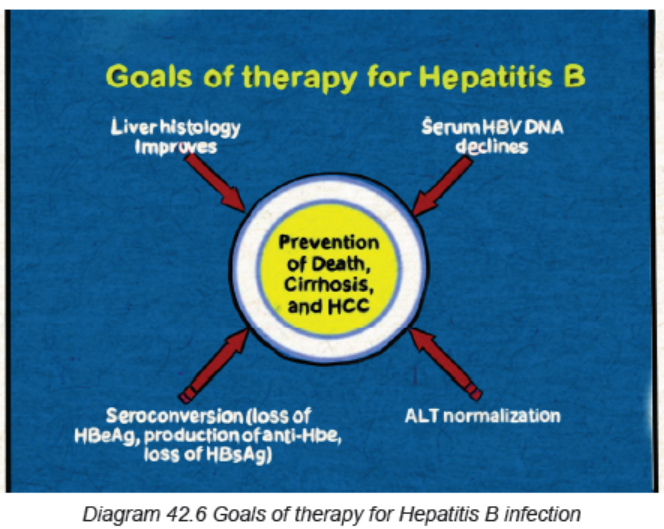
Prevention
A safe and effective vaccine that offers 98% to 100% protection against hepatitis B is
available. Preventing hepatitis B infection averts the development of complications
including chronic disease and liver cancer. The hepatitis B vaccine is typically given
as three or four injections over six months. The hepatitis B vaccine is recommended
for newborns, children and adolescents not vaccinated at birth, those who work or
live in a center for people who are developmentally disabled, people who live with
someone who has hepatitis B, health care workers, emergency workers and other
people who come into contact with blood, anyone who has a sexually transmitted
infection including HIV, Men who have sex with men, people who have multiple
sexual partners, sexual partners of someone who has hepatitis B, people who
inject illegal drugs or share needles and syringes and the health care professionals,
people with chronic liver disease, people with end-stage kidney disease, travelers
planning to go to an area of the world with a high hepatitis B infection rate.
Evolution and Complications
Most patients with hepatitis B recover fully, even if their signs and symptoms are
severe. Infants and children are more likely to develop a chronic (long-lasting)
hepatitis B infection. A vaccine can prevent hepatitis B, but there’s no cure if
you have the condition. If infected, taking certain precautions can help prevent
spreading the virus to others. The diagnosis of acute HBV infection is based upon
the detection of hepatitis B surface antigen (HBsAg) and IgM antibody to hepatitis B
core antigen (anti-HBc). For most patients, treatment is mainly supportive. Having
a chronic HBV infection can lead to serious complications such as:
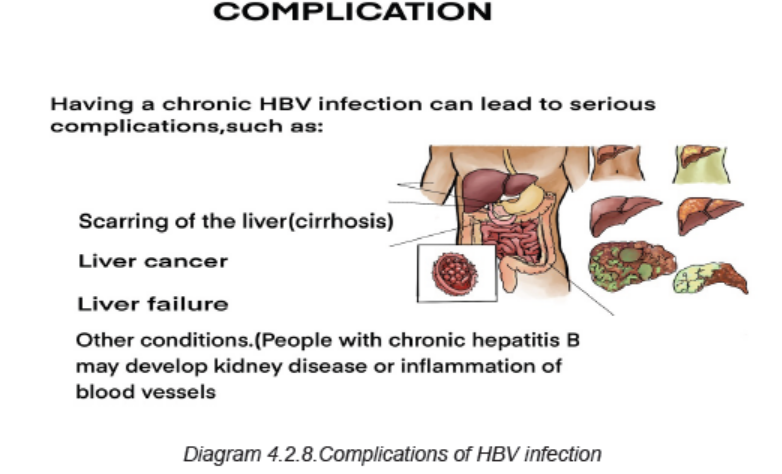
Self-assessment 4.2.6
1. What are different modes of HBV transmission?
2. Briefly described the pathogenesis of HBV infection.
3. What are different investigations used to the diagnosis of HBV?
4. What are the complications resulting from HBV infection?
4.2.7 GENITAL HERPES
Learning Activity 4.2.7
Carefulyl read the case study below and answer the following questions
Mrs B.A is 28 year old female patient who was presented at Rubona Health
Center with complaints fever, headache, pain during sex intercourse, itching and
sores in the vagina and anus area. The vital signs were the body temperature
of 38.5 degree Celius, blood pressure of 120/70 mm Hg, PR was 88bpm. Mrs
B.A was immediately referred to Rwamagana Hospital where she received an
antiviral drugs tha she doesn’t remember. After six months the same symptoms
reappeared and she revisited the Rwamagana Hospital for further management.
Arriving at hospital, the medical doctor did complete physical eamination and
found that she had sores at external genitalia and inside the vagina.
He decided to hospitalise her, gave her IV fluids 1.5 liters/24 hours, brufen 400mg
three times a day for 3 days, IV ceftriaxone 500mg TDS for 5 days, Acyclovir
200mg TDS for 7 days and local care of sores. He also requested the complete
blood count, vaginal and cervical swabs that the results were pending.
1. What are the abnormal signs and symptoms that the patient was presenting?
2. Basing on those signs and symptoms, what could be the medical problem
of this patient?
3. What are the investigations that have been requetsed to confirm the
medical condition of Mrs B.A?
4. What was included in the treatment plan of this case?
5. If not well treated, what will be the complications?
Genital herpes is a common sexually transmitted infection caused by the herpes
simplex virus type 1 or type 2 and manifests as either a primary or recurrent
infection, Sexual contact is the primary way that the virus spreads. After the initial
infection, the virus lies dormant in the body and can reactivate several times a year.
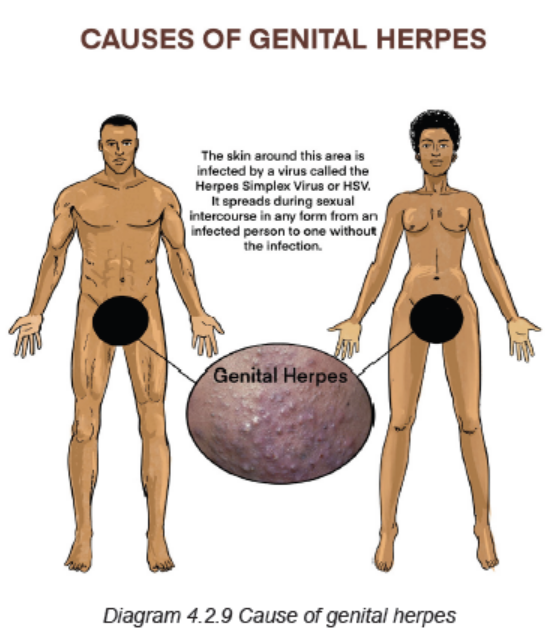
Two types of herpes simplex virus infections can cause genital herpes:
HSV-1: This is the type that usually causes cold sores or fever blisters around the
mouth. HSV-1 is often spread through skin-to-skin contact, though it can be spread
to the genital area during oral sex. Recurrences are much less frequent than they
are with HSV-2 infection.
HSV-2: This is the type that commonly causes genital herpes. The virus spreads
through sexual contact and skin-to-skin contact. HSV-2 is very common and highly
contagious, whether or not there is an open sore.
Because the virus dies quickly outside of the body, it’s nearly impossible to get the
infection through contact with toilets, towels or other objects used by an infected
person.
Risk factors for acquiring HSV-2 infection revolve around direct exposure to fluids
(i.e., semen, blood, saliva, etc.) from a seropositive individual containing viral
products most often during sexual intercourse. HSV-2 is mainly transmitted through
sexual intercourse, attributing to its predominant rise starting at puberty. Due to its
low stability outside the body, HSV can only remain infectious for days on moist
surfaces. Therefore, modes of transmission other than sexual intercourse are often
insignificant. Both primary and recurrent HSV infections in pregnant women can
lead to intrauterine transmission and resultant congenital HSV infection.
Pathophysiology
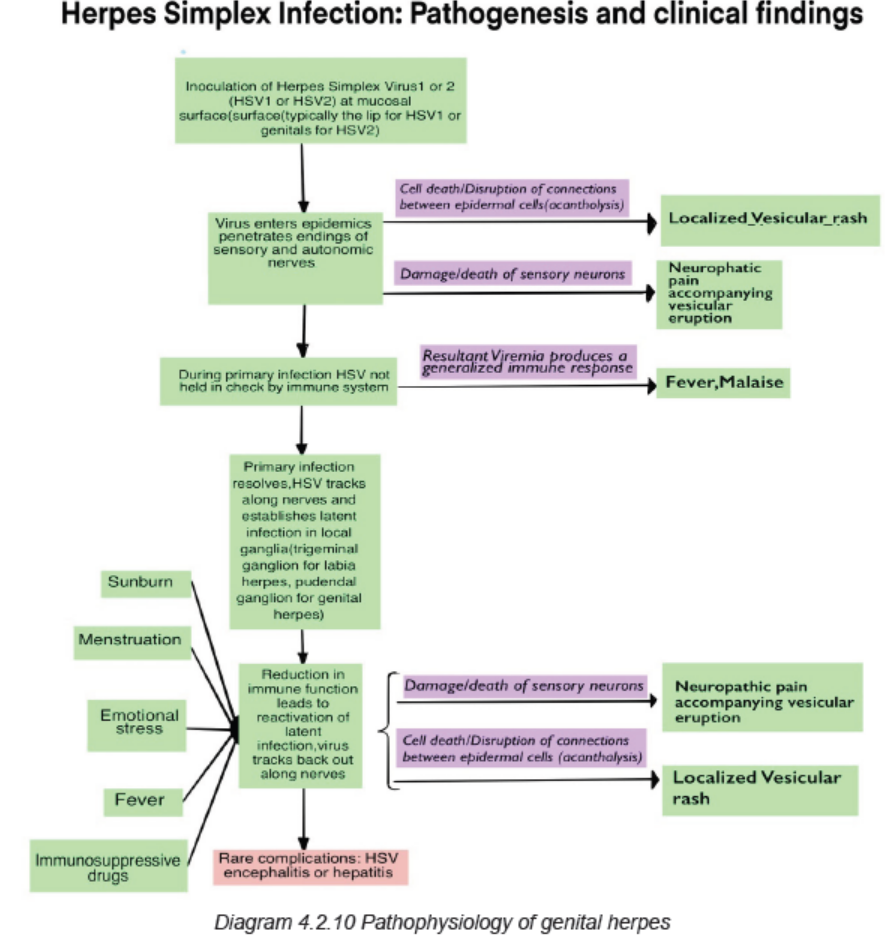
HSV-2 is transmitted through direct contact of sections in a seropositive individual
who is actively shedding the virus. The virus preferentially affects the skin and
mucous membranes with the virus invading epithelial cells on initial exposure
and ultimately replicating intracellularly at that site. After the initial exposure and
symptoms resolve, in 10 to 14 days, on average, the virus then lays dormant in
the periaxonal sheath of the sensory nerves of either the trigeminal, cervical,
lumbosacral, or autonomic ganglia. In these locations, the viral replication is often
controlled by the patient’s immune system and remains in a dormant state only to
later reactive later in life. When reactivation does occur, the virus travels through
the sensory nerves until it reaches the muco-cutaneous sites where replication then
takes place and leads to vesicular clusters at the dermatological site of that sensory
neuron.
Signs and Symptoms
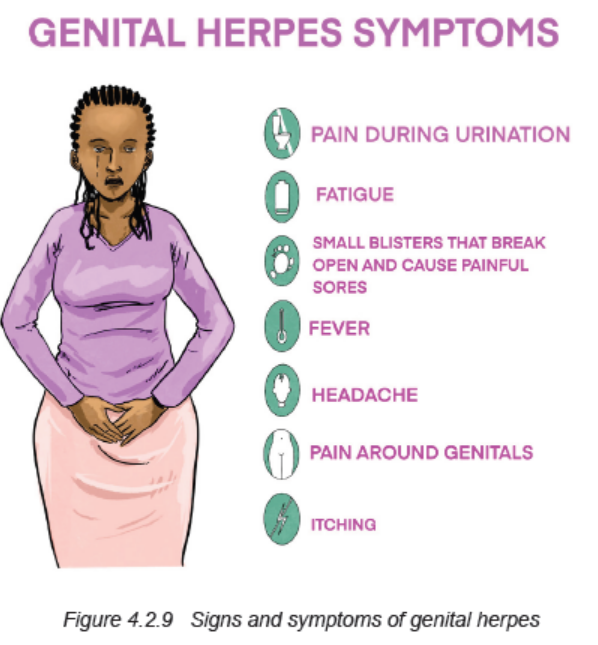
Most people infected with HSV do not know they have it because they don’t have
any specific signs or symptoms or because their signs and symptoms are so mild.
When present, symptoms may begin about two to 12 days after exposure to the
virus.
The signs and symptoms of genital herpes include:
Pain or itching: client may experience pain and tenderness in your genital area
until the infection clears.
Small red bumps or tiny white blisters or sores: These may appear a few days
to a few weeks after infection. Sores appear where the infection entered the body.
The infection can be spread by touching a sore and then rubbing or scratching
another area of the body, including the eyes.
Men and women can develop sores on the buttocks and thighs, anus, mouth and
urethra. Women can also develop sores in or on the vaginal area, external genitals,
and cervix. Men can also develop sores in or on the penis, and scrotum.
Ulcers: These may form when blisters rupture and ooze or bleed. Ulcers may make
very painful when urinating.
Scabs: Skin will crust over and form scabs as ulcers heal.
Genital herpes is different for each person. The signs and symptoms may recur,
off and on, for years. Some people experience numerous episodes each year. For
many people, however, the outbreaks are less frequent as time passes. During a
recurrence, shortly before sores appear, the client may feel burning, tingling and
itching where the infection first entered your body, pain in your lower back, buttocks
and legs. However, recurrences are generally less painful than the original outbreak,
and sores generally heal more quickly.
Investigations
Sometimes people mistake a pimple or ingrown hair for herpes. The doctor can
take a small sample from sores by using a swab test for laboratory examination.
If a client doesn’t have symptoms but think he/she might have herpes, the doctor
can order other test:
Viral culture: This test involves taking a tissue sample or scraping of the sores for
examination in the laboratory.
Polymerase chain reaction (PCR) test: PCR is used to copy the DNA from a
sample of the blood, tissue from a sore or spinal fluid. The DNA can then be tested
to establish the presence of HSV and determine which type of HSV the client has.
Blood test: This test analyzes a sample of the blood for the presence
of HSV antibodies to detect a past herpes infection.
Adequate medical diagnosis
Genital herpes is a common sexually transmitted infection marked by genital pain
and sores. It is caused by the herpes simplex virus, and this disease can affect
both men and women. Pain, itching and small sores appear first. They form ulcers
and scabs. After initial infection, genital herpes lies dormant in the body. Symptoms
can recur for years. Medication (mainly painkillers, antiviral drugs) can be used to
manage the condition.
Treatment plan
There’s no cure for genital herpes, but the treatment with antiviral medications may
help sores heal sooner during an initial outbreak, lessen the severity and duration
of symptoms in recurrent outbreaks, reduce the frequency of recurrence, minimize
the chance of transmitting the herpes virus to another. There are three major drugs
commonly used to treat genital herpes symptoms: acyclovir (zovirax), famciclovir
(famvir), and valacyclovir (valtrex). Moderate and minor cases are treated with
oral medications and severe cases may be treated with the intravenous (IV) drugs
seven to 10 days. Therapy should be initiated as early as possible following onset
of signs and symptoms.
Prevention
If the client is sexually active, there’s a chance to get herpes. He or she will make
it a lot less likely if he/she use a latex or polyurethane condom or dental dam every
time, for every activity. The dam or condom only protects the area it covers. If client
has herpes, he/she and his or her partner should get tested for STDs before sex.
To feel better during an outbreak, the client should wear loose-fitting clothes and
cotton underwear, avoid sun or heat that could cause more blisters, take a warm,
soothing bath, not use perfumed soaps or douches near the blisters.
Evolution and Complications
During vaginal birth, the herpes virus could spread to the baby, especially if the first
outbreak happens around the delivery time. The virus could give the baby rashes,
eye problems, or more serious issues. A caesarean section makes that less likely.
The doctor may also prescribe an anti-viral medicine starting at about 34 weeks to
avoid an outbreak around the due date.
Complications associated with genital herpes may include:
Other sexually transmitted infections: having genital sores increases the risk
of transmitting or contracting other sexually transmitted infections, including HIV/AIDS.
Newborn infection: babies born to infected mothers can be exposed to the virus
during the birthing process. This may result in brain damage, blindness or death forthe newborn.
Bladder problems: in some cases, the sores associated with genital herpes
can cause inflammation around the tube that delivers urine from the bladder to
the outside world (urethra). The swelling can close the urethra for several days,requiring the insertion of a catheter to drain the bladder.
Meningitis: in rare instances, HSV infection leads to inflammation of the membranesand cerebrospinal fluid surrounding the brain and spinal cord.
Rectal inflammation (proctitis): genital herpes can lead to inflammation of thelining of the rectum, particularly in men who have sex with men.
Pregnancy precautions: in case of pregnancy, the doctor may ask the woman
to be tested for genital Herpes and recommend her to start taking herpes antiviral
medications late in pregnancy to try to prevent an outbreak around the time of
delivery. If she is having a disease during the time she goes into labor, the doctorwill suggest a cesarean section to reduce the risk of passing the virus to the baby.
Self-assessment 4.2.7
1. What are the causes of genital Herpes?
2. Describe the pathophysiology of genital herpes.
3. What are the signs and symptoms of genital Herpes?
4. Which investigations should be requested to confirm the diagnosis of
genital Herpes?
5. What is the treatment plan of Genital Herpes?6. What are the complications of Genital Herpes?
4.2.8 TRICHOMONIASIS
Learning Activity 4.2.8
A 29-year-old man presented at Muhima DH complaining of oozing pus from
discrete areas over his glans penis with leaking of urine from those same
areas on micturition. This illness evolved over the preceding 7 months. He
was otherwise well. During the physical examination, the initial genitourinary
examination revealed a circumcised penis with two wart-like lesions and pus
oozing from the urethra. Prior to visit to Muhima Hospital, at Remera Health
center he was given cefixime 400 mg oral single dose, doxycycline 100 mg 12
hourly for 7 days, and metronidazole 2 g single dose over the preceding 7 months
with no improvement. At Muhima they did cytological examination of the purulent
discharge and found squamous epithelial cells and suppurative inflammation.
Organisms with features suggestive of Trichomonas vaginalis were observed.
The patient was treated with KMnO4 soaks for the lesions and tinidazole 2gr
single dose. He was sent back home and given the appointment to come after 1month for evaluation and possible biopsy of the wart lesions.
1. What were the signs and symptoms was the patient presenting?
2. What are the differential medical diagnoses that the patient was having?
3. What were the investigations requested to look for accurate medical
diagnosis?
4. What was involved into his treatment plan?5. If poorly treated, what will be the complications?
Trichomoniasis is a very common sexually transmitted disease (STD). It is caused
by infection with a protozoan parasite called Trichomonas vaginalis. Although
symptoms of the disease vary, most people who have the parasite cannot tell theyare infected.
Causes and risk factors
Trichomoniasis is caused by a one-celled protozoan “Trichomonas vaginalis “, a
type of tiny parasite that travels between people during sexual intercourse. The
incubation period between exposure and infection is unknown, but it’s thought to
range from four to 28 days.
The risk factors of trichomoniasis include having multiple sexual partners, a history
of other sexually transmitted infections, a previous episode of trichomoniasis, andsex without a condom.
Physiopathology
The parasite passes from an infected person to an uninfected person during sex.
In women, the most commonly infected part of the body is the lower genital tract
(vulva, vagina, cervix, or urethra). In men, the most commonly infected body part
is the inside of the penis (urethra). During sex, the parasite usually spreads from
a penis to a vagina, or from a vagina to a penis. It can also spread from a vagina
to another vagina. It is not common for the parasite to infect other body parts, like
the hands, mouth, or anus. It is unclear why some people with the infection get
symptoms while others do not. It probably depends on factors like a person’s age
and overall health. Infected people without symptoms can still pass the infection onto others.
Signs and symptoms
About 70% of infected people do not have any signs or symptoms. When
trichomoniasis does cause symptoms, they can range from mild irritation to severe
inflammation. Some people with symptoms get them within 5 to 28 days after
being infected. Others do not develop symptoms until much later. Symptoms can
come and go. Men with trichomoniasis may notice itching or irritation inside the
penis, burning after urination or ejaculation, discharge from the penis. Women with
trichomoniasis may notice itching, burning, redness or soreness of the genitals,
discomfort with urination, a change in their vaginal discharge (i.e., thin discharge or
increased volume) that can be clear, white, yellowish, or greenish with an unusual
fishy smell. Having trichomoniasis can make it feel unpleasant to have sex. Withouttreatment, the infection can last for months or even years.
Investigations
It is not possible to diagnose trichomoniasis based on symptoms alone. For both
men and women, the health care provider can examine the woman and get a
laboratory test to diagnose trichomoniasis. The healthcare provider may performthe following to diagnose trichomoniasis:
Complete physical exam (For women, this exam includes a pelvic exam)
Lab test: The healthcare provider examines a sample of the genital discharge
under a microscope to check for the cause of infection. The vaginal swab collected
may be sent to the lab for further testing if trichomonas are not seen under the
microscope. Trichomoniasis can be diagnosed by looking at a sample of vaginal
fluid for women or urine for men under a microscope. If the parasite can be
seen under the microscope, no further tests are needed. If this test isn’t conclusive,
tests called rapid antigen tests and nucleic acid amplification may be used.
Adequate medical diagnosis
Trichomoniasis also called trich, is a common sexual transmitted disease (STDs).
It is caused by a tiny one-celled parasite named Trichomonas vaginalis. Anyone
who’s sexually active can get it. It affects women more than men, older women
more than younger ones. People with trich often don’t have any symptoms, and
it doesn’t usually cause problems. But if you don’t get treatment, it raises your
chances of getting or spreading other STDs including HIV. Trichomoniasis can be
diagnosed by looking at a sample of vaginal fluid for women or urine for men under
a microscope. If the parasite can be seen under the microscope, no further tests
are needed. If this test isn’t conclusive, tests called rapid antigen tests and nucleic
acid amplification may be used. Without treatment, trich can last for months or even
years. It doesn’t go away on its own. The entire time the client is infected, he or shecan give the STD to his or her sexual partners.
Treatment plan
Trichomoniasis can be treated with medication prescribed by a doctor. These pills
are taken by mouth. It is safe for pregnant women to take this medication. People
who have been treated for trichomoniasis can get it again. About 1 in 5 people get
infected again within 3 months after receiving treatment. To avoid getting reinfected,all sex partners should get treated with antibiotics at the same time.
Oral anti-infective medications kill trich. The healthcare provider may prescribe
metronidazole (Flagyl®) or tinidazole (Tindamax®). It’s important to keep thefollowing points in mind while undergoing treatment:
• A single medication dose cures up to 95% of infected women. Men and
women may need to take the medication for five to seven days.
• Don’t drink alcohol for 24 hours after taking metronidazole or 72 hours after
taking tinidazole, because it can cause severe nausea and vomiting.
• Both sexual partners must be treated for trich.
• The client shouldn’t have sex for one week after finishing the medication to
give the drug time to kill off the infection and for symptoms to clear up. Having
sex too soon can lead to reinfection.
• The client should see the healthcare provider in three months to ensure you’re
no longer infected.
Wait to have sex again until everyone has been treated and any symptoms go away
(usually about a week). Get checked at 3 months to make sure that there is not a
new infection, or sooner if the symptoms come back before then.
Prevention
The only way to avoid STDs is not to have vaginal, anal, or oral sex.
If the client is a sexually active, he/she can do the following things to lower the
chances of getting trichomoniasis:
• Be in a long-term mutually monogamous relationship with a partner who has
been tested and has negative STD test results
• Use latex condoms the right way every time you have sex. This can lower the
chances of getting trichomoniasis.
• Get tested routinely for trichomoniasis and other STDs.
• Get treated if a client has trichomoniasis or other STDs.
• Tell the sexual partners if they have trich so they can get tested and treated.
• Limit the number of sexual partners.
Evolution and complications
Trichomoniasis can increase the risk of getting or spreading other sexually
transmitted infections. For example, trichomoniasis can cause genital inflammation
that makes it easier to get infected with HIV, or to pass the HIV virus on to a sex
partner. Untreated HIV can lead to AIDS. Women who have trich and HIV are
more likely to pass both diseases on to their partners. For this reason, the CDC
recommends that HIV-positive women get tested for trich at least once a year.
Pregnant women with trichomoniasis while pregnant or breastfeeding, it’s generally
safe to take anti-infective medication. Left untreated, trich increases the risk of
premature labor (childbirth before the 37th week of pregnancy), low birth weight(new-borns who weigh less than 2kg500), limit your number of sexual partners.
Self-assessment 4.2.8
1. What are the signs and symptoms of Trichomoniasis in man and woman?
2. Describe the pathophysiology of Trichomoniasis
3. What are the investigations that should be requested to confirm the medical
diagnosis of Trichomoniasis?
4. What is involved into the treatment plan of Trichomoniasis?
5. Explain the preventive measures for trichomoniasis.6. What are the complications of trichomoniasis?
4.3. END UNIT 4 ASSESSMENT
End unit assessment
1. Enumerate different commonest causes of UTI
2. Pathophysiological, describe how a UTI can lead to acute kidney injury.
3. What are the goals for UTI treatment?
4. What are general signs and symptoms of UTI.
5. Describe different complications of UTI.
6. Discuss different causes of urethritis.
7. Discuss different causes and risk factors of pyelonephritis.
8. Discuss different investigations helpful in diagnosis of pyelonephritis.
9. Different treatment options for pyelonephritis.
10. What are the investigations to be requested for diagnosing the prostatitis.
11. What are the investigations to request for diagnosing the syphilis?
12. What are different treatment options for gonorrhea?
13. Discuss different ways of HIV contamination.
14. Describe different preventive measures of HIV infection.
15. Discuss different complications related to HIV infection.
16. What are the risk factors of HPV infection?
17. Basing on the pathogenesis, discuss how HPV can lead do cervical cancer.
18. Describe different preventive measures of HPV.
19. What are different risk factors for development of Hepatitis B?
20. What are different investigations of diagnosing hepatitis B?
21. What are different treatment options for hepatitis B?
22. What are the complications of hepatitis B virus infection?23. What are different preventive measures of STDs?
UNIT 5 MEDICAL PATHOLOGIES OF ENDOCRINE SYSTEM
Key Unit Competences
To take an appropriate decision on management of common pathologies of
Endocrine system.
Introductory activity 5.0
Carefully observe the picture below and answer the following questions:
Figure 5.1 Glycemia measurement
1. How do you call the instrument shown at the picture below?
2. Can you interpret the readings/results from the instrument above?
3. Can you list some conditions that a person might present that will enablethe use of this equipment?
Endocrine glands include the hypothalamus, pituitary, thyroid, parathyroids,
adrenals, pancreas, ovaries, testes, and pineal gland. Exocrine glands are not part
of the endocrine system. They secrete their substances into ducts that then empty
into a body cavity or onto a surface. Hormones are chemical substances produced
in the body that control and regulate the activity of certain target cells or organs.
Many are produced in one part of the body and control and regulate the activity of
certain cells or organs in another part of the body. Endocrine glands produce andsecrete hormones that travel to affect their specific target tissues.
5.1 DIABETES MELLITUS
Learning Activity 5.1
Carefully read this below situation and answer the following questions:
A 54 year old female visited NCD clinic with the complaints of excessive urination,
sudden weight loss, blurred vision, increased thirst, fatigue and excessive
sweating. She was experiencing these conditions from last one month. From the
past medical history, she was also suffering from hypertension from last 3 years
under treatment (Atenolol 50mg OD per day and Lasix 40mg BID per day from
last 3 years. From the general examination, weight: 70kg and height: 152cm
BMI: 30.5kg/m2. She also had limited physical activities as she always stayed
at home.
From all observations, the NCD Medical Doctor recommended to monitor the
patient’s blood glucose level. At that time patient’s random blood glucose level
was 245mg/dl which was beyond the normal range of the random blood glucose
level (70-110mg/dl). The NCD Medical Doctor recommended also to patient
to monitor the patient fasting glucose level and then to check HbA1C Level
after about every 3rd month in the following visits. The NCD Medical Doctor
prescribed the drug (metformin 500mg BID per day) that should be taken about
5 -10 minutes before the meal and in combination with other drugs she has been
taking.
The patient was also advised that instead of eating a lot at 3 meals, divide total
intake in 5 meals. She was also suggested to avoid sugar intake, do exercise
and walk to reduce body weight, take high fiber diet and less intake of fats and
carbohydrates. The patient was given the appointments to visit the NCD clinic
on monthly basis to monitor the trends of blood sugar levels and also the other
symptoms that might arise from existing condition.
1. What are the abnormal signs and symptoms that the patient was presenting?
2. What do you think is the medical condition was she presenting in addition
to hypertension?
3. What are the investigations requested to diagnose that medical condition?
4. What was included into her plan of the management?5. If this condition is not well managed, what are the possible complications?
The pancreas is a long, tapered, lobular, soft gland located behind the stomach and
anterior to the first and second lumbar vertebrae. The pancreas has both exocrine
and endocrine functions. The hormone-secreting portion of the pancreas is referred
to as the islets of Langerhans. The islets account for less than 2% of the gland
and consist of four types of hormone-secreting cells: α, β, delta, and F cells. α
Cells produce and secrete the hormone glucagon. Insulin and amylin are produced
and secreted by β cells. Somatostatin is produced and secreted by the delta cells.
Pancreatic polypeptide (PP) is secreted by the F
(or PP) cells.
Glucagon is synthesized and released from pancreatic α cells and the gut in response
to low levels of blood glucose, protein ingestion, and exercise. Glucagon increases
blood glucose by stimulating glycogenolysis, gluconeogenesis, and ketogenesis.
Glucagon and insulin function in a reciprocal manner to maintain normal blood
glucose levels. In the fasting state, hormones such as catecholamines, cortisol,
and glucagon break down stored complex fuels (catabolism) to provide glucose as
fuel for energy.
Insulin is the principal regulator of metabolism and storage of ingested
carbohydrates, fats, and proteins. Insulin facilitates glucose transport across
cell membranes in most tissues. However, the brain, nerves, lens of the eye,
hepatocytes, erythrocytes, and cells in the intestinal mucosa and kidney tubules
are not dependent on insulin for glucose uptake. An increased blood glucose level
is the major stimulus for insulin synthesis and secretion. Other stimuli to insulin
secretion are increased amino acid levels and vagal stimulation. Insulin secretion is
usually inhibited by low blood glucose levels, glucagon, somatostatin, hypokalemia,
and catecholamines. A major effect of insulin on glucose metabolism occurs in
the liver, where the hormone enhances glucose incorporation into glycogen and
triglycerides by altering enzymatic activity and inhibiting gluconeogenesis. After a
meal, insulin is responsible for the storage of nutrients (anabolism). Another major
effect occurs in peripheral tissues, where insulin facilitates glucose transport into
cells, transport of amino acids across muscle membranes and their synthesis into
protein, and transport of triglycerides into adipose tissue.
The term diabetes mellitus describes diseases of abnormal carbohydrate metabolism
that are characterized by hyperglycemia. It is associated with a relative or absolute
impairment in insulin secretion, along with varying degrees of peripheral resistance
to the action of insulin.
Types of diabetes mellitus and their causes: the underlying cause of diabetesvaries by type:
A. Prediabetes:
Prediabetes is a condition in which blood glucose levels are too high to be considered
normal but not high enough to be labeled diabetes. People have prediabetes if their
fasting blood glucose level is between 100 mg/dL (5.6 mmol/L) and 125 mg/dL
(6.9 mmol/L) or if their blood glucose level 2 hours after a glucose tolerance test
is between 140 mg/dL (7.8 mmol/L) and 199 mg/dL (11.0 mmol/L). Prediabetes
carries a higher risk of future diabetes as well as heart disease. Decreasing body
weight by 5 to 10% through diet and exercise can significantly reduce the risk of
developing future diabetes.
B. Type 1 diabetes mellitus:
In type 1 diabetes mellitus (formerly called insulin-dependent diabetes or
juvenile-onset diabetes), the body’s immune system attacks the insulin-producing
cells of the pancreas, and more than 90% of them are permanently destroyed. The
pancreas, therefore, produces little or no insulin. Most people who have type 1
diabetes develop the disease before age 30, although it can develop later in life.
Some environmental factors like viral infection or nutritional factor during childhood
or early adulthood cause the immune system to destroy the insulin-producing cells
of the pancreas. A genetic predisposition makes some people more susceptible to
an environmental factor.
C. Type 2 diabetes mellitus:
In type 2 diabetes mellitus (formerly called non–insulin-dependent diabetes or
adult-onset diabetes), the pancreas often continues to produce insulin, sometimes
even at higher than normal levels, especially early in the disease. However, the
body develops resistance to the effects of insulin, so there is not enough insulin to
meet the body’s needs. As type 2 diabetes progresses, the insulin producing ability
of the pancreas decreases.
Obesity is the chief risk factor for developing type 2 diabetes, and 80 to
90% of people with this disorder are overweight or obese. Because obesity
causes insulin resistance, obese people need very large amounts of insulin to
maintain normal blood glucose levels.
Certain disorders and drugs can affect the way the body uses insulin and can lead
to type 2 diabetes mellitus.
Examples of common states (conditions) that result in impaired insulin use are
high levels of corticosteroids (most commonly due to use of corticosteroid drugs or
Cushing syndrome (a disorder that occurs when your body makes too much of the
hormone cortisol over a long period of time), Pregnancy. Diabetes also may occur
in people with excess production of growth hormone (acromegaly) and in people
with certain hormone-secreting tumors. Severe or recurring pancreatitis and otherdisorders that directly damage the pancreas can lead to diabetes
D. Gestational diabetes:
Gestational diabetes is diabetes diagnosed for the first time during pregnancy
(gestation). Like other types of diabetes, gestational diabetes affects how your cells
use sugar (glucose). Gestational diabetes causes high blood sugar that can affect
your pregnancy and your baby’s health. For a person who has gestational diabetes
during pregnancy, generally the blood sugar returns to its usual level soon after
delivery. But the person has a higher risk of getting type 2 diabetes mellitus.
Risk factors and Pathophysiology
The factors that increase the risk of developing diabetes mellitus differ dependingon the type of diabetes.
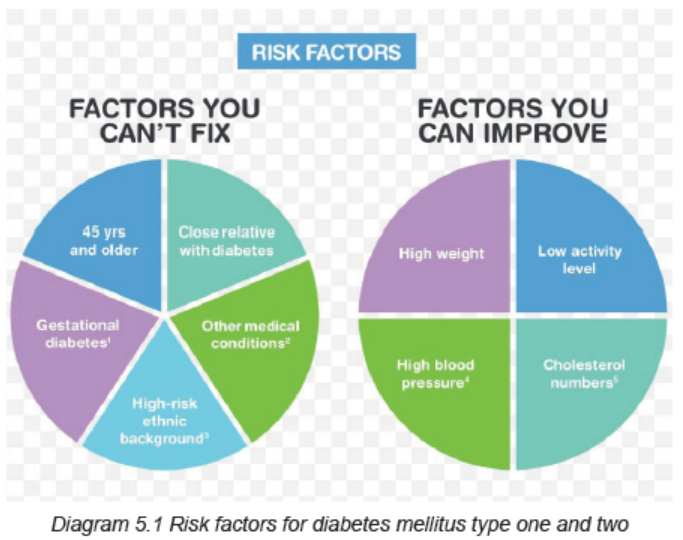
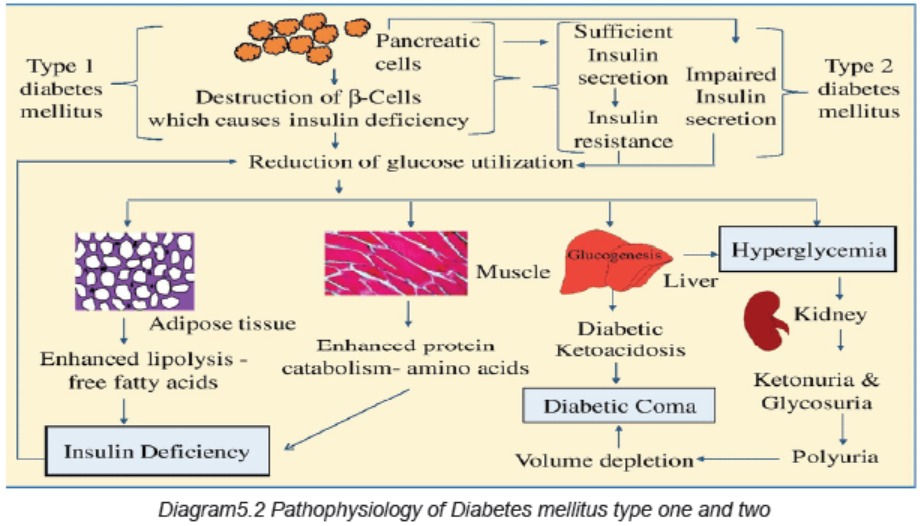
Signs and symptoms:
Diabetes signs and symptoms vary depending on how much the blood sugar iselevated.
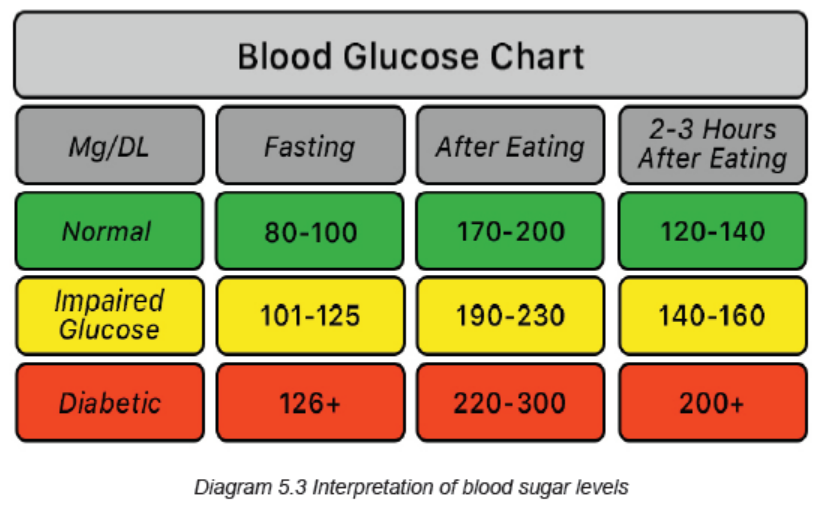
Some people, especially those with prediabetes or type 2 diabetes, may sometimes
not experience symptoms. In type 1 diabetes, symptoms tend to come on quickly
and be more severe.
The signs and symptoms of type 1 diabetes and type 2 diabetes are: increased
thirst (polydipsia), frequent urination (polyuria), extreme hunger (polyphagia),
unexplained weight loss, presence of ketones (are a byproduct of the breakdown
of muscle and fat that happens when there’s not enough available insulin) in the
urine, fatigue, irritability, blurred vision, numbness or tingling into the hands or feet,
slow-healing sores, frequent infections such as gums or skin infections and vaginal
infections. Patient with type 1 diabetes might also present nausea, vomiting andstomach pains.
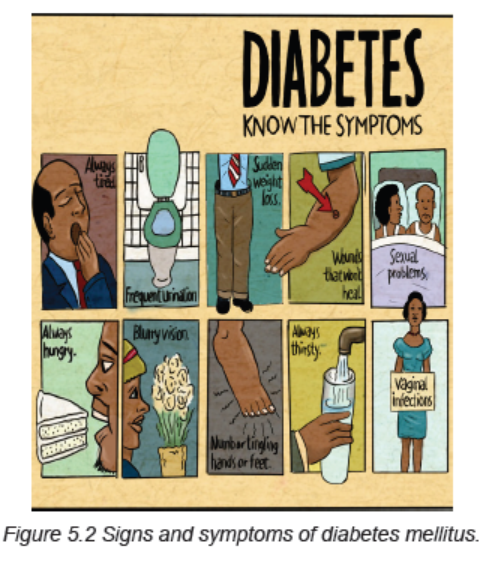
Investigations
Symptomatic hyperglycemia: The diagnosis of diabetes mellitus is easily
established when a patient presents with classic symptoms of hyperglycemia (thirst,
polyuria, weight loss, blurry vision) and has a random blood glucose value of 200
mg/dL (11.1 mmol/L) or higher.
Most patients with type 1 diabetes are symptomatic and have plasma glucose
concentrations/random blood glucose of ≥200 mg/dL. Some patients with type 2
diabetes also present with symptomatic hyperglycemia and blood glucose ≥200
mg/dL.
Asymptomatic hyperglycemia: The diagnosis of diabetes in an asymptomatic
individual (generally type 2 diabetes) can be established with any of the followingcriteria:
• Fasting plasma glucose (FPG) values ≥126 mg/dL (7.0 mmol/L). Fasting is
defined as no caloric intake for at least eight hours.
• Two-hour plasma glucose values of ≥200 mg/dL (11.1 mmol/L)
• A1C (hemoglobin A1C, HbA1C, glycated hemoglobin, and glycosylatedhemoglobin test) values ≥6.5 percent (48 mmol/mol).
In the absence of symptomatic hyperglycemia, the diagnosis of diabetes must be
confirmed by repeated measurement, repeating the same test for confirmation.
However, if two different tests (eg, FPG and A1C) are available and are concordant
for the diagnosis of diabetes, additional testing is not needed.
Urine analysis must also be done for glucosuria, ketonuria. Other investigations
include: full blood count, proteins into urine, blood urea and electrolytes, liverbiochemistry, lipidemia and cholesterol levels, etc.
Adequate medical diagnosis
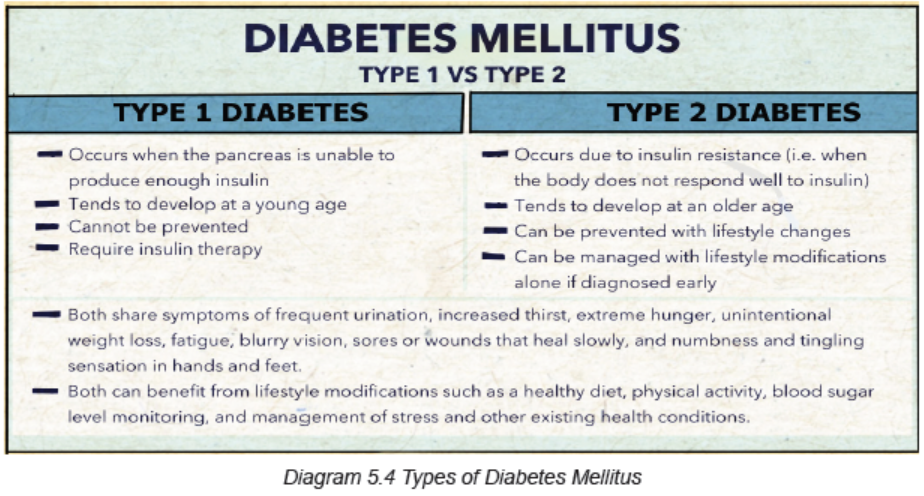
Plan of management of each type of diabetes mellitus
The goal of diabetes management is to keep blood glucose levels as close to normal
as safely possible. Since diabetes may greatly increase risk for heart disease and
peripheral artery disease, measures to control blood pressure and cholesterol
levels are an essential part of diabetes treatment as well.
People with diabetes must take responsibility for their day-to-day care. This includes
monitoring blood glucose levels, dietary management, maintaining physical
activity, keeping weight and stress under control, monitoring and adhering to oral
medications or insulin use via injections. To help patients achieve this, the health
care facility must offer self-management educational programs that emphasize
individualized diabetes care.
The plan of management of diabetes mellitus includes:A. Dietary management and physical activity
Modifying eating habits and increasing physical activity are typically the first steps
toward reducing blood sugar levels. The benefits of exercises include to improve
insulin sensitivity, to lower blood glucose during and after exercise, to improve lipid
profile, may improve some hypertension, to assist with weight loss, to promotecardiovascular fitness, to increase strength and flexibility, to improve sense of wellbeing.
The patient must also know some risks of exercises: precipitation or exacerbation
of cardiovascular disease, angina, dysrrhythmias, sudden death, hypoglycemia if
taking insulin or oral agents, late onset post-exercise hypoglycemia, hypoglycemia
after very strenuous exercise, worsening of long-term complications such as
proliferative retinopathy, peripheral neuropathy. The patient must also know that
taking some glucose before an exercise may be necessary to minimize the risk forhypoglycemia. Blood glucose check up before and after exercise is necessary.
B. Insulin Therapy
People with type 1 diabetes require multiple insulin injections each day to maintain
safe insulin levels. Insulin is often required to treat type 2 diabetes too. The pump
is about the size of a pager and is usually worn on your belt. Insulin is delivered
through a small syringe that contains the small and thin needle that is placed under
the skin (usually in the abdomen) during injection. There are four major types ofinsulin: rapid-acting, short-acting, intermediate-acting and long-acting.
C. Oral Medications/Hypoglycemia
Sometimes blood sugar levels remain high in people with type 2 diabetes even
though they eat in a healthy manner and exercise. When this happens, medications
taken in pill form may be prescribed. The medications work in several different ways.
These include improve the effectiveness of the body’s natural insulin, reduce blood
sugar production, increase insulin production and inhibit blood sugar absorption.Oral diabetes medications are sometimes taken in combination with insulin.
Oral hypoglycemia agents in type 2 diabetes in early stages are e.g biguanides such
as Metformin reduces hepatic glucose production, Thiazolidinediones/glitazones
reduce insulin resistance, alpha-Glucosidase inhibitors such as miglitol reducepostprandial hyperglycemia by delaying glucose absorption.
D. Monitor glycemia before meal and before bedtime
C. Education to diabetic patients: Education about signs and symptoms of
hypoglycemia, During any journey, the patient should carry the drugs on him/her.
The diabetic card is also necessary, and the patient should not forget to carry some
foods or fluid containing sugar to take in case of hypoglycemia,
Education on self-injection: number of injections per day, way of administration (S/C
route) and site of injection, General hygiene specifically feet hygiene, Educate the
patient and the family the importance of insulin therapy and some complications
of diabetes if insulin is not taken carefully, Don’t forget the importance of diabetic
regimen, Advise the patient to join diabetic associations (it will help her or him
to have medication on low cost, and he/she will learn more about the diabetes
mellitus). FOOT CARE is also very important due to these three major factors that
interact in foot problems in diabetes: neuropathy, ischemia, and sepsis. Therefore
patient must also be educated to never soak feet, wash feet daily and dry them well,
playing attention to the area between the toes, inspect the feet daily (color changes,
swelling, cuts, cracks in the skin, redness, blisters, temperature changes), never
walk barefoot. Always wear shoes or slippers, wear well-fitting shoes, after bathing,
when toenails are soft, cut nails straight across and don’t cut into the corners, if feet
are dry, apply lotion or cream; don’t put lotion between the toes, consult a podiatristfor any problem of the feet.
Evolution and complications of type 1 and 2 diabetes mellitus
Diabetes mellitus is a chronic disease and does not have a cure, except for the case
of gestational diabetes which usually disappears after childbirth. Among diabetes
mellitus complications, there are Acute that develop suddenly and Long-term
complications of diabetes that develop gradually. The longer you have diabetes and
the less controlled your blood sugar the higher the risk of complications. Eventually,diabetes complications may be disabling or even life-threatening.
Acute complications include diabetic ketoacidosis (DKA), Hperglycemic
Hyperosmolar nonketonic coma (HHNC/HHS), Hypoglycemia, the somogyi effect
(happens when patient takes insulin before bed and wake up with high blood
sugar levels; according to the theory of the Somogyi effect, when insulin lowers the
blood sugar too much, it can trigger a release of hormones that send the blood sugar
levels into a rebound high), the dawn phenomenon (early morning hyperglycemiadue to the liberation of growth hormone during nighttime).
Possible long-term complications include:
• Cardiovascular disease: diabetes dramatically increases the risk of various
cardiovascular problems, including coronary artery disease with chest pain
(angina), heart attack, stroke and narrowing of arteries (atherosclerosis).
• Nerve damage (neuropathy): excess sugar can injure the walls of the tiny
blood vessels (capillaries) that nourish the nerves, especially in the legs. This
can cause tingling, numbness, burning or pain that usually begins at the tips
of the toes or fingers and gradually spreads upward. Left untreated, it can
lead to loss of all sense of feeling in the affected limbs. Damage to the nerves
related to digestion can cause problems with nausea, vomiting, diarrhea orconstipation. For men, it may lead to erectile dysfunction
• Kidney damage (nephropathy): the kidneys contain millions of tiny blood
vessel clusters (glomeruli) that filter waste from the blood. Diabetes can
damage this delicate filtering system. Severe damage can lead to kidney
failure or irreversible end-stage kidney disease, which may require dialysis
or a kidney transplant.
• Eye damage (retinopathy): diabetes can damage the blood vessels of the
retina (diabetic retinopathy), potentially leading to blindness. Diabetes also
increases the risk of other serious vision conditions, such as cataracts and
glaucoma.
• Foot damage: nerve damage in the feet or poor blood flow to the feet increases
the risk of various foot complications. Left untreated, cuts and blisters can
develop serious infections, which often heal poorly. These infections may
ultimately require toe, foot or leg amputation.
• Skin conditions: diabetes may leave a person to more susceptible to skin
problems, including bacterial and fungal infections.
• Hearing impairment: hearing problems are more common in people with
diabetes.
• Alzheimer›s disease: type 2 diabetes may increase the risk of dementia,
such as Alzheimer›s disease. The poorer the blood sugar control, the greater
the risk appears to be.
• Depression: depression symptoms are common in people with type 1 and
type 2 diabetes. Depression can affect diabetes self-management leading topoor outcomes.
Complications of gestational diabetes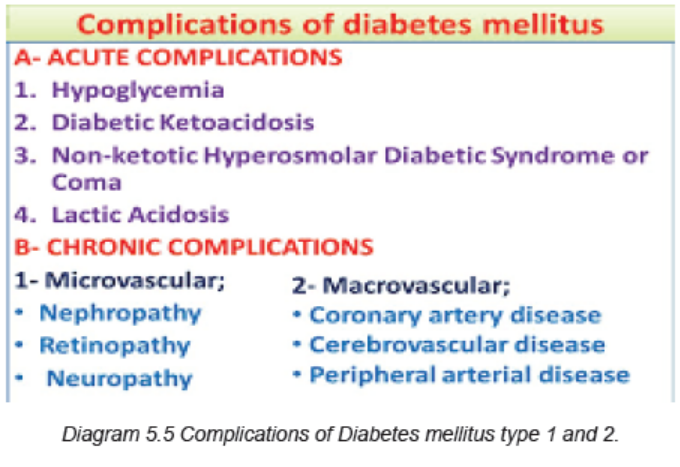
Most women who have gestational diabetes deliver healthy babies. However,
untreated or uncontrolled blood sugar levels can cause problems for the mother
and/or the baby.
Complications to the baby can occur as a result of gestational diabetes, including:
– Excess growth: Extra glucose can cross the placenta, which triggers the
baby›s pancreas to make extra insulin. This can cause the baby to grow too
large (macrosomia). Very large babies are more likely to require a C-section
birth.
– Low blood sugar: Sometimes babies of mothers with gestational diabetes
develop low blood sugar (hypoglycemia) shortly after birth because their own
insulin production is high. Prompt feedings and sometimes an intravenous
glucose solution can return the baby›s blood sugar level to normal.
– Type 2 diabetes later in life: Babies of mothers who have gestational
diabetes have a higher risk of developing obesity and type 2 diabetes later
in life.
– Death: Untreated gestational diabetes can result in a baby›s death either
before or shortly after birth.
– Complications to the mother also can occur as a result of gestational
diabetes, including:
– Preeclampsia: This condition is characterized by high blood pressure, excess
protein in the urine, and swelling in the legs and feet. Preeclampsia can lead
to serious or even life-threatening complications for both mother and baby.
– Subsequent gestational diabetes. Once a pregnant women had gestational
diabetes in one pregnancy, she will be more likely to have it again with the
next pregnancy. She is also more likely to develop diabetes typically type 2
diabetes — as she gets older.
Very serious and Acute Complications of Diabetes Mellitus (DKA and HHS)
A. DIABETIC KETOACIDOSIS (DKA)
DKA results from relative or absolute insulin deficiency (lack of insulin, insulin
omission). The decreased ratio of insulin to glucagon promotes gluconeogenesis,
glycogenolysis, and ketone body formation in the liver. Ketosis results from a
marked increase in free fatty acid release from adipocytes, with a resulting shift
toward ketone body synthesis in the liver. Reduced insulin levels, in combination
with elevations in catecholamines and growth hormone, increase lipolysis and therelease of free fatty acids. DKA is more present in type 1 diabetes mellitus.
Causes of DKA
• DKA is the initial manifestation of diabetes in 20% of adults and 30–40% of
children with type 1 diabetes.
• In patients with established diabetes, causes of DKA include:
• Infection (30%-50%)
Most common infections urinary tract infection and pneumonia
• Noncompliance with insulin• Psychological stress
Clinical manifestations include: Hyperglycemia, Ketosis: ketonuria, serum ketone
(ketonemia), ketone smelling (fruity odor), Metabolic acidosis, Hyperlipoproteinemia,
Nausea, Signs of acidosis (Kussmaul respiration, acetone breath), Signs of volume
depletion/ dehydration, Polyuria, polydipsia, polyphagia, weight loss, Fever due to
underlying infection is common(if present), Gastrointestinal signs (abdominal pain,
vomiting), Neurological signs (hemiparesis and seizures) related to metabolicacidosis.
Diagnosis of DKA
• Serum glucose level > 250 mg/dL
• Serum bicarbonate < 18 mg/dL
• Serum pH < 7.30
• Presence anion gap
• History and physical examination,
• Blood studies including immediate blood glucose, complete blood count, pH,
ketones, electrolytes, blood urea nitrogen, arterial or venous blood gases.• Urinalysis, including specific gravity, glucose, acetone
Management of DKA:
1. Confirm diagnosis (↑plasma glucose, positive serum ketones, metabolic
acidosis).
2. Admit to hospital (unconsciousness, PH < 7 )
3. Assess: serum electrolytes (K+, Na+, Mg2+, Cl-, bicarbonate, phosphate),
acid-base status (pH, HCO3-, PCO2), renal function (creatinine, urine output)
4. Replace fluids: 2–3 L of 0.9% saline over first 1–3 h (10–15 mL/kg per hour);
5. Administer short-acting insulin: IV (0.1 unit/kg/hour) or IM/ SC (0.3 units/
kg). Insulin increases peripheral glucose utilization and decreases hepatic
glucose production. If initial serum potassium is < 3.3 mmol/L (3.3 meq/L), donot administer insulin until the potassium is corrected to > 3.3 mmol/L.
6. Give medication to correct hyperkalemia (urgent treatment of hyperkalemia
includes stabilizing the myocardium to protect against arrhythmias and
shifting potassium from the vascular space into the cells. Intravenous calcium
(eg: calcium gluconate) is administered to stabilize the myocardium; it lowers
the threshold potential, thus counteracting the toxic effect of high potassium.
Other medications like sodium polystyrene sulfonate (Kaayexalate) works by
helping the body get rid of extra potassium through feces, etc.
7. Electrolyte replacement
8. Assessment of mental status, Assessment of blood glucose levels, Assessment
of blood and urine for ketones, Assessment of cardiovascular and respiratory
status and ECG monitoring, Assess patient: What precipitated the episode
(noncompliance, infection, trauma, alcohol?
9. Monitoring and recording of intake and output
10. Central venous pressure monitoring (if indicated)
11. Measure capillary glucose every 1–2 h; measure electrolytes (especially K+,
bicarbonate, phosphate) and anion gap every 4 h for first 24 h.
12. Initiate appropriate workup for precipitating event (cultures, Chest X-Ray,ECG).
The complications of diabetic ketoacidosis
DKA can cause complications such as low levels of potassium (hypokalemia) that
can cause severe problems like muscle weakness and heart rhythm problems
which can cause death), swelling inside the brain (cerebral edema), fluid inside the
lungs (pulmonary edema), damage to the kidney or other organs from the fluid loss.All these can lead to sudden death.
B. HYPERGLYCEMIC HYPEROSMOLAR NONKETONIC COMA/STATUS(HHCN/HHS)
This is a complication of type 2 diabetes mellitus especially for the elderly people.
Hyperglycemia induces an osmotic diuresis that leads to intravascular volume
depletion, which is exacerbated by inadequate fluid replacement (impaired patient’s
perception of thirst due to underlying cerebrovascular disease). The polyuriadisappears early because of the severe dehydration.
Clinical manifestations
• Severe dehydration (fluid deficit of 8-9 L)
• Severe hyperglycemia (plasma glucose may be >55.5 mmol/L (1000 mg/dL)• Hyperosmolarity (>350 mosmol/L)
Management
• IV replacement with hypotonic solutions (0.45% normal saline)
• IV insulin is not needed, give insulin subcutaneously
Possible complications of untreated HHS are shock, blood clot formation, brain
swelling (cerebral edema) or increased blood acid level (lactic acidosis).
C. HYPOGLYCEMIA
The hypoglycemia in diabetic person is due to insulin therapy or glucose lowering
agents:
• Insulin overdosage
• Glucose lowering agents overdosage
• Inconsistent carbohydrates intake (no glucose intake before insulin injection)
• Alcohol consumption
• Uncompensated exercise• Patient with end-stage renal or liver failure are at risk for hypoglycemia
Signs and symptoms
Adrenergic symptoms (hypoglycemia causes the liberation of chathecholamines
particulary adrenalin as compensatory mechanism): pallor, diaphoresis, tachycardia,
palpitation, nervousness, irritability, sensation of coldness, weakness, trembling,
hunger.
Neuroglycopenic symptoms: the low glucose in nervous system causes
headache, mental confusion, fatigue, incoherent speech, coma, diplopia, emotionallability, and convulsion.
Self-assessment 5.1
Read the clinical case scenario below and answer the followingquestions:
A 27year old man was brought to the emergency reception reporting severe
weakness, dizziness, and sleepiness all the time. Upon questioning, he reported
increased and not resolving thirst, and the repeated need to urinate. Although
he ate all of his rations as well as whatever he could get from his family, he had
lost 7 kgs during recent 9 months. On the previous day before his consult, he
complained of vague abdominal pain, which was worse on the morning and had
vomited once. During the physical examination, he was oriented but tachypneic
(pulse rate of 138 beats per minute) and his blood pressure was 90/60 mm
Hg. He appeared pale, dehydrated with dry mucous membranes, and poor
skin turgor. His respiratory rate was 36 cycles per minute with deep, laborious
breathing. After admission, the laboratory investigations showed blood glucose
levels of 560 mg/dl, sodium 154, potassium 6.5, pH 7.10, bicarbonate 10 mM/liter,
chloride 90, BUN 38 mg/dl, creatinine 2.5 mg/dl. (Normal values: glucose: 70-
110 mg/dl; Na = 135-145; K, 3.5-5.5; Cl, 98-108; CO2, 20-32 [all in mM/l]; BUN,
7-22mg/dl; creatinine, 0.7-1.5 mg/dl). A urine sample was 4+ for glucose and
had “large” acetone. Glycated hemoglobin (HbA1c) was 14% (normal=4-6.2%).
He was treated with insulin and normal saline I.V. initially and by the 4th hour
of treatment, potassium chloride was added to the IV at a rate of 15 mEq/hour.
Sixteen hours later, he was active, alert, well hydrated and cheerful, indicating
he felt extremely well. He requested that his IV be discontinued. His physician
decided to switch his insulin to subcutaneous injections and to start a liquid diet.
He was later put on a diabetes maintenance diet and treated with one injection of
Human Lente insulin in the morning. Although his blood sugars the next morning
were 100-140 mg/dl, he had frequent episodes of hypoglycemia during the day,
he was put on 3 injections of regular insulin/day, and a bedtime intermediate
duration (Lente) insulin.
1. Basing on the case presented above, what was the medical condition that
the patient was presenting?
2. What are the signs and symptoms that guided you in thinking about that
medical diagnosis?
3. What are different investigations requested to confirm that medical
condition?
4. What are all possible treatment options are available to that medical
condition?5. If it is not properly managed, what are the possible complications?
5.2 END UNIT 5 ASSESSMENT
End unit assessment
1. Explain how the pancreas serves both endocrine and exocrine functions.
2. By definition, differentiate diabetes mellitus type one and two
3. Give 5 risk factors of type one and two of diabetes mellitus.
4. What are the general signs and symptoms of diabetes mellitus?
5. What are the investigations that are relevant into the diagnosis of diabetes
mellitus?
6. Discuss different management principles of diabetes mellitus.
7. Discuss how the diabetes mellitus can lead to kidney, eye and foot
problems.
8. Basing on the causes and signs and symptoms, differentiate the DKA and
HHS.
9. What are different management principles of DKA?
10. In addition to promoting the transport of glucose from the blood into the
cell, what does insulin do?
a. Enhances the breakdown of adipose tissue for energy
b. Stimulates hepatic glycogenolysis and gluconeogenesis
c. Prevents the transport of triglycerides into adipose tissue
d. Accelerates the transport of amino acids into cells and their synthesisinto protein
11. Why are the hormones cortisol, glucagon, epinephrine, and growth
hormone referred to as counter regulatory hormones?
a. Decrease glucose production
b. Stimulate glucose output by the liver
c. Increase glucose transport into the cells
d. Independently regulate glucose level in the blood
12. What characterizes type 2 diabetes?
a. β-Cell exhaustion
b. Insulin resistance
c. Genetic predisposition
d. Altered production of adipokines
e. Inherited defect in insulin receptors
f. Inappropriate glucose production by the liver
13. Which laboratory results would indicate that the patient has prediabetes?
a. Glucose tolerance result of 132 mg/dL
b. Glucose tolerance result of 240 mg/dL
c. Fasting blood glucose result of 80 mg/dL
d. Fasting blood glucose result of 120 mg/dL
14. The nurse is teaching the patient with prediabetes ways to prevent or delay
the development of type 2 diabetes. What information should be included?
a. Maintain a healthy weight.
b. Exercise for 60 minutes each day.
c. Have blood pressure checked regularly.
d. Assess for visual changes on monthly basis
e. Monitor for polyuria, polyphagia, and polydipsia.
15. When teaching the patient with diabetes about insulin administration, the
nurse should include which instruction for the patient?
a. Pull back on the plunger after inserting the needle to check for blood.
b. Consistently use the same size of insulin syringe to avoid dosing errors.
c. Clean the skin at the injection site with an alcohol swab before each
injection.
d. Rotate injection sites from arms to thighs to abdomen with each injection
to prevent lipodystrophies.
16. A patient taking insulin has recorded fasting glucose levels above 200 mg/
dL (11.1 mmol/L) on awakening for the last five mornings. What should the
nurse advise the patient to do first?
a. Increase the evening insulin dose to prevent the dawn phenomenon.
b. Use a single-dose insulin regimen with an intermediate-acting insulin.
c. Monitor the glucose level at bedtime, between 2:00 am and 4:00 am,
and on arising.
d. Decrease the evening insulin dosage to prevent night hypoglycemia
and the Somogyi effect.
17. The nurse is assessing a newly admitted diabetic patient. Which observation
should be addressed as the priority by the nurse?
a. Bilateral numbness of both hands
b. Stage II pressure ulcer on the right heel
c. Rapid respirations with deep inspiration
d. Areas of lumps and dents on the abdomen
18. The nurse should observe the patient for symptoms of ketoacidosis when:
a. Illnesses causing nausea and vomiting lead to bicarbonate loss with
body fluids.
b. Glucose levels become so high that osmotic diuresis promotes fluid
and electrolyte loss.
c. An insulin deficit causes the body to metabolize large amounts of fatty
acids rather than glucose for energy.
d. The patient skips meals after taking insulin, leading to rapid metabolism
of glucose and breakdown of fats for energy.
19. What are manifestations of diabetic ketoacidosis (DKA)?
a. Thirst
b. Ketonuria
c. Dehydration
d. Metabolic acidosis
e. Kussmaul respirations
f. Sweet, fruity breath odor
20. What describes the primary difference in treatment for diabetic ketoacidosis
(DKA) and hyperosmolar hyperglycemic syndrome (HHS)?
a. DKA requires administration of bicarbonate to correct acidosis.
b. Potassium replacement is not necessary in management of HHS.
c. HHS requires greater fluid replacement to correct the dehydration.
d. Administration of glucose is withheld in HHS until the blood glucose
reaches a normal level.
21. A diabetic patient is found unconscious at home and a family member calls
the clinic. After determining that a glucometer is not available, what should
the nurse advise the family member to do?
a. Have the patient drink some orange juice.
b. Administer 10 U of regular insulin subcutaneously.
c. Call for an ambulance to transport the patient to a medical facility.
d. Administer glucagon 1 mg intramuscularly (IM) or subcutaneously.
22. The patient with diabetes is brought to the emergency department by his
family members, who say that he is not acting like himself and he is more
tired than usual. Number the nursing actions in the order of priority for this
patient.
a. Establish IV access.
b. Check blood glucose.
c. Ensure patent airway.
d. Begin continuous regular insulin drip.
e. Administer 0.9% NaCl solution at 1L/hr.
f. Establish time of last food and medication(s).
23. What disorders and diseases are related to macrovascular complications
of diabetes?
a. Chronic kidney disease
b. Coronary artery disease
c. Microaneurysms and destruction of retinal vessels
d. Ulceration and amputation of the lower extremitiese. Capillary and arteriole membrane thickening specific to diabetes
UNIT 6 MEDICAL PATHOLOGIES OF NEUROLOGICAL SYSTEM
Key Unit Competences
To take an appropriate decision on management of common pathologies ofNeurological system (Headache, Migraine, and Epilepsy)
Introductory activity 6.0
Carefully observe the picture below and answer the following questions:
Figure 6.1 Person with neurologic disorder
1. What are the abnormal observations can you recognize from this person?
2. What might be the pathologies that this person might be experiencing?
The nervous system is divided into two anatomic divisions: the central nervous
system (CNS) and the peripheral nervous system (PNS). The basic structure of the
nervous system is the nerve cell or neuron. Neurons are either sensory or motor.
Sensory neurons transmit impulses to the CNS; motor neurons transmit impulses
from the CNS. The nervous system consists of the brain, spinal cord, and peripheral
nerves. It is responsible for coordinating body functions and responding to changes
in or stimuli from the internal and external environment. Changes in the functioning
of the nervous system can profoundly affect the entire body.
Neurological disorders are diseases of the central and peripheral nervous system.
In other words, the brain, spinal cord, cranial nerves, peripheral nerves, nerve
roots, autonomic nervous system, neuromuscular junction, and muscles. Thesedisorders include epilepsy, Alzheimer disease and other dementias, cerebrovascular
diseases including stroke, migraine and other headache disorders, multiple
sclerosis, Parkinson’s disease, neuroinfections, brain tumours, traumatic disorders
of the nervous system due to head trauma, and neurological disorders as a result
of malnutrition. Examples of symptoms include paralysis, muscle weakness, poor
coordination, loss of sensation, seizures, confusion, pain and altered levels of
consciousness. The specific causes of neurological problems vary, but can include
genetic disorders, congenital abnormalities or disorders, infections, lifestyle or
environmental health problems including malnutrition, and brain injury, spinal cordinjury or nerve injury.
6.1 HEADACHE/CEPHALGIAS
Learning Activity 6.1
Carefully read the clinical case scenario and answer the followingquestions:
A 31-yr-old woman comes to the emergency department because of a severe
headache in the occipital region. She says the headache began suddenly about
1 h ago, and she describes it as “the worst headache of my life.” She says the
pain is constant and is accompanied by nausea but not vomiting. She deniesvisual symptoms, focal weakness, and problems with gait and balance.
She has frequently had similar headaches beginning about 2years ago. The
headaches have increased in frequency this past week, and this episode is by
far the worst. She says the headaches start suddenly, last about an hour, and
are associated with palpitations, unexplained anxiety, and light-headedness.
She has also had nausea and occasional swelling of the neck during these
episodes. The headaches are usually associated with exertion or with straining
during bowel movements but sometimes occur without any provocation. She
has not been evaluated for these headaches before. The woman who appears
uncomfortable because of headache, and her vital signs are temperature: 37.6°
C, pulse: 104 beats/min, BP: 150/90 mmHg, respiration rate: 20/min, oxygen
saturation of 99% on room air. She was given paracetamol 1gr TDS for 5 days,
advised to have rest for 4 days and CT scan was ordered.
1. What were abnormal signs and symptoms that the patient was presenting?
2. What might be some risk factors to the development of those symptoms?
3. What investigation was requested to lure out the cause of those symptoms?4. What was included into her plan of management?
Headache is among the most common reasons that patients seek medical
attention. A classification system developed by the International Headache Society
characterizes headache as primary or secondary.
Primary headaches are those in which headache and its associated features are
the disorder in itself. E.g. Migraine, Tension-type, exertional- type.
Secondary headaches are those caused by exogenous disorders. E.g. Systemic
infection, Head injury, Vascular disorders, Subarachnoid hemorrhage, Brain tumor.Causes, risk factors and pathophysiology
Headache pain results from signals interacting among the brain, blood vessels and
surrounding nerves. During a headache, an unknown mechanism activates specific
nerves that affect muscles and blood vessels. These nerves send pain signals tothe brain.
Migraines result when unstable nerve cells overreact to various factors (triggers).
The nerve cells send out impulses to blood vessels and cause chemical changes inthe brain. The result is disabling pain.
The patient who presents with a new, severe headache (acute, new-onset
headache) has a differential diagnosis that is quite different from the patient with
recurrent headaches over many years. In new-onset and severe headache, the
probability of finding a potentially serious cause is considerably greater than in
recurrent headache. Patients with recent onset of pain require prompt evaluation and
often treatment. Serious causes to be considered include meningitis, subarachnoid
hemorrhage, epidural or subdural hematoma, glaucoma, and purulent sinusitis.
Headaches have a tendency to run in families, especially migraines. Children who
have migraines usually have at least one parent who also suffers from them.
Headaches can also be triggered by environmental factors shared in a family’s
household, such as eating certain foods or ingredients (caffeine, alcohol, fermented
foods, chocolate and cheese, etc), exposure to allergens, secondhand smoke,
strong odors from household chemicals or perfumes. Common triggers of tension
headaches or migraines include alcohol use; dehydration, changes in eating or
sleeping patterns; depression; emotional stress related to family and friends, work
or school; excessive medication use; eye, neck or back strain caused by poor
posture; lighting; noise or weather changes.
Headaches in children: for about 20% of them, tension headaches and migraines
are a reoccurring problem. Similar to adults, triggers for headaches in children
include certain foods that trigger headaches for the individual, changes in sleep,environmental factors and stress.
The brain itself is not sensitive to pain, because it lacks pain receptors. However,
several areas of the head and neck have pain receptors and can thus sense pain.
These include the extracranial arteries, middle meningeal artery, large veins,
venous sinuses, cranial and spinal nerves, head and neck muscles, the meninges,
falx cerebri, parts of the brainstem, eyes, ears, teeth and lining of the mouth. Pial
arteries, rather than pial veins are responsible for pain production.
Headaches often result from traction to or irritation of the meninges and blood
vessels. The pain receptors may be stimulated by head trauma or tumors and
cause headaches. Blood vessel spasms, dilated blood vessels, inflammation or
infection of meninges and muscular tension can also stimulate pain receptors. Once
stimulated, a nociceptor sends a message up the length of the nerve fiber to the
nerve cells in the brain, signaling that a part of the body hurts. Primary headaches
are more difficult to understand than secondary headaches. The exact mechanisms
which cause migraines, tension headaches and cluster headaches are not known.
Migraines are currently thought to be caused by dysfunction of the nerves in thebrain.
Signs and symptoms
Headache signs and symptoms vary depending on the type of headache:
Tension headaches: tension headaches are the most common type of
headache. Tension headache pain tends to be consistent without throbbing, mild
to moderate, on both sides of the head (bilateral), responsive to over-the-counter
treatment, worse during routine activities (such as bending over or walking upstairs).
Migraines: migraines are the second most common type of primary headaches.
Symptoms of migraine include moderate to severe pain, nausea and vomiting,
pounding or throbbing pain, pain that lasts four hours to three days, sensitivity to
light, noise or odors, stomach upset or abdominal pain.
Cluster headaches: cluster headaches are the most severe type of primary
headache. Cluster headaches come in a group or cluster, usually in the spring or
fall. They occur one to eight times per day during a cluster period, which may last
two weeks to three months. The headaches may disappear completely (go into
remission) for months or years, only to recur later. The pain of a cluster headache
is intense with a burning or stabbing sensation, located behind one of your eyes or
in the eye region, without changing sides, throbbing or constant.
New daily persistent headaches: new daily persistent headaches (NDPH) come
on suddenly and last for more than three months. They typically occur in people
who weren’t having frequent headaches before. The pain of NDPH is constant and
persistent without easing up, located on both sides of the head, not responsive tomedications.
Sinus headaches: sinus headaches are the result of a sinus infection, which
causes congestion and inflammation in the sinuses (open passageways behind
the cheeks and forehead). People, and even healthcare providers, often mistake
migraines for sinus headaches. Symptoms of sinus headaches include bad taste
in mouth, deep, constant pain in your cheekbones and forehead, facial swelling,
feeling of fullness in ears, fever, pain that gets worse with sudden head movement
or straining, mucus discharge (snot).
Some headache symptoms that suggest a serious underlying disorder and that
require immediate medical care are those with a sudden, new, severe headache;
a headache that is associated with neurological symptoms such as weakness,
dizziness, sudden loss of balance or falling, numbness or tingling, paralysis,
speech difficulties, mental confusion, seizures, personality changes/inappropriate
behavior, or vision changes (blurry vision, double vision, or blind spots); headache
with a fever, shortness of breath, stiff neck, or rash; headache pain that awakens
you up at night; headaches with severe nausea and vomiting; headaches that occurafter a head injury or accident; getting a new type of headache after age 55.
Secondary headaches from: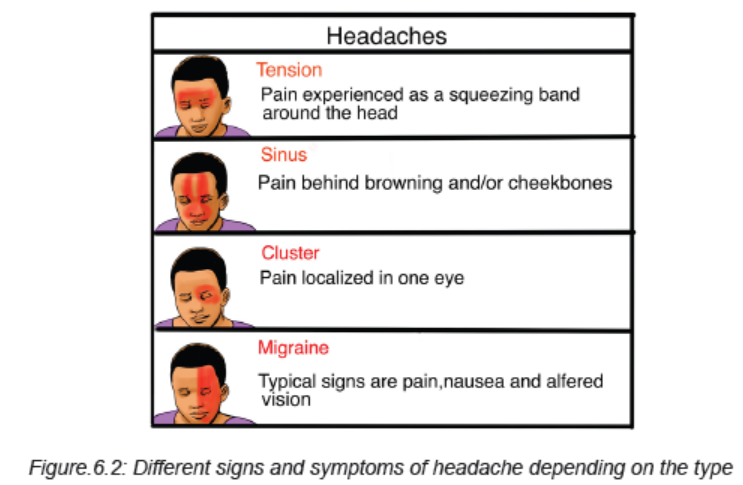
Meningitis: acute, severe headache with stiff neck and fever suggests meningitis.
Lumbar Puncture is mandatory. Often there is striking accentuation of pain with
eye movement. Meningitis can be easily mistaken for migraine in that the cardinal
symptoms of pulsative headache, photophobia, nausea, and vomiting are present.
Intracranial Hemorrhage: acute, severe headache with stiff neck but without fever
suggests subarachnoid hemorrhage. Rarely, if the hemorrhage is small or below the
foramen magnum, the head CT scan can be normal. Therefore, Lumbar Puncturemay be required to definitively diagnose subarachnoid hemorrhage.
Brain Tumor: approximately 30% of patients with brain tumors consider headache
to be their chief complaint. The head pain is usually an intermittent deep, dull aching
of moderate intensity, which may worsen with exertion or change in position and
may be associated with nausea and vomiting. The headache of brain tumor disturbs
sleep in about 10% of patients. A history of amenorrhea or galactorrhea should lead
one to question whether a prolactin-secreting pituitary adenoma is the source of
headache. Head pain appearing abruptly after bending, lifting, or coughing can be
due to a posterior fossa mass (or a Chiari malformation).
Temporal arteritis: head pain may be unilateral or bilateral and is located
temporally in 50% of patients but may involve any and all aspects of the cranium.
Pain usually appears gradually over a few hours before peak intensity is reached.
The quality of pain is only seldom agonizing; it is almost invariably described as dull
and boring, with superimposed episodic sharp pains similar to those that appear in
migraine. The pain is usually superficial, external to the skull, rather than originating
deep within the cranium. Scalp tenderness is present, often to a marked degree;
brushing the hair or resting the head on a pillow may be impossible because of
pain. Headache is usually worse at night and often aggravated by exposure to cold.
Glaucoma: glaucoma may present with a prostrating headache associated with
nausea and vomiting. The headache often starts with severe eye pain. On physicalexamination, the eye is often red with a fixed, moderately dilated pupil.
Investigations
Investigating headache might focus on:
Obtaining complete medical history and performing the holistic physical examination
where to look for signs and symptoms of an illness that may be causing the headacheand neurological examination and neurological tests.
Although scans and other imagining tests can be important when ruling out
other diseases, they do not help in diagnosing migraines, cluster or tension-type
headaches. However, if the healthcare provider thinks that the headaches are being
caused by another medical condition, there are several imaging tests that may be
done like a CT Scan or MRI (if headaches are connected to an issue with the central
nervous system. Both of these tests produce cross-sectional images of the brain
that can show any abnormal areas or problems). An EEG (electroencephalogram)may also be needed. Electromyography
Electromyography (EMG) studies the changes in the electrical potential of muscles
and the nerves supplying the muscles. An EMG is useful in determining the presenceof neuromuscular disorders.
Lumbar Puncture: changes in CSF occur in many neurologic disorders. A lumbar
puncture (spinal tap) is performed to obtain samples of CSF from the subarachnoid
space for laboratory examination and to measure CSF pressure. Bacteriologic tests
on specimens of CSF reveal the presence of pathogenic microorganisms. Strictaseptic technique is required during the procedure.
Other laboratory investigations might be helpful especially if there is high suspiciousof other underlying factors/causes.
Plan of treatment of headache
One of the most crucial aspect of treating headaches is figuring out the triggers,
and once the triggers are known, the treatment choices can be very easy. Triggers
are very specific to each person and once every patient determines his/her triggers,he/she can avoid or minimize them.
Counseling and stress management techniques can help the patient to handle
the triggers better. By lowering the stress level, patient can avoid stress-induced
headaches. Stress management teaches the patient ways to cope with stressful
situations. Relaxations technics are helpful in managing stress. Patient can use
deep breathing, muscle relaxation, mental images and music to ease the tension.
Biofeedback teaches the patient to recognize when tension is building in the
body. During biofeedback, sensors are connected to the body. They monitor the
involuntary physical responses to headaches, which include increases in breathingrate, pulse, heart rate, temperature, muscle tension, and brain activity.
Not every headache requires medication. Occasional tension headaches usually
respond well to NSAIDs (paracetamol, ibuprofen, etc), but be aware that using
these medications too often can lead to a long-term daily headache. For frequent orsevere headaches, the triptans and other types of drugs can stop a migraine attack.
Drugs for high blood pressure, seizures and depression can sometimes prevent
migraines. The healthcare provider may recommend trying one of these medicationsto reduce headache frequency.
6.2 MIGRAINE
Migraine headaches are chronic headaches that can be significant for hours or
even days. Symptoms can be very severe and it may be necessary to find a dark,
quiet place to lie down. It is usually an episodic headache that is associated with
certain features such as sensitivity to light, sound, or movement; nausea and
vomiting often accompany the headache. A useful description of migraine is a
benign and recurring syndrome of headache associated with other symptoms of
neurologic dysfunction in varying admixtures. Migraine can often be recognized byits activators, referred to as triggers.
Causes, risk factors and pathophysiology
Although many of the causes of migraines are not well understood, both genetic
and environmental factors appear to play a role. Many people with migraines have
a family history of migraines. If one or both parents have migraines, chances arethey will.
Whatever the mechanism of migraine, some of the following can trigger the migraine:
Hormonal changes in women: fluctuations in estrogen seem to cause headaches in
women known as migraines. Women with a history of migraines often get headaches
just before or during their periods, when they have high levels of estrogen. Others
tend to develop increased migraines during pregnancy or menopause. Hormonal
medications, such as birth control pills and hormone replacement therapy, can alsoworsen migraines, although some women find it beneficial.
Food: some migraines are triggered by certain foods. Common include wine, beer
and wine, cheese, chocolate; aspartame, overuse of caffeine, and processed foods.
Skipping meals or fasting can also trigger migraines. Stress at work or at home cantrigger migraines.
Feeling of stimulation: bright lights and the sun can trigger migraines, as can loud
sounds. Unusual odors including pleasant scents, such as perfume, and unpleasant
odors, such as paint and cigarette smoke, can also trigger migraines. Change
the sleep-wake cycle (either lack of sleep or too much sleep) can be a trigger formigraine attacks in some people.
Physical exertion, change the environment (changes in weather or barometricpressure) or medicines can trigger migraines or make migraines very worse.
Migraines can be caused by changes in the trigeminal nerve. An imbalance in brain
chemicals, including serotonin, may also be involved. Serotonin levels decrease
during migraines. This can trigger the trigeminal nervous system to release
substances called neuropeptides, which travel to the outer covering of the brain(meninges). The result is a headache.
The sensory sensitivity that is characteristic of migraine is probably due to
dysfunction of monoaminergic sensory control systems located in the brainstemand thalamus.
There is involvement of the neurotransmitter serotonin in migraine. The introduction
of serotonine agonist, methysergide was found as the first drug capable of preventingmigraine attacks.
Data also support a role for dopamine in the pathophysiology of certain subtypes
of migraine. Most migraine symptoms can be induced by dopaminergic stimulation.
Moreover, there is dopamine receptor hypersensitivity in migraineurs, as
demonstrated by the induction of yawning, nausea, vomiting, hypotension, and
other symptoms of a migraine attack by dopaminergic agonists at doses that do
not affect nonmigraineurs. Dopamine receptor antagonists are effective therapeutic
agents in migraine, especially when given parenterally or concurrently with otherantimigraine agents.
Migraine genes identified by studying families with familial hemiplegic migraine
(FHM) reveal involvement of ion channels (Ca++, Na+, K+) suggesting thatalterations in membrane excitability can predispose to migraine.
Signs and symptoms of Migraine
A typical migraine attack causes some or all of the following signs and
symptoms: moderate to severe headache, which may be limited to one side of
the head or may affect both sides, fluctuating headache, pain that gets worse
with physical activity, pain interferes with regular activities, nausea with or without
vomiting, sensitive to light (photophobia) and sound, lightheadedness, scalp
tenderness, visual disturbances (Photopsia), paresthesias, vertigo, alteration of
consciousness (syncope, seizures, confusional state) and sometimes diarrhea.
When left untreated, migraines typically last four to 72 hours, but how oftenheadaches occur vary from person to person.
Not all migraines are the same. Most people experience migraines without warning
signs. Some people have migraines with warning signs, formerly known as classic
migraines. The prodromal warning may include vision changes, such as seeingflashing lights or pins and needles feeling in the arms or legs.
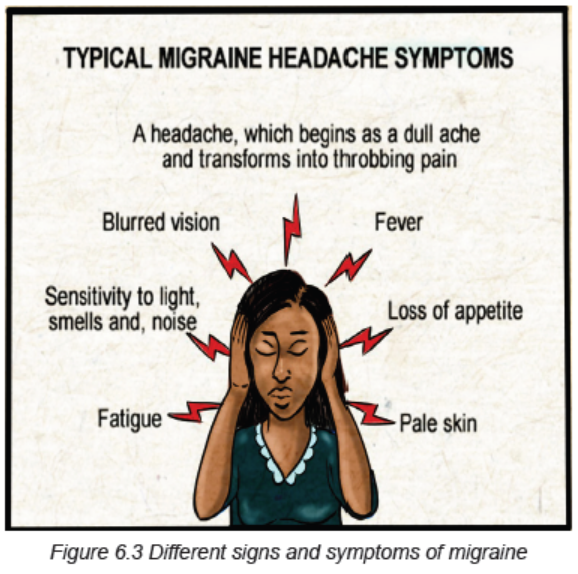
Stages of a migraine headache:
1. Prodrome: one or two days before a migraine, person might notice subtle
changes that warn of an upcoming migraine, including constipation, mood
changes from depression to euphoria, food cravings, neck stiffness, increased
thirst and urination or frequent yawning.
2. Aura: For some people, aura might occur before or during migraines. Auras are
reversible symptoms of the nervous system. They’re usually visual, but they
also can include other disturbances. Each symptom usually begins gradually,
builds up over several minutes and lasts 20 minutes to one hour. Examples of
auras include visual phenomena (such as seeing various shapes, bright spots or
flashes of light, etc), vision loss, pins-and-needles sensations in an arm or leg,
weakness or numbness in the face, or one side of the body, difficulty speaking,
hearing noises or music, and Uncontrollable jerking or other movements.
3. Attack: A migraine usually lasts from four to 72 hours if untreated, and the
frequency varies by the person. Migraines might occur rarely or strike several
times a month. During a migraine, patient might have pain (usually on one side
of the head, but often on both sides), pain that throbs or pulses, sensitivity to
light, sound, and sometimes smell and touch, nausea and vomiting.
4. Post-drome/recovery: after a migraine attack, patient might feel drained,
confused and washed out for up to a day. Some people report feeling elated.Sudden head movement might bring on pain again briefly.
Investigations
Diagnosis and confirmation of migraine starts from using the simplified diagnostic
criteria for Migraine (from Headache Classification Committee of the International
Headache Society):
• Repeated attacks of headache lasting 4–72 h in patients with a normal
physical examination, no other reasonable cause for the headache, and:
• At least 2 of the following features: Unilateral pain, Throbbing pain, Aggravation
by movement, Moderate or severe intensity.
• Plus at least 1 of the following features: Nausea/vomiting, Photophobia and
phonophobia
The migraine aura, consisting of visual disturbances with flashing lights or zigzag
lines moving across the visual field or of other neurologic symptoms, is reported in
only 20–25% of patients.
If migraines are typical or there is a family history of migraines, the doctor is likely
to diagnose the underlying problem based on the medical history and examination.
However, if the headache is unusual, severe, or unexpected, the doctor mayrecommend a series of tests to rule out other possible causes:
Computed tomography (CT): this helps the doctor diagnose tumors, infections, and
possibly other medical problems that can cause headaches.
Magnetic resonance imaging (MRI): using powerful radio waves, an MRI creates
a very detailed cross-section of the brain. MRI helps diagnose tumors, strokes,
aneurysms, neurological diseases, and other brain abnormalities. An MRI can also
be used to examine the blood vessels that supply the brain.
Lumbar puncture: if the doctor suspects an underlying problem, such as meningitis
and the cerebrospinal fluid that surrounds the brain and spinal cord, a lumbar
puncture may be ordered. During this procedure, a fine needle is inserted between
two vertebrae in the lower back to extract a sample of cerebrospinal fluid (CSF) for
laboratory investigations.EEG (electroencephalogram) might also be helpful.
Plan of treatment
Choosing a strategy for migraine management depends on the frequency and
severity of headaches, the extent of the disability causing the headache, and themedical problem. Treatment of migraine might focus on:
A. Analgesics
For best results, use a pain reliever as soon as you experience signs or symptomsof a migraine.
Non-steroidal anti-inflammatory drugs (NSAIDs): these medications, such
as ibuprofen, paracetamol or aspirin, can help relieve mild migraines. Medicines
marketed specifically for migraines, such as a combination of acetaminophen,
aspirin, and caffeine may also be helpful for moderate migraines but alone are
ineffective for severe migraine. If taken too often or for a long time, NSAIDs canlead to ulcers, gastrointestinal bleeding, and rebound headaches.
Triptans: for many people with severe migraine attacks, triptans are the drug of
choice. They are effective in reducing pain, nausea, and sensitivity to light and
sound associated with migraines. Medications include sumatriptan (Imitrex),
rizatriptan (Maxalt), naratriptan (Amerge), zolmitriptan (Zomig), almotriptan (Axert),
frovatriptan (Frova), and eletriptan (Relpax). Side effects of triptans include nausea,
dizziness, and muscle weakness. These medications are not recommended forpeople at risk of stroke and heart attack.
Serotonin agonists (Ergot): Ergotamine (Migergot, Cafergot) is less expensive,
but also less effective than triptans. It seems to be most effective for people with
pain that lasts more than 48 hours. Dihydroergotamine (Migranal) is a more effectiveergot derivative with fewer side effects than ergotamine.
Anti-nausea medication: because migraine attacks are often accompanied by
nausea with or without vomiting, the use of anti-nausea medications is appropriate
and is often combined with other medications. Frequently prescribed medications
are dopamine antagonists like metoclopramide (oral) or chlorpromazine (oral orsuppository).
Butalbital combination: drugs that combine the sedative butalbital with aspirin or
acetaminophen (Butapap, Phrenlin Forte) are sometimes used to treat migraine
attacks. Some combinations also include coffee or codeine (Esgic-Plus, Fioricet).
However, these drugs carry a high risk of headache symptoms returning whenstopped.
Narcotic drugs: especially codeine, are sometimes used to treat migraines when
triptans or ergot cannot be taken. Drugs form a habit and are often used only as alast resort.
B. Other medications that may be helpful in management of migraine:
Antidepressants: some antidepressants help prevent certain types of headaches,
including migraines. The most effective are tricyclic antidepressants, such as
amitriptyline, nortriptyline (Pamelor), and protriptyline (Vivactil). These medications
are considered first-line and can relieve migraines by affecting levels of serotonin
and other brain chemicals. Other types of antidepressants, called selective serotonin
reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors(SNRIs), have not been shown to be effective for prevention. migraine headache.
Antiepileptic drugs: some antiepileptic drugs, such as Divalproex (Depakote) and
topiramate (Topamax), and gabapentin (Neurontin), seem to reduce the frequency
of migraines. However, at high doses, antiepileptic drugs can cause side effectssuch as nausea and vomiting, diarrhea, abdominal pain, hair loss, and dizziness.
C. Lifestyle and remedy
Self-care measures can help relieve migraine pain:
Try muscle relaxation exercises: muscle relaxation, relaxation meditation, and yoga
do not require any equipment. They can be learned in the classroom or at home
using books or tapes. Or spend at least half an hour a day doing something relaxing- gardening, music, taking a hot bath or reading a book.
Get enough sleep but don’t oversleep: middle-aged adults need six to eight hoursof sleep a night. It is best to go to bed and wake up at the same time.
Rest and relax: if possible, rest in a quiet room in the dark when you feel a headache
coming on. Place an ice pack wrapped in a cloth on the back of the neck and applygentle pressure to the painful areas of the scalp.
Biofeedback: biofeedback seems to be particularly effective at reducing migraines.
This technique uses special relaxation equipment to teach how to monitor andcontrol certain responses related to stress, such as muscle tension.
Massage: massage can help reduce the frequency of migraines. And it can improvesleep quality, which can help prevent migraines.
Herbs, vitamins, and minerals: there is some evidence that herbs can prevent or
reduce migraine severity. High doses of riboflavin (vitamin B-2) may also preventmigraines by correcting small deficiencies in brain cells.
Lifestyle changes can help reduce the number and severity of migraines. One or
more of these suggestions may be helpful: to avoid triggers, exercise regularly,reduces the effects of estrogen.
Evolution and Complications
Migraine headaches are common and among the most disabling nonfatal conditions
of humankind. They are frequently misdiagnosed which can lead to under treatment.
Patients might also often self-diagnose and self-medicate resulting to inadequate
treatment. With adequate treatment, a patient’s condition and quality of life may
improve considerably. Patient education is extremely important to help patients
identify appropriate self-care measures such as identification of triggering events
and coping with chronic nature of their conditions. Treating health problems thatcause headaches, such as high blood pressure, can eliminate head pain.
If poorly managed, severe headache or migraine can lead to Status Migrainosus (a
relentless attack that lasts for more than 3 days, it can leave you feeling drained or
even disabled), Migrainous Infarction/stroke, where the blood vessel from brain get
narrowed and cut off the oxygen supply, Persistent Aura Without Infarction(patient
can have aura and symptoms like trouble breathing and numbness for months
or even years, the signs seem close to bleeding in the brain but without actualbleeding), Migraine-Triggered Seizure ( this is rare and look like epileptic seizure).
Migraines can also lead to other very serious health issues like depression and
anxiety, vertigo, sleeplessness/insomnia, nausea and vomiting, serotonin
syndrome (use of combined triptans and antidepressants can cause the
serotonin levels which can cause agitation, confusion, diarrhea, twitchy
muscles), stomach problems, rebound headache, etc. Migraines are
associated with a small increased risk of ischaemic strokes, and a very small
increased risk of mental health problems (depression, bipolar disorders,anxiety disorders, panic disorders, etc).
Self-assessment 6.1 and 6.2
1. Basing on signs and symptoms, differentiate different types of headache.
2. What are different risk factors of migraine?
3. What are the signs and symptoms of migraine?
4. What are different treatment options of migraine?
5. List 5 complications of migraine.
6.3 EPILEPSY
Learning Activity 6.3
Carefully read the clinical case scenario below and answer the followingquestions:
A 27 year-old woman was brought by her husband at the district hospital with
seizures. During the history taking, they revealed that patient had episode of
seizures even before and sometimes felt down. They also reported that at the
age of 20 she was experiencing multiple daily episodes of seizures and leftsided
face, arm and leg twitching with loss of consciousness and had multiple
hospitalizations. She has been receiving carbamazepine/tegretol 200mg BID for
the past 7 years but without improvement. She graduated from high school and
worked as a teacher in nearby primary school but was forced to quit due to herseizures.
At the hospital admission, the vital signs were BP of 124/65 mmHg, pulse rate
of 112 beats/ min, temperature of 36.7 degree Celsius, oxygen saturation of
96% on room air and was having hyper-salivation. The neurological examination
showed episodes of left facial twitching every 5 minutes. Her memory, orientation
to place, person and time were impaired. The patient was admitted in secured
room where she was alone and the care giver was instructed to be near the
patient and always turn the head to left and right side. She was placed on
injectable anti-epileptic drugs (phenobarbital inj 600mg to be given into 500ml
of NS 0.9%) to control her seizures, and was also given IV fluids (normal saline
1.5liters per 24 hours) for maintenance. The admitting doctor also ordered the
FBC, electrolytes, EEG and also brain CT scan.
1. Basing on case above, what are the abnormal signs and symptoms was
the patient presenting?
2. What do you think was the medical diagnosis that she had?3. What are the investigations requested to investigate that medical diagnosis?
4. What was included into her plan of management?
5. What do you think can happen to that woman if the condition was not wellmanaged or not responding to treatment?
Epilepsy is a central nervous system (neurological) disorder in which brain
activity becomes abnormal, and is a chronic non-communicable disease of the
brain characterized by recurrent seizures, which are brief episodes of involuntary
movement that may involve a part of the body (partial) or the entire body (generalized)
and are sometimes accompanied by loss of consciousness and control of bowel or
bladder function.
Seizure episodes are a result of excessive electrical discharges in a group of brain
cells. Different parts of the brain can be the site of such discharges. Seizures can
vary from the briefest lapses of attention or muscle jerks to severe and prolonged
convulsions. Seizures can also vary in frequency, from less than one per year
to several per day. One seizure does not signify epilepsy (up to 10% of people
worldwide have one seizure during their lifetime). Epilepsy is defined as having two
or more unprovoked seizures.
Seizures are sudden, explosive, disorderly discharge of cerebral neurons and are
characterized by a sudden, transient alteration in brain function, usually involving
motor, sensory and autonomic or psychic clinical manifestations and altered level
of arousal (awareness). There is a brief disruption in the brain electrical functions.
Convulsion, a term sometimes applied to seizures, refers to the jerky, contract-relax(tonic-clonic) movement associated with some seizures.
Causes, risk factors and pathophysiology
Epilepsy is not contagious. Although many underlying disease mechanisms can
lead to epilepsy, the cause of the disease is still unknown in about 50% of cases
globally. The causes of epilepsy are divided into the following categories: structural,
genetic, infectious, metabolic, immune and unknown. Examples include brain
damage from prenatal or perinatal causes (loss of oxygen or trauma during birth,
low birth weight, infection to the mother, poor nutrition, etc), congenital abnormalities
or genetic conditions with associated brain malformations or abnormalities (brain
tumors or vascular malformations such as arteriovenous malformations (AVMs)
and cavernous malformations, etc), a severe head injury, a stroke that restricts
the amount of oxygen to the brain, an infection of the brain (meningitis, viral
encephalitis or neurocysticercosis, some parasitic infections, etc), certain genetic
syndromes or some developmental disorders (like autism, dementia in older
adults), biochemical disorders (metabolic defects like hypoglycemia, hypocalcemia,drugs and alcohol abuse, etc) and a brain tumor.
There are two phenomenon in the pathophysiology of a seizure:
Hyper-excitability of a neuron: neuronal messages are transmitted by electrical
impulses called the Action Potential. This is actually a net positive inward ion flux
that leads to depolarization or voltage change in the neuronal membrane. The ions
involved include sodium, potassium, calcium and chloride. Normally brain tissues
prevent hyper excitability by several inhibitory mechanisms involving negative ions
like chloride ions. Disturbance in this normal excitability leads to hyper-excitability.
In this state there is increases excitatory transmission of impulses and decreases
inhibitory transmission. In addition there is alteration in the voltage gated ionic
channels. These ion channels normally open when the voltage difference across
the neuronal membrane is changed favorably. Once activated the impulses flow via
the neuronal circuits along the axons of the nerves. An action potential travels down
the axon to the terminal buttons and then releases neurotransmitters in the synapticcleft. This carries the action potential from one nerve to another.
Hyper synchronization: means that a hyper-excitable neuron leads to excessive
excitability of a large group of surrounding neurons. This means that when a large
electrical impulse is generated in one part of the brain from a focus of tissuesmillions of neurons in the brain fire excessively in addition bringing on a seizure.
In summary, the seizures develop into these mechanisms: excitation of a group
of nerves. This is caused by inward currents of Na, Ca and involvement of
excitatory neurotransmitters like Glutamate and Aspartate, too little inhibition, and
epileptogenesis (process whereby a previously normal brain is functionally altered
and biased towards the generation of the abnormal paroxysmal electrical activity
that defines chronic seizures) and hyperexcitability and hypersynchronization
of neurons that facilitates spread. There has to be abnormal synchronization which
is a property of a population of neurons to discharge together independently. Alone,a hyperexcitable neuron cannot generate a seizure.
Signs and symptoms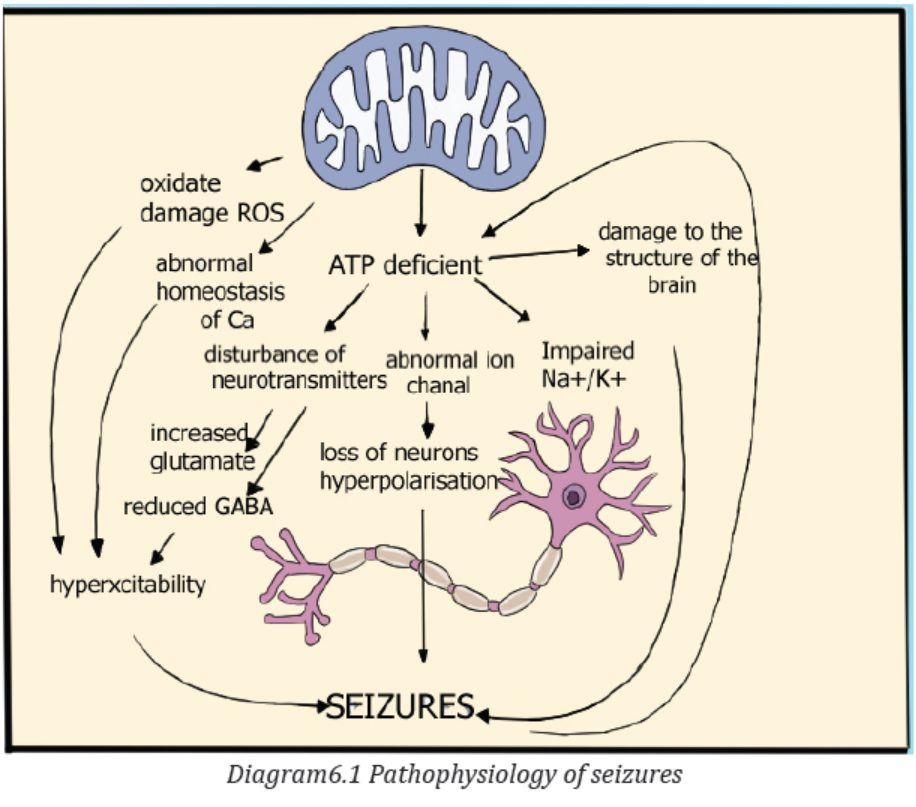
Because epilepsy is caused by abnormal activity in the brain, characteristics of
seizures vary and depend on where in the brain the disturbance first starts, and
how far it spreads. Temporary symptoms occur, such as loss of awareness or
consciousness, and disturbances of movement, sensation (including vision, hearing
and taste), mood, or other cognitive functions, temporary confusion, a staring spell,
stiff muscles, uncontrollable jerking movements of the arms and legs, psychologicalsymptoms such as fear, anxiety or déjà vu.
Signs and symptoms vary depending on the type of epilepsy/seizure. The seizures
are classified as either focal or generalized, based on how and where the abnormalbrain activity begins:
A. Partial/Focal seizures: when seizures appear to result from abnormal activity
in just one area of your brain, they’re called focal seizures. These seizures fallinto two categories:
• Focal seizures without loss of consciousness: also called simple partial
seizures, these seizures don›t cause a loss of consciousness. They may alter
emotions or change the way things look, smell, feel, taste or sound. Some
people experience deja vu. This type of seizure may also result in involuntary
jerking of one body part, such as an arm or leg, and spontaneous sensory
symptoms such as tingling, dizziness and flashing lights.
• Focal seizures with impaired awareness: also called complex partial
seizures, these seizures involve a change or loss of consciousness or
awareness. This type of seizure may seem like being in a dream. During a
focal seizure with impaired awareness, the patient may stare into space and
not respond normally to the environment or perform repetitive movements,
such as hand rubbing, chewing, swallowing or walking in circles. An important
additional subgroup comprises those seizures that begin as partial seizures
and then spread diffusely throughout the cortex, i.e., partial seizures withsecondary generalization.
Signs and symptoms of partial/focal seizures may be confused with other
neurological disorders, such as migraine, narcolepsy or mental illness. A thoroughexamination and testing are needed to distinguish epilepsy from other disorders.
B. Generalized seizures: these are the seizures that appear to involve all
areas of the brain are called generalized seizures. Six types of generalizedseizures exist:
• Absence seizures: absence seizures, previously known as petit mal seizures,
typically occur in children. They’re characterized by staring into space with or
without subtle body movements such as eye blinking or lip smacking and only
last between 5-10 seconds. These seizures may occur in clusters, happening
as often as 100 times per day, and cause a brief loss of awareness.
• Tonic seizures: tonic seizures cause stiff muscles and may affect
consciousness. These seizures usually affect muscles in your back, arms
and legs and may cause you to fall to the ground.
• Atonic seizures: atonic seizures, also known as drop seizures, cause a loss
of muscle control. Since this most often affects the legs, it often causes you
to suddenly collapse or fall down.
• Clonic seizures: clonic seizures are associated with repeated or rhythmic,
jerking muscle movements. These seizures usually affect the neck, face and
arms.
• Myoclonic seizures: myoclonic seizures usually appear as sudden brief
jerks or twitches and usually affect the upper body, arms and legs.
• Tonic-clonic seizures: tonic-clonic seizures, previously known as grand mal
seizures, are the most dramatic type of epileptic seizure. They can cause anabrupt loss of consciousness and body stiffening, twitching and shaking. They
sometimes cause loss of bladder control or biting your tongue. The tonic
clonic seizures develop into these different stages: prodromal (early clinical
manifestations such as malaise, headache, or a sense of depression, that
may occur hours to a few days before the onset of a seizure), aura (peculiar
sensation that immediately precedes the onset of generalized seizure and
may take the form of gustatory, visual or auditory experience or a feeling
of dizziness, numbness), tonic phase (tonic contraction of the muscles of
expiration and the larynx at the onset will produce a loud moan or “ictal cry”.
Respirations are impaired, secretions pool in the oropharynx, and cyanosis
develops. Contraction of the jaw muscles may cause biting of the tongue. A
marked enhancement of sympathetic tone leads to increases in heart rate,
blood pressure, and pupillary size. The duration of this phase ranges between
10 and 20 s. This is associated with loss of consciousness), clonic phase
(after 10-20 s, the tonic phase of the seizure typically evolves into the clonic
phase with alternation of contraction and relaxation of muscles. This phase
lasts no more than 1 min), the postictal (relaxation) phase (the time period
immediately following the cessation of seizure activity. It is characterized by
muscle relaxation (muscular flaccidity), and excessive salivation that can
cause stridorous breathing and partial airway obstruction). Bladder or bowel
incontinence may occur at this point. Patients gradually regain consciousness
over minutes to hours, and during this transition there is typically a period
of postictal confusion. Patients subsequently complain of headache, fatigue,and muscle ache that can last for many hours.
Investigations
To diagnose the epilepsy, there is need to review all the signs and symptoms andensure complete history taking and complete physical exam.
Several tests are used to diagnose epilepsy and determine the cause of the seizures:
A neurological exam: there is need of testing the behavior, motor abilities, mental
function and other areas to diagnose the condition and determine the type of
epilepsy the patients has. This exam included an assessment of motor skills (tested
by having the patient push and pull against the healthcare provider’s hands with his
or her arms and legs. The patient’s joints may also be checked simply by passive
and active movement) and sensory skills (the patient’s healthcare provider mayalso do a sensory test that checks his or her ability to feel.
This may be done by using different instruments: dull needles, tuning forks, alcohol
swabs, or other objects. The healthcare provider may touch the patient’s legs, arms,
or other parts of the body and have him or her identify the sensation (for example,
hot or cold, sharp or dull), balance and coordination (the patient may be asked to
walk normally or on a line on the floor. The patient may be instructed to tap his or herfingers or foot quickly or touch something, such as his or her nose with eyes closed.
Balance may be checked by assessing how the person stands and walks or having
the patient stand with his or her eyes closed while being gently pushed to one side
or the other), mental status (the patient’s level of awareness and interaction with
the environment may be assessed by conversing with the patient and establishinghis or her awareness of person, place, and time.
The person will also be observed for clear speech and making sense while talking.
This is usually done by the patient’s healthcare provider just by observing the
patient during normal interactions), reflexes (these are usually examined with the
use of a reflex hammer. The reflex hammer is used at different points on the body
to test numerous reflexes, which are noted by the movement that the hammer
causes), and functioning of the nerves (there are 12 main nerves of the brain, called
the cranial nerves. During a complete neurological exam, most of these nerves are
evaluated to help determine the functioning of the brain: Cranial nerve I (olfactory
nerve) is the nerve of smell, the patient may be asked to identify different smells
with his or her eyes closed. Cranial nerve II (optic nerve) this nerve carries visionto the brain.
A visual test may be given and the patient’s eye may be examined with a special
light. Cranial nerve III (oculomotor) is responsible for pupil size and certain
movements of the eye. The patient’s healthcare provider may examine the pupil
(the black part of the eye) with a light and have the patient follow the light in various
directions. Cranial nerve IV (trochlear nerve) helps with the movement of the eyes.
Cranial nerve V (trigeminal nerve) allows for many functions, including the ability
to feel the face, inside the mouth, and move the muscles involved with chewing.
The patient’s healthcare provider may touch the face at different areas and watch
the patient as he or she bites down. Cranial nerve VI (abducens nerve) helps with
the movement of the eyes. The patient may be asked to follow a light or finger to
move the eyes. Cranial nerve VII (facial nerve) is responsible for various functions,
including the movement of the face muscle and taste. The patient may be asked
to identify different tastes (sweet, sour, bitter), asked to smile, move the cheeks,
or show the teeth. Cranial nerve VIII (acoustic nerve) is the nerve of hearing. A
hearing test may be performed on the patient. Cranial nerve IX (glossopharyngeal
nerve) is involved with taste and swallowing. Once again, the patient may be asked
to identify different tastes on the back of the tongue. The gag reflex may be tested.
Cranial nerve X (vagus nerve) is mainly responsible for the ability to swallow, thegag reflex, some taste, and part of speech.
The patient may be asked to swallow and a tongue blade may be used to elicit the
gag response. Cranial nerve XI (accessory nerve) is involved in the movement of
the shoulders and neck. The patient may be asked to turn his or her head from
side to side against mild resistance, or to shrug the shoulders. Cranial nerve XII(hypoglossal nerve) is mainly responsible for movement of the tongue. The patient
may be instructed to stick out his or her tongue and speak). The extent of the
exam depends on many factors, including the initial problem that the patient isexperiencing, the age of the patient, and the condition of the patient.
Blood tests (FBC, renal and liver function tests, hormones dosages, lumbar
puncture to get CSF, ionograms, blood glucose, cultures, etc): helpful to check
for signs of infections, genetic conditions or other conditions that may be associatedwith seizures.
Electroencephalogram (EEG): this is the most common test used to diagnose
epilepsy. In this test, electrodes are attached to your scalp with a paste-like
substance or cap. The electrodes record the electrical activity of your brain. If the
patient has epilepsy, it’s common to have changes in your normal pattern of brain
waves, even when there is no seizure. The performer may monitor on video when
conducting an EEG while patient is awake or asleep, to record any seizures he/she
experiences. Recording the seizures may help to determine what kind of seizures
or rule out other conditions. The patient is given instructions to do something thatwill cause seizures, such as getting little sleep prior to the test, etc.
High-density EEG: in a variation of an EEG test, there may recommend highdensity
EEG, which spaces electrodes more closely than conventional EEG about
a half a centimeter apart. High-density EEG may help more precisely determinewhich areas of the brain are affected by seizures.
Computerized tomography (CT) scan: a CT scan uses X-rays to obtain crosssectional
images of the brain. CT scans can reveal abnormalities in the structure of
the brain that might be causing seizures, such as tumors, bleeding and cysts.
Magnetic resonance imaging (MRI): an MRI uses powerful magnets and radio
waves to create a detailed view of the brain. It is helpful to detect lesions or
abnormalities in the brain that could be causing seizures.
Functional MRI (fMRI): A functional MRI measures the changes in blood flow that
occur when specific parts of the brain are working. A fMRI is used before surgery to
identify the exact locations of critical functions, such as speech and movement, so
that surgeons can avoid injuring those places while operating.
Positron emission tomography (PET) Scans: PET scans use a small amount of
low-dose radioactive material that’s injected into a vein to help visualize metabolic
activity of the brain and detect abnormalities. Areas of the brain with low metabolism
may indicate where seizures occur.
Single-photon emission computerized tomography (SPECT): this type of test
is used primarily if an MRI and EEG that didn’t pinpoint the location in brain wherethe seizures are originating.
Neuropsychological tests: in these tests, doctors assess the thinking, memory
and speech skills. The test results help doctors determine which areas of the brain
are affected.
Plan of treatment
The treatment of epilepsy always starts from taking anti-epileptics medications,
and if these medications don’t treat the condition, there can be surgery or another
type of treatment. For better management of epilepsy, there is first need to treat the
cause if identified and provision of antiepileptic drugs.
A. Medications
Most people with epilepsy can become seizure-free by taking one anti-seizure
medication, which is also called anti-epileptic medication. Others may be able to
decrease the frequency and intensity of their seizures by taking a combination of
medications. The prescription starts from a single medication at a relatively low
dosage and may increase the dosage gradually until the seizures are well controlled.
At least half the people newly diagnosed with epilepsy will become seizure-freewhen properly taking first medication.
Monitoring of the patient and health education are keys because these medications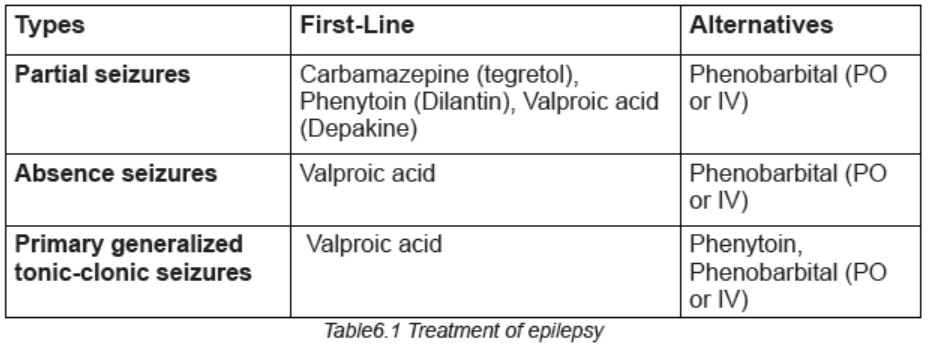
may have some side effects like fatigue, dizziness, weight gain, loss of bone density,skin rashes, loss of coordination, speech problems, memory and thinking problems.
B. Epilepsy surgery
When medications fail to provide adequate control over seizures, surgery may be
an option. With epilepsy surgery, a surgeon removes the area of the brain that is
causing seizures. Surgery is always performed when the tests show that seizures
originate in a small, well-defined area of the brain, the area in the brain to be
operated on doesn’t interfere with vital functions such as speech, language, motorfunction, vision or hearing.
For some types of epilepsy, minimally invasive approaches such as MRI-guided
stereotactic laser ablation may provide effective treatment when an open procedure
may be too risky. In these procedures, the surgeon direct a thermal laser probe at
the specific area in the brain causing seizures to destroy that tissue in an effort tobetter control the seizures.
C. Other therapies
Apart from medications and surgery, these potential therapies offer an alternativefor treating epilepsy:
Vagus nerve stimulation: in vagus nerve stimulation, a device called a vagus
nerve stimulator is implanted underneath the skin of your chest, similar to a heart
pacemaker. Wires from the stimulator are connected to the vagus nerve in the
neck. The battery-powered device sends bursts of electrical energy through thevagus nerve and to the brain.
Ketogenic diet: some children with epilepsy have been able to reduce their
seizures by following a strict diet that’s high in fats and low in carbohydrates. In this
diet, called a ketogenic diet, the body breaks down fats instead of carbohydrates
for energy. After a few years, some children may be able to stop the ketogenic dietand remain seizure-free.
Deep brain stimulation: in deep brain stimulation, surgeons implant electrodes into
a specific part of the brain, typically the thalamus. The electrodes are connected to
a generator implanted in the chest. The generator regularly sends electrical pulses
to the brain at timed intervals, and may reduce the seizures. Deep brain stimulationis often used for people whose seizures don’t get better with medication.
Responsive neurostimulation: these implantable, pacemaker-like devices can
help significantly reduce how often seizures occur. These responsive stimulation
devices analyze brain activity patterns to detect seizures as they start and deliveran electrical charge or drug to stop the seizure before it causes impairment.
D. Prevention of epilepsy
An estimated 25% of epilepsy cases are preventable through:
– Education (recognition of signs and symptoms of prodroma and aura, so that
the patient may avoid the fall in a very risk area i.e. fire, stairs…)
– Avoid driving, working with machinery, working at heights, swimming and
other activities that may cause serious injuries
– Psychosocial support (Counseling to minimize depression, anxiety due to
social stigmatization, lack of job, frequent hospitalization…)
– Preventing head injury is the most effective way to prevent post-traumaticepilepsy.
– Adequate perinatal care can reduce new cases of epilepsy caused by birth
injury.
– The use of drugs and other methods to lower the body temperature of a
feverish child can reduce the chance of febrile seizures.
– The prevention of epilepsy associated with stroke is focused on cardiovascular
risk factor reduction, e.g. measures to prevent or control high blood pressure,
diabetes and obesity, and the avoidance of tobacco and excessive alcohol
use.
– Central nervous system infections are common causes of epilepsy in tropical
areas, elimination of microorganisms/parasites in the environments and
education on how to avoid infections can be effective ways to reduce epilepsyworldwide.
Adequate medical diagnosis
Epilepsy is a type of neurological disorder known for causing seizures. These
seizures can be sporadic and occur without warning, or they might be chronic and
occur on a regular basis. Majority of epileptic patients require ongoing treatment toprevent seizures from disrupting their daily activities.
Treatment is one of the most important factors that affect the overall epilepsy
prognosis. Anti-seizures medications when taken on a regular basis, can help
control activity in the brain that leads to epileptic seizures. In turn, this helps to
also minimize risk factors and complications related to epilepsy. If not properly
managed, epilepsy leads to very life threatening complications. A great proportion
of the causes of death related to epilepsy are potentially preventable, such as falls,drowning, burns and prolonged seizures.
Evolution and complications
People with epilepsy tend to have more physical problems (such as fractures and
bruising from injuries related to seizures), as well as higher rates of psychological
conditions, including anxiety and depression. Similarly, the risk of premature death
in people with epilepsy is up to three times higher than in the general population.
The other complications related to epilepsy are drowning, car accidents,
pregnancy complications, emotional and psychological health issues problems,
especially depression, anxiety, and suicidal thoughts and behaviors. Other lifethreatening
complications of epilepsy that might occur are:
• Status epilepticus: this condition occurs if a patient is in a state of continuous
seizure activity lasting more than five minutes or if there is frequent recurrent
seizures without regaining full consciousness in between them. People with
status epilepticus have an increased risk of permanent brain damage anddeath.
• Sudden unexpected death in epilepsy (SUDEP): people with epilepsy
also have a small risk of sudden unexpected death. The cause is unknown
but may occur due to heart or respiratory conditions mainly to patients with
frequent tonic-clonic seizures or people whose seizures aren’t controlled ornot responding to medications.
Self-assessment 6.3
1. Differentiate the epilepsy to seizures
2. Basing on signs and symptoms, differentiate two major types of epilepsy
3. What are the mechanisms involved into pathophysiology of epilepsy
4. What are the examples of drugs used to treat different types of seizures?
6.4 END UNIT 6 ASSESSMENT
End unit assessment 6
SECTION A:SHORT ANSWER QUESTIONS
1. What are the elements of neurological diseases assessment?
2. Differentiate the headache to migraine.
3. What are the risk factors to develop the migraine?
4. Describe different treatment options of migraine.
5. Define epilepsy and differentiate epilepsy to seizures and convulsions.
6. Basing on signs and symptoms, differentiate two major types of epilepsy
7. List 5 different complications of epilepsy
8. What are the preventive strategies of epilepsy?
9. Describe the status epilepticus
SECTION B:MULTIPLE CHOICE QUESTIONS
1. Which type of headache is suspected when the headaches are unilateral
and throbbing, preceded by a prodrome of photophobia, and associated
with a family history of this type of headache?
a. Cluster
b. Migraine
c. Frontal-typed. Tension-type
2. A patient is diagnosed with cluster headaches. The nurse knows that
which characteristics are associated with this type of headache?
a. Family history
b. Alcohol is the only dietary trigger
c. Abrupt onset lasting 5 to 180 minutes
d. Severe, sharp, penetrating head pain
e. Bilateral pressure or tightness sensation
f. May be accompanied by unilateral ptosis or lacrimation
3. What is the most important method of diagnosing functional headaches?
a. CT scan
b. Electromyography (EMG)
c. Cerebral blood flow studies
d. Thorough history of the headache
4. The nurse is preparing to admit a newly diagnosed patient experiencing
tonic-clonic seizures. What could the registered nurse delegate to associate
nurse?
a. Complete the admission assessment.
b. Explain the call system to the patient.
c. Obtain the suction equipment from the supply cabinet.
d. Place a padded tongue blade on the wall above the patient’s bed.
5. How do generalized seizures differ from focal seizures?
a. Focal seizures are confined to one side of the brain and remain focal
in nature.
b. Generalized seizures result in loss of consciousness whereas focal
seizures do not.
c. Generalized seizures result in temporary residual deficits during the
postictal phase.
d. Generalized seizures have bilateral synchronous epileptic discharges
affecting the whole brain at onset of the seizure.
6. The patient is diagnosed with complex focal seizures. Which characteristics
are related to complex focal seizures?
a. Formerly known as grand mal seizure
b. Often accompanied by incontinence or tongue or cheek biting
c. Psychomotor seizures with repetitive behaviors and lip smacking
d. Altered memory, sexual sensations, and distortions of visual or auditorysensations
e. Loss of consciousness and stiffening of the body with subsequent
jerking of extremities
f. Often involves behavioral, emotional, and cognitive functions with
altered consciousness
7. Which type of seizure is most likely to cause death for the patient?
a. Subclinical seizures
b. Myoclonic seizures
c. Psychogenic seizures
d. Tonic-clonic status epilepticus
8. A patient admitted to the hospital following a generalized tonic-clonic
seizure asks the nurse what caused the seizure. What is the best response
by the nurse?
a. “So many factors can cause epilepsy that it is impossible to say what
caused your seizure.”
b. “Epilepsy is an inherited disorder. Does anyone else in your family have
a seizure disorder?”
c. “In seizures, some type of trigger causes sudden, abnormal bursts of
electrical brain activity.”
d. “Scar tissue in the brain alters the chemical balance, creating
uncontrolled electrical discharges.”
9. Following a generalized tonic-clonic seizure, the patient is tired and sleepy.
What care should the nurse provide?
a. Suction the patient before allowing him to rest.
b. Allow the patient to sleep as long as he feels sleepy.
c. Stimulate the patient to increase his level of consciousness.
d. Check the patient’s level of consciousness every 15 minutes for an
hour.
10. During the diagnosis and long-term management of a seizure disorder,
what should the nurse recognize as one of the major needs of the patient?
a. Managing the complicated drug regimen of seizure control
b. Coping with the effects of negative social attitudes toward epilepsy
c. Adjusting to the very restricted lifestyle required by a diagnosis of
epilepsy
d. Learning to minimize the effect of the condition in order to obtainemployment
REFERENCES
1. Barbara K. Timby; Nancy E. Smith. (2010). Introductory medical-surgical
nursing 10th Edition.
2. Daniel J Bonthius, Andrew D Hershey. (2022). Headache in children: Approach
to evaluation and general management strategies
3. Deborah J Wexler. (2022). Initial management of hyperglycemia in adults with
type 2 diabetes mellitus.
4. Deborah J Wexler. (2022). Overview of general medical care in nonpregnant
adults with diabetes mellitus
5. Diabetes mellitus, cases management, retrieved from
6. Epilepsy case management, retrieved from https://www.healthline.com/health/
epilepsy
7. Epilepsy case management, retrieved from https://www.mayoclinic.org/
diseases-conditions/epilepsy/symptoms-causes/syc-20350093
8. Epilepsy factsheets, retrieved from https://www.who.int/news-room/fact-sheets/
detail/epilepsy
9. Michael Cutrer. (2022). Pathophysiology, clinical manifestations, and diagnosis
of migraine in adults. Retrieved from https://www.uptodate.com/contents/
pathophysiology-clinical-manifestations-and-diagnosis-of-migraine-in-adul
ts?search=migraine&source=search_result&selectedTitle=2~150&usage_
type=default&display_rank=2
10. John Service, MD, (2000). Diabetes mellitus: Management and complications.
DOI: https://doi.org/10.1016/S0025-6196(12)61411-6
11. Frederick R Taylor. (2022). Tension-type headache in adults: Pathophysiology,
clinical features, and diagnosis. Retrived from https://www.uptodate.
com/contents/tension-type-headache-in-adults-pathophysiologyclinical-
features-and-diagnosis?search=headache&source=search_
result&selectedTitle=5~150&usage_type=default&display_rank=4
12. https://www.mayoclinic.org/diseases-conditions/diabetes/symptoms-causes/
syc-20371444
13. Introductory medical-surgical nursing by Barbara K. Timby and Nancy E. Smith
10th edition
14. Irl B Hirsch, Michael Emmett. (2020). Diabetic ketoacidosis and hyperosmolar
hyperglycemic state in adults: Clinical features, evaluation, and diagnosis
15. Irl B Hirsch, Michael Emmett. (2020). Diabetic ketoacidosis and hyperosmolar
hyperglycemic state in adults: Epidemiology and pathogenesis
16. Irl B Hirsch, Michael Emmett. (2022). Diabetic ketoacidosis and hyperosmolarhyperglycemic state in adults: Treatment
17. Lynne L Levitsky, Madhusmita Misra. (2022).Epidemiology, presentation, and
diagnosis of type 1 diabetes mellitus in children and adolescents
18. R Joshua Wootton, Franz J Wippold II, Mark A Whealy. (2021). Evaluation of
headache in adults.
19. Sharon L. Lewis, Shannon Ruff Dirken, Margaret McLean Heitkemper, L. B.
(2014). Medical-surgical nursing. Assessment and management of clinical
conditions.
20. Silvio E Inzucchi, Beatrice Lupsa. (2022). Clinical presentation, diagnosis, and
initial evaluation of diabetes mellitus in adults. Retrieved from From https://www.
uptodate.com/contents/clinical-presentation-diagnosis-and-initial-evaluationof-
diabetes-mellitus-in-adults?search=diabetes%20mellitus&source=search_
result&selectedTitle=1~150&usage_type=default&display_rank=1
21. Silvio E Inzucchi, Beatrice Lupsa. (2022). Clinical presentation, diagnosis, and
initial evaluation of diabetes mellitus in adults
22. Tina Shih. (2021). Seizures and epilepsy in older adults: Etiology, clinical
presentation, and diagnosis. Retrieved from https://www.uptodate.com/contents/
seizures-and-epilepsy-in-older-adults-etiology-clinical-presentation-and-diag
nosis?search=epilepsy&source=search_result&selectedTitle=9~150&usage_
type=default&display_rank=9
23. Todd J Schwedt, Ivan Garza. (2022). Acute treatment of migraine in adults. Retrived
rom https://www.uptodate.com/contents/acute-treatment-of-migraine-in-adu
lts?search=migraine&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
24. Todd J Schwedt, Ivan Garza. (2022). Preventive treatment of episodic migraine
in adults. Retrieved from https://www.uptodate.com/contents/preventivetreatment-
of-episodic-migraine-in-adults?search=migraine&source=search_
result&selectedTitle=3~150&usage_type=default&display_rank=3
25. Barbara K. Timby; Nancy E. Smith. (2010). Introductory medical-surgical
nursing 10th Edition.
26. CDC. (2021). Stroke. Retrieved from https://www.cdc.gov/stroke/facts.htm,
27. Christopher H Fanta, M. (2021). An overview of asthma management. Retrieved
from https://www.uptodate.com/contents/an-overview-of-asthma-managem
ent?search=asthma&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
28. Frederick E Barr, MD, M., & Barney S Graham, MD, P. (2011). Respiratory
syncytial virus infection: Treatment. Retrieved September 19, 2021, from
Respiratory syncytial virus infection: Treatment website: https://www.
uptodate.com/contents/respiratory-syncytial-virus-infection-treatment?se
arch=bronchiolitis&source=search_result&selectedTitle=8~150&usage_type=default&display_rank=8
29. Jamary Oliveira-Filho, M. T. M. (2021). Initial assessment and management
of acute stroke. Retrieved from https://www.uptodate.com/contents/initialassessment-
and-management-of-acute-stroke?search=stroke&source=sear
ch_result&selectedTitle=1~150&usage_type=default&display_rank=1
30. Jan Basile, M. J. B. (2021). Overview of hypertension in adults. Retrieved
from https://www.uptodate.com/contents/overview-of-hypertension-in-adults
?search=hypertension&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1,
31. Jose-Alberto Palma, H. K. (2021). Mechanisms, causes, and evaluation
of orthostatic hypotension. Retrieved from https://www.uptodate.com/
contents/mechanisms-causes-and-evaluation-of-orthostatic-hypotension?
search=hypotension&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
32. Julio A Ramirez, MD, F. (2021). Overview of community-acquired pneumonia
in adults. Retrieved from https://www.uptodate.com/contents/overview-ofcommunity-
acquired-pneumonia-in-adults?search=pneumonia&source=sear
ch_result&selectedTitle=3~150&usage_type=default&display_rank=3 on 22nd
September 2021
33. Louis R Caplan. (2020). Etiology, classification, and epidemiology of
stroke. Retrieved from https://www.uptodate.com/contents/etiologyclassification-
and-epidemiology-of-stroke?search=stroke&source=search_
result&selectedTitle=3~150&usage_type=default&display_rank=3,
34. Louis R Caplan. (2021). Clinical diagnosis of stroke subtypes. Retrieved
from https://www.uptodate.com/contents/clinical-diagnosis-of-stroke-subty
pes?search=stroke&source=search_result&selectedTitle=5~150&usage_
type=default&display_rank=5,
35. Mayo Clinic. (2021). Low Blood pressure/Hypotension. Retrieved from https://
www.mayoclinic.org/diseases-conditions/low-blood-pressure/symptomscauses/
syc-20355465#:~:text=What’s considered low blood pressure,pressure
is lower than normal.,
36. Michael Klompas, MD, M. (2021). Clinical evaluation and diagnostic testing
for community-acquired pneumonia in adults. Retrieved from https://www.
uptodate.com/contents/clinical-evaluation-and-diagnostic-testing-forcommunity-
acquired-pneumonia-in-adults?search=pneumonia&source=sear
ch_result&selectedTitle=1~150&usage_type=default&display_rank=1
37. Pedro A Piedra, M., & Ann R Stark, M. (2021). Bronchiolitis in infants and children:
Treatment, outcome, and prevention. Retrieved from https://www.uptodate.com/
contents/bronchiolitis-in-infants-and-children-treatment-outcome-and-preventi
on?search=bronchiolitis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 on 23rd September 2021
38. Sharon L. Lewis, Shannon Ruff Dirken, Margaret McLean Heitkemper, L. B.
(2014). Medical-surgical nursing. Assessment and management of clinical
conditions.
39. Sterns, R. H. (2020). Etiology, clinical manifestations, and diagnosis
of volume depletion in adults. Retrieved from https://www.uptodate.
com/contents/etiology-clinical-manifestations-and-diagnosis-of-volumedepletion-
in-adults?search=hypotension in adults&source=search_
result&selectedTitle=5~150&usage_type=default&display_rank=5
40. Talmadge E King, Jr, M. (2021a). Overview of bronchiolar disorders in
adults. Retrieved from https://www.uptodate.com/contents/overview-ofbronchiolar-
disorders-in-adults?search=bronchiolitis&source=search_
result&selectedTitle=3~150&usage_type=default&display_rank=3
41. Talmadge E King, Jr, M. (2021b). Respiratory bronchiolitis-associated interstitial
lung disease. Retrieved from https://www.uptodate.com/contents/respiratorybronchiolitis-
associated-interstitial-lung-disease?search=bronchiolitis&source
=search_result&selectedTitle=4~150&usage_type=default&display_rank=4 on
20th September 2021
42. WHO. (2021a). Hypertension. Retrieved from https://www.who.int/news-room/
fact-sheets/detail/hypertension
43. WHO. (2021b). Stroke/Cerebrovascular accident. Retrieved from http://www.
emro.who.int/health-topics/stroke-cerebrovascular-accident/index.html,
44. William J Barson, M. (2021). Pneumonia in children: Epidemiology, pathogenesis,
and etiology. Retrieved from https://www.uptodate.com/contents/pneumonia-inchildren-
epidemiology-pathogenesis-and-etiology?search=pneumonia&sourc
e=search_result&selectedTitle=10~150&usage_type=default&display_rank=6
on 22nd September 2021
45. Nader Shaikh, M., & Alejandro Hoberman, M. (2021). Urinary tract infections
in infants older than one month and young children: Acute management,
imaging, and prognosis. Retrieved from https://www.uptodate.com/contents/
urinary-tract-infections-in-infants-older-than-one-month-and-young-childrenacute-
management-imaging-and-prognosis?search=UTI&source=search_
result&selectedTitle=2~150&usage_type=default&display_rank=2
46. Thomas M Hooton, M. (2021). Acute simple cystitis in men. Retrieved from https://
www.uptodate.com/contents/acute-simple-cystitis-in-men?search=acute
simple cystitis&source=search_result&selectedTitle=2~150&usage_
type=default&display_rank=2
47. Alain Meyrier, M., & Thomas Fekete, M. (2021). Acute and chronic bacterial
prostatitis. Retrieved from https://www.uptodate.com/contents/acute-bacterialprostatitis?
search=acute and chronic bacterial prostatitis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
48. J Dennis Fortenberry, MD, M. (2021). Sexually transmitted infections:
Issues specific to adolescents. Retrieved from https://www.uptodate.
com/contents/sexually-transmitted-infections-issues-specific-toadolescents?
search=Sexually transmitted infections: Issues specific
to adolescents&source=search_result&selectedTitle=1~150&usage_
type=default&display_rank=1
49. Michel Pontari, M. (2021). Chronic prostatitis and chronic pelvic pain syndrome.
Retrieved from https://www.uptodate.com/contents/chronic-prostatitis-andchronic-
pelvic-pain-syndrome?search=chronic prostatitis&source=search_
result&selectedTitle=1~37&usage_type=default&display_rank=1
50. Thomas M Hooton, M., & Kalpana Gupta, MD, M. (2021). Acute complicated
urinary tract infection (including pyelonephritis) in adults. Retrieved from
https://www.uptodate.com/contents/acute-complicated-urinary-tractinfection-
including-pyelonephritis-in-adults?search=Acute complicated
urinary tract infection (including pyelonephritis) in adults&source=search_
result&selectedTitle=1~150&usage_type=default&display_rank=1
51. Barbara K. Timby; Nancy E. Smith. (2010). Introductory medical-surgical
nursing 10th Edition.
52. Sharon L. Lewis, Shannon Ruff Dirken, Margaret McLean Heitkemper, L. B.
(2014). Medical-surgical nursing. Assessment and management of clinical
conditions.
53. Charles B. Hicks, Meredith Clement. (2021). Syphilis: Epidemiology,
pathophysiology, clinical manifestations, treatment and monitoring.
54. Source: https://www.cdc.gov/std/gonorrhea/stdfact-gonorrhea.htm accessed
on 04th Novemebr,2021
55. Introductory medical-surgical nursing by Barbara K. Timby and Nancy E. Smith
10th edition P.889-892.
56. https://www.mayoclinic.org/diseases-conditions/hpv-infection/symptomscauses/
syc-20351596 accessed on 20th November,2021
57. https://en.wikipedia.org/wiki/Human_papillomavirus_infection#/media/
File:HPV_causing_cervical_cancer.jpg accessed on 19th November,2021
58. https://www.mayoclinic.org/diseases-conditions/chlamydia/diagnosistreatment/
drc-20
59. https://www.karger.com/Article/Abstract/348751
60. https://www.wikidoc.org/index.php/Chlamydia_infection_pathophysiology
61. https://my.clevelandclinic.org/health/diseases/4108-diarrhea visitedon17thOctober,2021.